

Improving Communication About Constipation in a Long-Term Care Setting by Using the Bristol Stool Scale
Abstract
The purpose of this pilot quality improvement project was to explore the feasibility of using the Bristol stool scale (BSS) to improve communication with long-term care (LTC) patients regarding constipation. After an in-service about the BSS, residents at a Veterans Affairs nursing home self-reported stool types to nurses. A nursing note template was changed in order for nurses to document BSS scores and interventions for constipation. The proportion of constipated patients decreased from 70% in the month at baseline (54 of 77 patients) to 27% in the month after the practice change (22 of 82 patients; P < .001). There were a total of 176 interventions (11.8% of 1487 bowel movements) done post- implementation. Routine use of the BSS was feasible in this project. Among nurses completing a satisfaction survey, most agreed that the BSS improved communication and helped to assess constipation. Further projects are needed to evaluate outcomes associated with using the BSS in a LTC setting.
Citation: Ann Longterm Care. 2016;24(7):25-29.
Received January 13, 2016; accepted March 9, 2016.
Introduction
Constipation has a negative impact on one’s quality of life and may affect overall wellbeing. The prevalence of constipation among nursing home (NH) residents is high, ranging from 44% to 80%.1-3 Constipation is typically characterized by infrequent bowel movements and subjective symptoms like abdominal discomfort, straining, and the sensation of incomplete evacuation.4 In clinical practice, constipation is typically defined as fewer than three bowel movements per week.5,6
There are many factors that may lead to the development of constipation, including lack of physical activity, decreased fluid intake, decline in functional and cognitive status, and side effects of medications.2,4 Increased fiber and fluid intake, added physical activity, and a toileting schedule can help to achieve regular bowel patterns. Additionally, laxatives and stool softeners are often prescribed for long-term care (LTC) residents to prevent and treat constipation. It is important for nursing staff to recognize the signs and symptoms of constipation and to quickly initiate treatment, as chronic constipation can lead to fecal impaction, fecal incontinence, hemorrhoids, anal fissures, and rectal prolapse.3,4
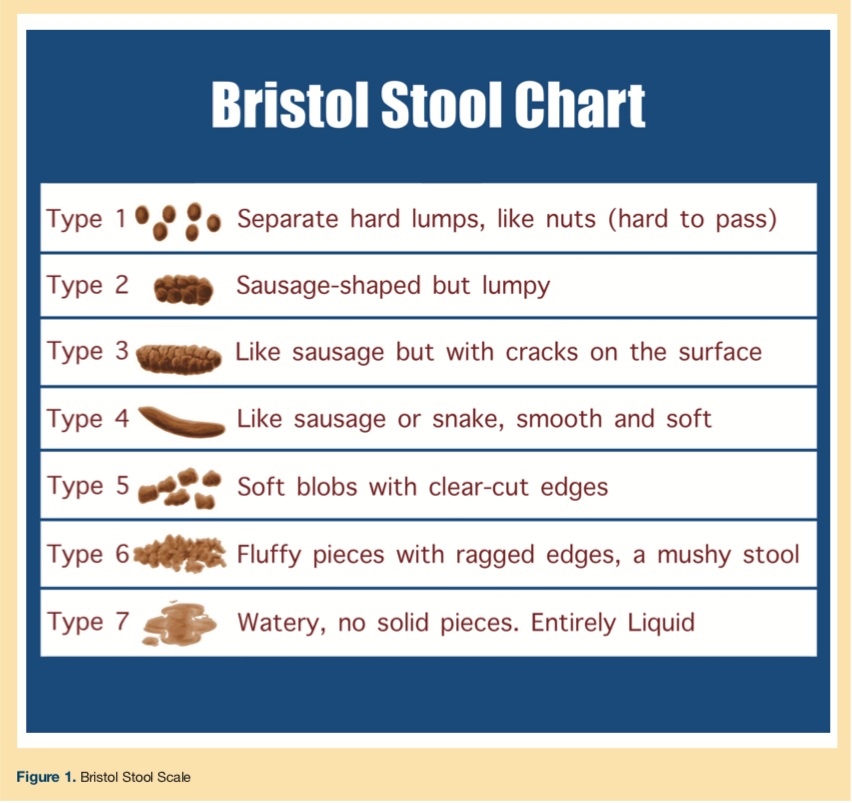
The Bristol stool scale (BSS) is a medical aid designed to classify stool forms into seven categories (Figure 1). It was developed in 1997 by Lewis and Heaton,7 who showed that change in stool form correlates with change in intestinal transit time. Intestinal transit time is of principal importance in gut physiology and is a major factor for bowel symptoms. Recently, the BSS has been applied to address a variety of research topics, including constipation in pediatrics, fecal incontinence in women during pregnancy, efficacy of bowel preparations for colonoscopy, and Clostridium difficile infections.8-12
At an 80-bed Veterans Affairs NH located in the southwestern region of the United States, a clinical pharmacist and dietician identified constipation as an area for improvement due to a lack of routine discussion with patients about constipation. The purpose of this pilot project was to explore the feasibility of using the BSS to improve communication about constipation with LTC residents. We hypothesized that use of the BSS to assess stool types and communicate with residents about constipation may help to decrease the prevalence of constipation in NHs.
