


Cost-Effectiveness of Pharmacist-led Interventions in Polypharmacy and Hospitalizations in Long-Term Care Facilities: A Systematic Review
Abstract
This article discusses the impact of pharmacist-led interventions on addressing polypharmacy-related issues in long-term care settings for older adults. The study aimed to evaluate cost savings associated with these interventions in terms of both medication and clinical costs. A literature search on PubMed identified 15 relevant studies. Out of the 13 studies focusing on medication outcomes, 12 demonstrated significant drug cost reductions ranging from $64.00 to $1,414.52 per resident annually, attributed to medication adjustments and discontinuations. Among the six studies addressing clinical outcomes, two indicated potential savings of $622.35 to $5,072.00 per patient by preventing hospitalizations, but without statistical significance. Common pharmacist interventions included medication reviews, physician-targeted recommendations, and deprescribing. This review highlights pharmacist-led interventions showed noteworthy cost reduction in medication expenses but lacked statistically significant evidence in reducing hospitalizations. These findings emphasize pharmacists' pivotal role in managing medications for long-term care residents, contributing to overall health care cost reduction.
Citation: Ann Longterm Care. 2023. Published online September 27, 2023.
DOI:10.25270/altc.2023.09.006
Adults aged age 65 and older who reside in long-term care (LTC) facilities, such as nursing homes, take more medications than any other age group due to multiple chronic health conditions and are therefore at a greater risk for inappropriate medication use.1 About 36% of older adults regularly take at least five different prescription drugs; among this population, 33% received one or more potentially inappropriate drugs.2 The US Centers for Medicare & Medicaid Services also noted that excessive use of medications in older adults is a major public problem that contributes to increased health care expenditure, adverse drug events, medication adherence issues, hospitalization, and mortality in older adults.3
Kaye and colleagues3 noted that on average, the US spends approximately $177.4 billion annually on polypharmacy, of which drug-related hospitalizations accounted for the majority. Two studies linked hospital readmissions in older patients to drug-related problems in 18% to 28% of cases.4,5 Another study revealed that older adults with polypharmacy have an increased risk for death (HR, 1.83; 95% CI, 1.51-2.21; P=<.001).6
Pharmacy expertise in medication management for older adults has an impact in combating polypharmacy through a variety of interventions, such as reducing inappropriate prescriptions, and reducing the number of doses taken and as a result, decreasing health care expenditure.7 The salary for an LTC pharmacist is estimated to be $103,000 to $123,000 annually, which should be considered when considering potential cost savings for the health care system.8
Research has demonstrated the usefulness of pharmacist-led interventions in addressing polypharmacy in older adults. This systematic review of the literature summarizes the cost-effectiveness of pharmacist-led interventions in LTC specifically on medication and hospitalization costs.
Methods
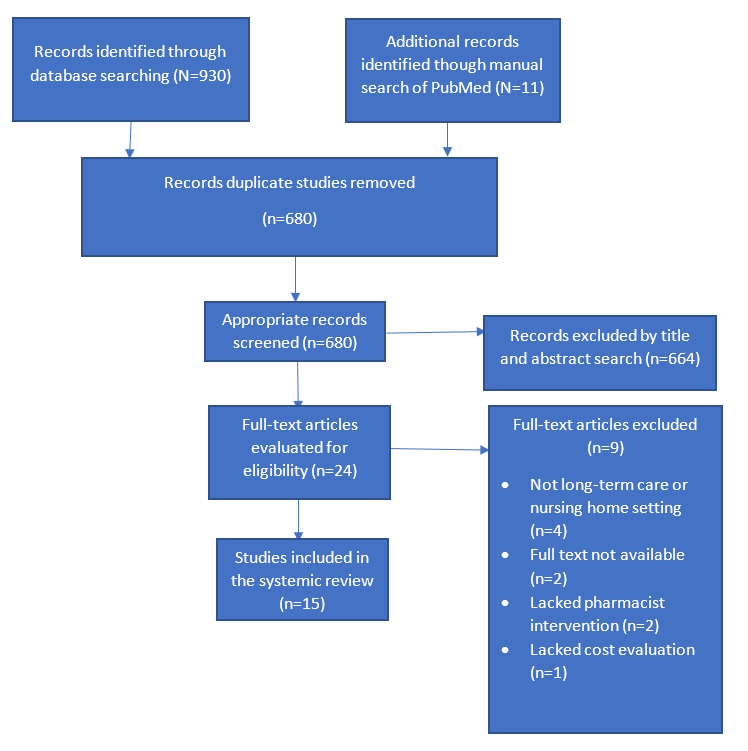
A search was performed in the PubMed database to identify articles that discussed polypharmacy, hospitalization, and cost in LTC and pharmacist-led interventions. The following keywords were used: cost effectiveness, older adults, pharmacist interventions, polypharmacy, hospitalization, and LTC facilities. A PRISMA flow diagram illustrates the study selection process (Figure). Articles were excluded if the focus of the study was not an LTC setting, did not include analysis of cost-effectiveness, or if it was a duplicate study. The articles included in the study were finalized after a full review of each study article. Of the 930 articles searched and reviewed, 915 were excluded, resulting in the evaluation of 15 articles for the systematic review.