Methods
Design and Setting
A pilot quality improvement (QI) project with a pre-post intervention design was conducted at a Veterans Affairs NH located in the southwestern region of the United States that includes a 20-bed hospice unit and 60 beds for rehabilitation and skilled nursing care. Unit nurse managers and the chief of geriatrics approved the project prior to initiation.
Project Implementation
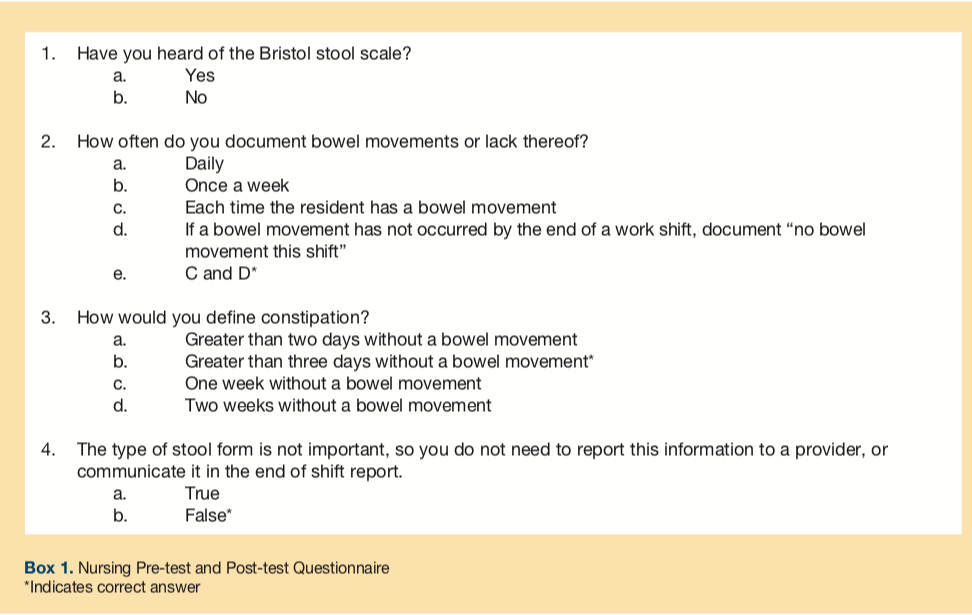
All patients admitted to the NH at any time during January 2015 were evaluated to determine a baseline prevalence of constipation. Constipation was defined as greater than 3 days without a bowel movement. During the month of February 2015, the BSS was incorporated into a nursing note template in the electronic medical record, and patients and health care professionals were informed about using the BSS to help evaluate constipation. BSS charts were printed and displayed at nursing workstations and patient bathrooms, and an in-service on the BSS and the project was given for nurses. Nurses completed a pre-test to measure their knowledge before the in-service (Box 1).
Use of the BSS began in March 2015. At the end of each shift, nurses documented: (1) whether patients had a bowel movement; (2) the BSS type; and (3) any interventions performed. Treatments available to be given to residents with constipation were as follows: encouraging increased fiber and fluid intake, offering medication for constipation as ordered, or requesting a new medication for constipation.
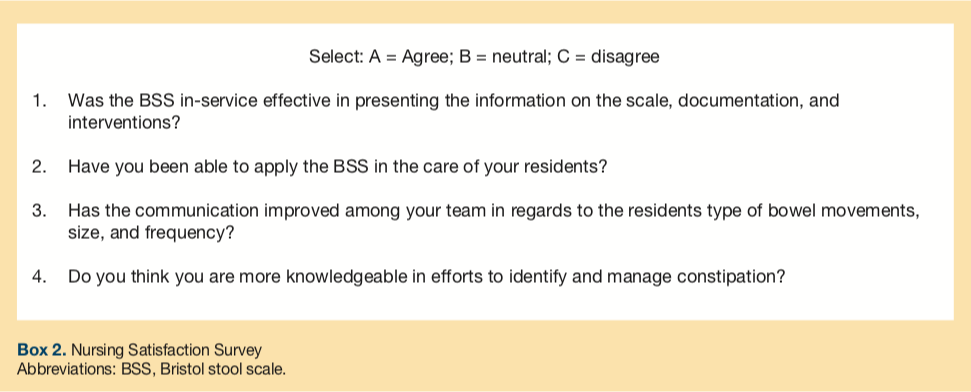
Post-implementation data was collected for March 2015 by chart review regarding the number of bowel movements, episodes of constipation, use of the BSS, and the number of interventions made. Nurses completed a post-test and a satisfaction survey mid-March after becoming familiar with the new process (Box 1, 2).