Figure. Study Selection Process
The studies are heterogenous, including various types of pharmacist-led interventions and varying endpoints. Pharmacist-led interventions were categorized into three different activities: comprehensive medication review, deprescribing, and physician–pharmacist drug therapy recommendations. Deprescribing is defined as the process of discontinuing, reducing the dose, or slowly withdrawing medications that are inappropriate, unsafe, or ineffective.9 The cost-effectiveness outcomes were analyzed into two categories: medication outcomes and clinical outcomes. The medication outcome was defined as drug cost savings realized after unnecessary or inappropriate medications were discontinued or switched to other medications. Clinical outcome was described as the potential cost-saving benefits from hospitalization prevention, which would have occurred due to adverse drug events.
Results
Study Evaluation
Fifteen of 930 originally retrieved studies from PubMed were included in the final study review (Figure). Of the 15 articles, the most common study design was cohort studies (n=8) versus randomized controlled trials (n=7). Studies were primarily conducted in Europe (n=6), followed by the US (n=4), Australia (n=2), Singapore (n=2), and Canada (n=1).
A total of 18,618 residents were included in the review; the study population size ranged from 49 to 6344 residents. The age range was between 76.8 and 88 years, with a mean age of 81.1 years.
This systemic review did not use a health economist to evaluate the studies. The selected studies were direct and unencumbered, thus not necessitating a specialist. However, it should be noted that nuances from the studies may have been omitted.
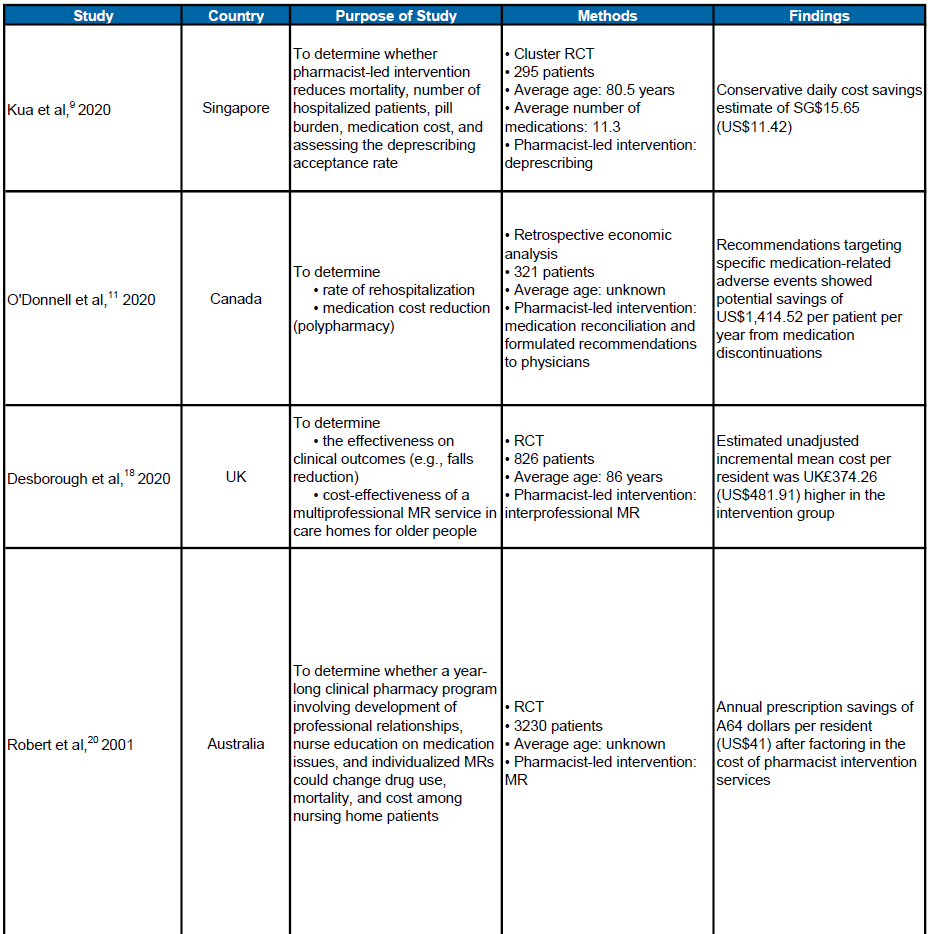
Medication Cost Outcome
Thirteen studies examined the cost-saving impact of a pharmacist-led intervention of nursing home resident medications (Table 1).10-22 Interventions included medication reviews and reconciliations, drug therapy recommendations to physicians and deprescribing unnecessary medications.10-22 Twelve studies reported a decrease in the number of unnecessary medications prescribed and a significant drug cost savings that ranged from $64 to $1,414.52 per resident per year.10-17,19-22 The most common drug cost savings interventions were characterized by discontinuation of medications, changing drug therapy, dose decrease, and switching to a lower-cost medications.10-22
Table 1. Overview of Studies Focused on Medication Cost Outcomes
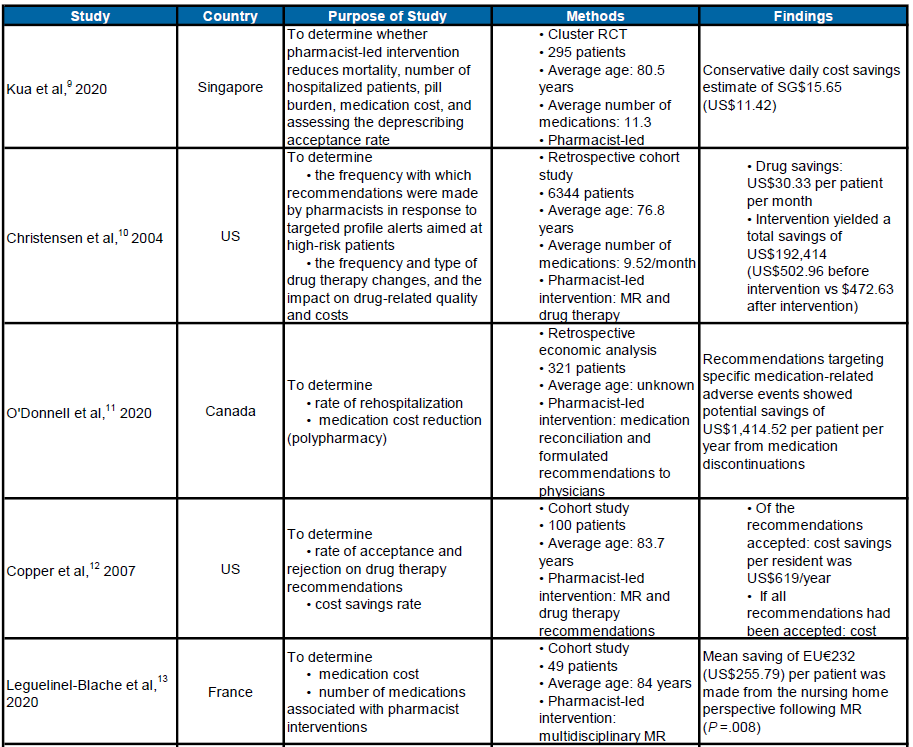
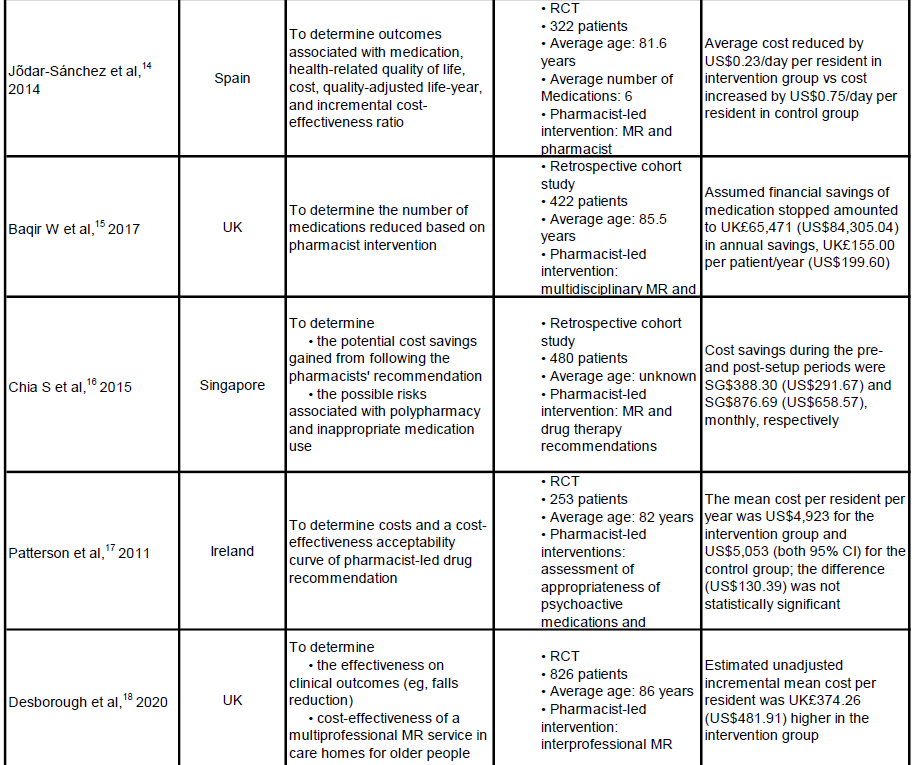
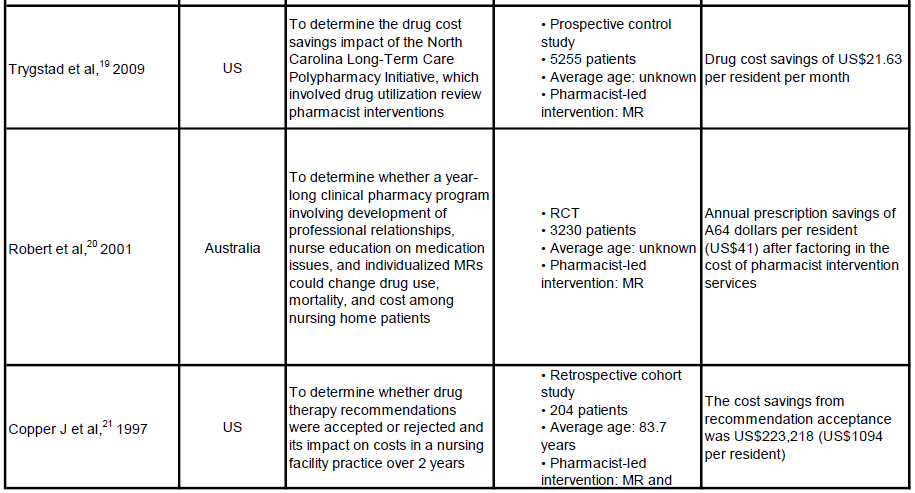
Abbreviations: MR, medication review; RCT, randomized controlled trial.
The most prevalent pharmacotherapy problems identified by the pharmacist that led to discontinuation of inappropriate medications (eg, medications that increased fall risk or caused an allergic reaction, constipation, hypoglycemia, or drug toxicity) were medications being used without indication, or inappropriate or suboptimal dose.10-22
Of note, two studies had unique findings that were positive but not statistically significant. Patterson and colleagues17 reported a mean total savings of $130.39 after assessment of appropriateness of psychoactive medications and medication changes with prescribers; however the findings were not statistically significant. Baqir and colleagues15 analyzed the difference between pharmacist-only review and pharmacist-plus-general-practitioner review and found out no statistically significant cost impact difference between a pharmacist-only and team-based care intervention in stopping inappropriate medications.