Statistical Analysis
A two-sample proportions test was used to compare the occurrence of constipation at baseline and post-implementation, as well as to assess changes in the rate of “correct” answers for the pre-test/post-test. Descriptive statistics were used to describe the results of the nursing satisfaction survey. Analyses were performed using SAS v9.2 (SAS Institute, Cary, NC). A significance level of P = .05 was assumed throughout.
Results
At baseline in January 2015, 70% of patients had an episode of constipation (54 episodes in 77 patients). In the month following initiation, the proportion of constipated patients decreased significantly to 27% (22 episodes in 82 patients; P < .001).
BSS scores were documented 88% of the time (1315 of 1487 bowel movements). Out of the 1487 bowel movements, there were a total of 176 interventions (11.8%) made for constipation post-implementation.
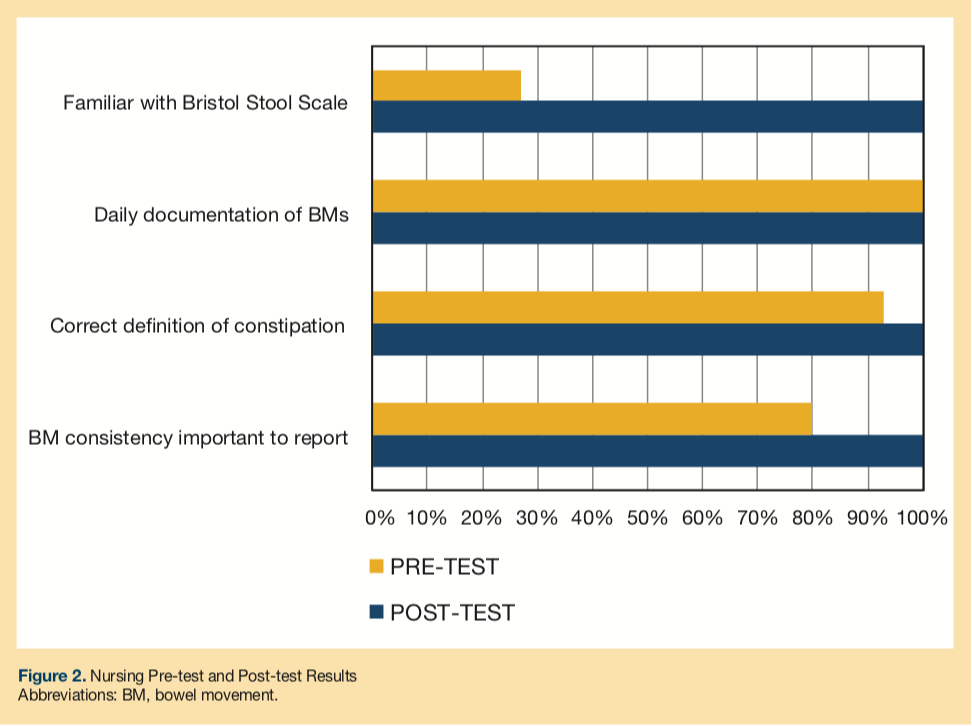
Prior to the in-service, the pre-test showed that only 27% of nurses (20 of 75) were familiar with the BSS (Figure 2). But nurses were aware of the definition of constipation and the procedure for documenting bowel movements or lack thereof. On Question 4, which measured the importance of stool form when assessing bowel movements, the proportion of “correct” answers increased from 80% on the pre-test (60 of 75) to 100% on the post-test (P < .001).
Among nurses completing the satisfaction survey, 82% felt the in-service was effective, 82% applied the BSS in care of their patients, 62% agreed it improved team communication, and 71% felt more knowledgeable about efforts to identify and manage constipation.
Discussion
There is a high prevalence of constipation in NHs, and it is important for nursing staff and providers to recognize constipation and initiate treatment in a timely manner. The baseline occurrence of constipation in this study population was similar to that reported from other studies.3-5 Documenting BSS scores as part of routine care improved communication between patients and health care professionals in this project. By creating a common language to describe stool types, nurses were able to offer treatments based on BSS scores.