Clinical Cost Outcome
Six studies investigated the cost-effectiveness of pharmacist-led interventions in preventing hospitalizations (Table 2). In the studies, the following were identified as potential medication-related adverse events that were likely to result in hospitalizations but were prevented by pharmacist-led interventions11,15,19,23,24: falls resulting in osteoporotic fractures, renal failure, hypoglycemia, acute bleeding, thromboembolic events, and life-threatening arrhythmias. Two studies calculated a cost savings from hospitalization prevention per patient, however neither were significant.9,21 Other studies did not find an impact of pharmacist-led interventions or did not include monetary estimates.15,19,21,24 In fact, Desborough and colleagues18 found that the estimated unadjusted incremental mean cost per resident was UK£270.18 ($347.80) higher in the intervention group (after pharmacist intervention) compared with the control group (usual care).
Table 2. Overview of Studies Focused on Clinical Cost Outcomes
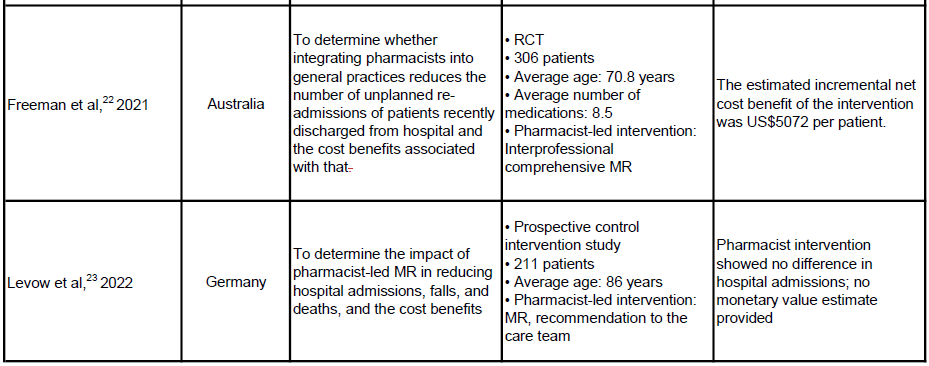
Abbreviations: MR, medication review; RCT, randomized controlled trial.
Discussion
This systematic review evaluated the cost savings associated with pharmacist-led reductions of polypharmacy and drug-induced hospitalizations in older adults residing in LTC and nursing home facilities. Studies found that the health care system can save up to $1,414.52 in medication cost per patient per year and $5,072 per patient in prevented hospitalization.9,22
Most studies (12 out of 13) that analyzed medication-related cost reported outcomes that were favored pharmacist-led interventions of medication review, deprescribing, and drug therapy recommendations to physicians.
Of the 6 studies that reviewed drug-induced hospitalization–related cost reduction, only two studies observed significant cost improvement. One study from the United Kingdom (UK), found the operating cost of a pharmacist was more expensive compared with the control (non-pharmacist intervention) in preventing hospitalizations. As noted in the study, UK physicians receive varying depths and breadths of pharmacologic training. To further confuse our understanding of UK physician knowledge base, schools lack assessment of graduates as prescribers. Ergo, UK physicians may be more adept, or less, than US physicians who receive very little pharmacology training.25
In addition, these findings are consistent with those of previous reviews that reported moderate financial advantages owing to pharmacist-led interventions related to medication costs.25,26 Given that older adults are twice as likely to be hospitalized compared with middle-aged adults due to a fragile health status that is not strictly drug-related, it is expected that pharmacist-led intervention had little effect on reducing hospitalization readmission and the subsequent cost.4
The results of this review highlight the importance of the pharmacist in LTC to improve cost-saving outcomes and the overall health outcomes of the patient. Discontinuing inappropriate medications increases medication adherence and reduces the risk of hospitalization and mortality associated with drug-related adverse reactions. This review also underscores the importance of multiprofessional care teams. Seven of the studies evaluated pharmacists who were part of a larger team-based care team and discovered that physicians were more likely to accept pharmacist drug therapy recommendations than when not on a team.13,16-19,23,24 Other favorable outcomes of multidisciplinary medication review included reduction in mortality and number of hospitalized residences and the overall better care management of the nursing home residents.17
Of note, the results of this review are based on cost estimates since it is impossible to ascertain the monetary value saved from hospitalizations that were prevented and medications that were discontinued following pharmacist intervention. Also, our study relied on one database (PubMed) for the identification of potentially eligible studies, and therefore some relevant studies may have been excluded in this systemic review. Finally, no universal validated checklists, such as the QUADAS and PRISMA, were used.27
Future economic evaluations with robust study design and methodology would be beneficial to investigate the cost-to-benefit of other pharmacist-led interventions (such as education, adherence and follow-up) and therefore determine the greatest cost savings interventions for health care budgets.
Conclusion
The findings of this study suggest that pharmacists play a key role in medication management of older adults as their interventions can reduce the use of potentially inappropriate medications, resulting in significant cost savings to the health care system. The patient care team should regularly employ pharmacists for medication reviews and reconciliations for all LTC patients. Additionally, pharmacists can and should provide training or continuing education sessions to all members of the LTC team to increase interprofessional awareness about pharmacists and the benefits that pharmacist-led interventions have for patient care and cost savings. To further emphasize and determine the specific cost-effectiveness of the pharmacist in LTC, a meta-analysis of the literature is needed. Including pharmacists in LTC benefits patients’ outcomes and will lead to cost savings, and the key will be integrating and using pharmacists’ expertise seamlessly into patient care.
Affiliations, Disclosures & Correspondence
Jackline Muia, PharmD, MS1 • Diane Calinski, PhD1
Affiliations:
1College of Pharmacy, Natural, and Health Sciences, Manchester University, Fort Wayne, IN
Disclosure:
The authors report no relevant financial relationships.
Address correspondence to:
Diane Calinski
16027 Diebold Rd., Fort Wayne, IN 46845
Phone (if applicable)260-470-2742
Email dmcalinski@manchester.edu
© 2023 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Annals of Long-Term Care or HMP Global, their employees, and affiliates.
References
Dagli RJ, Sharma A. Polypharmacy: A global risk factor for elderly people. J Int Oral Health. 2014;6(6):i-ii. PMID: 25628499; PMCID: PMC4295469.
Charlesworth CJ, Smit E, Lee DS, Alramadhan F, Odden MC. Polypharmacy among adults aged 65 years and older in the United States: 1988-2010. J Gerontol A Biol Sci Med Sci. 2015;70(8):989-995. doi:10.1093/gerona/glv013
Kaye HS, Harrington C, LaPlante MP. Long-term care: Who gets it, who provides it, who pays, and how much? Health (Millwood). 2010;29(1):11-21. doi:10.1377/hlthaff.2009.0535
Pereira F, Verloo H, Zhivko T, et al. Risk of 30-day hospital readmission associated with medical conditions and drug regimens of polymedicated, older inpatients discharged home: A registry-based cohort study. BMJ Open. 2021;11(7):e052755. doi:10.1136/bmjopen-2021-052755
Glans M, Kragh Ekstam A, Jakobsson U, Bondesson Å, Midlöv P. Medication-related hospital readmissions within 30 days of discharge-A retrospective study of risk factors in older adults. PLoS One. 2021;16(6):e0253024. doi:10.1371/journal.pone.0253024
Gómez C, Vega-Quiroga S, Bermejo-Pareja F, Medrano MJ, Louis ED, Benito-León J. Polypharmacy in the elderly: A marker of increased risk of mortality in a population-based prospective study (NEDICES). Gerontology. 2015;61(4):301-309. doi:10.1159/000365328
Chumney EC, Robinson LC. The effects of pharmacist interventions on patients with polypharmacy. Pharm Pract (Granada). 2006;4(3):103-109. PMID: 25247007; PMCID: PMC4156841.