The decreased occurrence of constipation from 70% to 27% represents an absolute risk reduction of 43%, which suggests an average of 1 out of 2.3 patients benefited from use of the BSS in this project. On the satisfaction survey, most nurses agreed that the BSS improved efforts to manage constipation.
While stool frequency is a common convention used by health care providers to define constipation, stool frequency is really a surrogate for outcomes that really matter such as unpleasant symptoms, pain, impaction, and fecal incontinence.
A major limitation of this QI project is that patient variables such as symptoms of constipation, age, medications, diet, fluid intake, and mobility were not evaluated. Thus, the change in constipation rate noted may be influenced by the type of patients in the NH. Baseline data regarding nursing interventions was not collected, so comparison with post-implementation data was not possible. A lack of blinding may have influenced the outcomes since nurses knew there was a new emphasis on treating constipation.
Future projects could improve upon the study design by using the same patients pre- and post-intervention or by using a control group. Over time, patients and/or nurses may become less diligent about discussing BSS results. Nurses already have to perform many tasks, so further projects are needed to see if the extra time devoted to documenting BSS scores is worthwhile in improving meaningful outcomes. Future in-service efforts may solicit ideas from staff regarding how to further enhance constipation detection and management in routine care.
Conclusion
For this project, using the BSS improved communication with LTC patients and helped nurses to assess constipation based on stool types. Further projects are needed to evaluate outcomes associated with using the BSS in LTC settings.
Affiliations, Disclosures, & Correspondence
Authors: Jagruti R Patel, RPh1; Angela S Chen, PharmD1; Nathan P Fewel, PharmD1; Eileen M Stock, PhD2,3
Affiliations:
1Central Texas Veterans Health Care System, Department of Veterans Affairs, Temple, TX
2Cooperative Studies Program Coordinating Center, Department of Veterans Affairs, Perry Point, MD
3Texas A&M Health Science Center, College of Medicine, Bryan, TX
Disclosures: The authors report no relevant financial relationships.
Acknowledgments: This work was completed with support from the Veterans Health Administration. The views are those of the authors and do not necessarily represent the views of the US Department of Veterans Affairs.
Correspondence:
Nathan Fewel
Central Texas Veterans Health Care System Pharmacy Service (119T)
Temple, TX 76504
Phone: (254) 743-2944
Fax: (254) 743-2202
Email: Nathan.Fewel@VA.gov
References
- Potter J, Wagg A. Management of bowel problems in older people: an update. Clin Med. 2005;5(3):289-295.
- Gallagher P, O’Mahony D. Constipation in old age. Best Pract Res Clin Gastroenterol. 2009;23(6):875-887.
- Fosnes GS, Lydersen S, Farup PG. Drugs and constipation in elderly in nursing homes: what is the relation? Gastroenterol Res Prac. 2012;2012:290231.
- Longstreth GF, Thompson WG, Chey WD, et al. Functional bowel disorders. Gastroenterology. 2006;130(5):1480-1491.
- Rao SS, Go JT. Update on the management of constipation in the elderly: new treatment options. Clin Interv Aging. 2010;5:163-171.
- Tariq SH. Constipation in long-term care. JAMDA. 2007;8(4):209-218.
- Lewis SJ, Heaton KW. Stool form scale as a useful guide to intestinal transit time. Scand J Gastroenterol. 1997;32(9):920-924.
- Muhammad S, Nawaz G, Jamil I, Ur Rehman A, Hussain I, Akhter S. Constipation in pediatric patients with lower urinary tract symptoms. J Coll Physicians Surg Pak. 2015;25(11):815-818.
- Parés D, Martinez-Franco E, Lorente N, Viguer J, Lopez-Negre JL, Mendez JR. Prevalence of fecal incontinence in women during pregnancy: a large cross-sectional study. Dis Colon Rectum. 2015;58(11):1098-1103.
- Malhotra A, Shah N, Depasquale J, Baddoura W, Spira R, Rector T. Use of Bristol stool form scale to predict the adequacy of bowel preparation-a prospective study. Colorectal Dis. 2015;18(2):200-204.
- Caroff DA, Edelstein PH, Hamilton K, Pegues DA, CDC Prevention Epicenters Program. The Bristol stool scale and its relationship to Clostridium difficile infection. J Clin Microbiol. 2014;52(9):3437-3439.
- Thabit AK, Nicolau DP. Lack of correlation between Bristol stool scale and quantitative bacterial load in Clostridium difficile infection. Infect Dis (Auckl). 2015;8:1-4.