Occupational Employment and Wages, May 2022. US Bureau of Labor Statistics. Updated April 25, 2023. Accessed July 21, 2023. https://www.bls.gov/oes/current/oes291051.html
Kua CH, Yeo CYY, Tan PC, et al. Association of deprescribing with reduction in mortality and hospitalization: a pragmatic stepped-wedge cluster-randomized controlled trial. J Am Med Dir Assoc. 2021;22(1):82-89:e3. doi:10.1016/j.jamda.2020.03.012
Christensen D, Trygstad T, Sullivan R, Garmise J, Wegner SE. A pharmacy management intervention for optimizing drug therapy for nursing home patients. Am J Geriatr Pharmacother. 2004;2(4):248-256. doi:10.1016/j.amjopharm.2004.12.002
O'Donnell D, Beaton C, Liang J, et al. Cost impact of a pharmacist-driven medication reconciliation program during transitions to long-term care and retirement homes. Healthc Q. 2020;23(3):34-40. doi:10.12927/hcq.2020.26335
Cooper JW, Wade WE, Cook CL, Burfield AH. Consultant pharmacist drug therapy recommendations acceptance and rejection from monthly drug regimen reviews in a geriatric nursing facility: Fourth year results and cost analysis. Hosp Pharm. 2007;42(8):729-736. doi:10.1310/hpj4208-729
Leguelinel-Blache G, Castelli C, Rolain J, et al. Impact of pharmacist-led multidisciplinary medication review on the safety and medication cost of the elderly people living in a nursing home: a before-after study. Expert Rev Pharmacoecon Outcomes Res. 2020;20(5):481-490. doi:10.1080/14737167.2020.1707082
Jõdar-Sánchez F, Martín JJ, Lõpez Del Amo MP, García L, Araújo-Santos JM, Epstein D. Cost-utility analysis of a pharmacotherapy follow-up for elderly nursing home residents in Spain. J Am Geriatr Soc. 2014;62(7):1272-1280. doi:10.1111/jgs.12890
Baqir W, Hughes J, Jones T, et al. Impact of medication review, within a shared decision-making framework, on deprescribing in people living in care homes. Eur J Hosp Pharm. 2017;24(1):30-33. doi:10.1136/ejhpharm-2016-000900
Chia HS, Ho JA, Lim BD. Pharmacist review and its impact on Singapore nursing homes. Singapore Med J. 2015;56(9):493-501. doi:10.11622/smedj.2015133
Patterson SM, Hughes CM, Cardwell C, Lapane KL, Murray AM, Crealey GE. A cluster randomized controlled trial of an adapted U.S. model of pharmaceutical care for nursing home residents in Northern Ireland (Fleetwood Northern Ireland study): A cost-effectiveness analysis. J Am Geriatr Soc. 2011;59(4):586-93. doi:10.1111/j.1532-5415.2011.03354.x
Desborough JA, Clark A, Houghton J, et al. Clinical and cost effectiveness of multi-professional medication reviews in care homes (CAREMED). Int J Pharm Pract. 2020;28(6):626-634. doi:10.1111/ijpp.12656
Trygstad TK, Christensen DB, Wegner SE, Sullivan R, Garmise JM. Analysis of the North Carolina long-term care polypharmacy initiative: A multiple-cohort approach using propensity-score matching for both evaluation and targeting. Clin Ther. 2009;31(9):2018-2037. doi:10.1016/j.clinthera.2009.09.006
Roberts MS, Stokes JA, King MA, et al. Outcomes of a randomized controlled trial of a clinical pharmacy intervention in 52 nursing homes. Br J Clin Pharmacol. 2001;51(3):257-265. doi:10.1046/j.1365-2125.2001.00347.x
Cooper JW Jr. Consultant pharmacist drug therapy recommendations from monthly drug regimen reviews in a geriatric nursing facility: a two-year study and cost analysis. J Nutr Health Aging. 1997;1(3):181-184. doi:10.1300/j055v06n01_03
Freeman CR, Scott IA, Hemming K, et al. Reducing Medical Admissions and Presentations Into Hospital through Optimising Medicines (REMAIN HOME): A stepped wedge, cluster randomised controlled trial. Med J Aust. 2021;214(5):212-217. doi:10.5694/mja2.50942
Lexow M, Wernecke K, Sultzer R, Bertsche T, Schiek S. Determine the impact of a structured pharmacist-led medication review - a controlled intervention study to optimise medication safety for residents in long-term care facilities. BMC Geriatr. 2022;22(1):307. doi:10.1186/s12877-022-03025-3
Hasan S, Thiruchelvam K, Kow CS, Ghori MU, Babar ZU. Economic evaluation of pharmacist-led medication reviews in residential aged care facilities. Expert Rev Pharmacoecon Outcomes Res. 2017;17(5):431-439. doi:10.1080/14737167.2017.1370376
Sadowski CA, Charrois TL, Sehn E, Chatterley T, Kim S. The role and impact of the pharmacist in long-term care settings: A systematic review. J Am Pharm Assoc (2003). 2020;60(3):516-524.e2. doi:10.1016/j.japh.2019.11.014
Page MJ, McKenzie JE, Bossuyt PM, et.al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
O'Shaughnessy L, Haq I, Maxwell S, Llewelyn M. Teaching of clinical pharmacology and therapeutics in UK medical schools: current status in 2009. Br J Clin Pharmacol. 2010;70(1):143-148. doi:10.1111/j.1365-2125.2010.03665.x
