


Homicide-Suicide in Long-Term Care: Risk Management Strategies for Providers
Abstract
Long-term care facilities have witnessed an increase in homicide-suicide occurrences across the United States. There is a lack of research about these tragic events in the long-term care setting and how facilities can implement meaningful changes and policies to prevent them. This report examines the interpersonal stressors and possible risk factors contributing to the perpetration of homicidal-suicidal acts in a nursing home setting and provides practical strategies to help facilities mitigate the risk of harm for residents, staff, and visitors.
Citation: Ann Longterm Care. 2021.
DOI: 10.25270/altc.2021.06.00005
Received October 28, 2020; accepted December 20, 2020. Published online June 28, 2021.
Introduction
In July 2019, an 82-year-old man shot and killed his 79-year-old wife, a resident of a Wilmington, Delaware, skilled nursing facility (SNF). Witnesses reported seeing him enter the facility, locate his wife in the common area, and shoot her once before turning the gun on himself.1 In the Upper Peninsula of Michigan, a husband and wife were found dead outside her nursing home (NH) in Sault Ste. Marie, Michigan.2 One month later, a husband and wife died in a homicide-suicide in Carmichael, California, where the wife resided in an assisted living facility because of her advanced dementia.3 On March 8, 2020, a 90-year-old man shot and killed his 79-year-old wife, a resident of an SNF in Texas City, Texas.4 In Sacramento, California, an NH resident was killed by her husband.5 The facility had been closed to visitors because of COVID-19.
The above examples represent several recent instances of homicide-suicide among older adults, with deaths occurring between intimate partners, including husbands and their wives. Homicide-suicide is defined as the completion of at least one homicide followed by the suicide of the perpetrator. Homicide-suicide deaths have disproportionately affected older couples, with most cases involving female victims and male perpetrators, as compared with other victim-perpetrator relationships.6 Although the frequency of these acts occurs less often than suicide or homicide alone, the impact to the community and social networks is significant and garners much attention in the media.7 However, research focusing on the etiology of homicide-suicide in long-term care (LTC) has been limited, primarily as a consequence of a lack of understanding of the stressors involved in the acts of these crimes.
We examine the interpersonal and situational stressors as well as possible risk factors contributing to the perpetration of homicidal-suicidal acts in the NH setting. We provide practical strategies to help facilities mitigate the risk of harm for residents, staff, and visitors.
Prevalence of Homicide-Suicide Among Older Adults in the United States
Homicide-suicide occurs infrequently, with an estimated annual rate of 0.22 per 100,000 people in the United States, or 4% of annual homicides and 1.5% of annual suicides; however, it is a terrible tragedy for the victims’ friends, family, and community members, with far-reaching repercussions.8 Although older adults comprise 12% of the US population, they account for 18% of all deaths by suicide.9 Since 1998, the homicide-suicide rate among couples aged 55 years and older in Florida has increased 10-fold.10 Spousal homicide-suicide events by adults aged 55 years and older account for one-third of all homicide-suicides in the United States, with older adult men accounting for 51% of the perpetrators. Women have been recognized as the perpetrators in only 14% of these cases.11
In her work published in 2000, Donna Cohen, PhD, identified three types of spousal/consortial homicide-suicides in older adults that are believed to comprise approximately 15% of the total: dependent-protective; aggressive and symbiotic. The common link to all three typologies is the belief on the part of the perpetrator, usually a male, that there is an unacceptable threat to the relationship.12 In circumstance involving the placement of the female spouse in a care facility, the male may feel control over the life of his partner, his ability to protect her or the financial pressures that arise from her placement. There may be additional factors including the burden of his own health, depression-related issues from years of being a caregiver, isolation, lack of purpose, and hopelessness. Dr Cohen notes that the aggressive form of murder-suicide is more frequently seen in young-old couples involving a history of threatening behaviors. The third type, symbiotic, is characterized by extraordinary dependency, multiple comorbidity in one or both of the spouses which prompt the male to perform a “mercy killing” of the female.12
The Violence Policy Center estimates that 11 murder-suicides occur each week in the United States and that more than 1200 Americans die each year. Nearly two-thirds involve intimate partners, the majority of which involved a firearm. Twenty-three percent of murder-suicides involved people aged 55 years or older. In 2017, 18% of homicides involved a perpetrator older than 55 years, however, 36% of all suicide victims were in this age group.13
Interpersonal Stressors Contributing to Homicide-Suicide Risk in LTC
Cognitive decline, the increased burden of physical illness, lack of social networks, and the increasing cost of care have been identified as catalysts for these fatal exchanges. Below, we explore some of these contributing stressors in more detail.
Forced Separation
Most homicide-suicides in older adults are associated with the development of physical illness in the perpetrator as well as a significant decline in the spouse. Approximately half of all the homicide-suicide cases arising in older adults are circumstances in which the older husband was the caregiver for a wife with a disability.14 These illnesses may be the catalyst for the older spouse to commit the crime, particularly if the wife is institutionalized and the husband is experiencing grief, loss, loneliness, desperation, financial pressures, loss of self, or any combination of these factors. The forced separation caused by the admission of one’s spouse to an assisted living or SNF is often a precipitating factor in accelerating the stress when the community-dwelling spouse is unable to physically care for his wife and views this inability to manage the care as a “failure” to fulfill the marital vows of “in sickness and in health.”
Presence of Depression and Other Comorbidities
Malphurs and Cohen15 assessed the causative factors and characteristics involved in older adult homicide-suicides by comparing the characteristics of men who committed suicide vs those who committed homicide-suicide. They noted that preexisting and untreated depression were identified in both groups; however, a history of domestic violence was reported with greater frequency (25% vs 5%) in homicide-suicide perpetrators compared with those who committed suicide. The husbands who committed homicide-suicide experienced recent changes in their own health status before the act.
Furthermore, in their 2010 study, Bourget and colleagues11 performed a retrospective analysis of domestic homicides in Quebec, Canada, from 1992 to 2007 that identified 27 cases in which homicide was committed by an individual aged 65 years or older. Their findings note that 11 of the 13 fatal homicide-suicide cases (85%) involved homicide-suicide perpetrated by men aged 65 to 78 years. The study concluded that, because the overwhelming proportion of victims had preexisting medical conditions at the time the offense was committed, the husband caregivers of chronically ill wives were at high risk for depression or a sense of hopelessness that may precipitate the act. The Bourget study suggested that older male caregivers with untreated depression who provide caregiving tasks for a spouse with a chronic illness or disability should trigger a higher index of suspicion for their potential to inflict severe harm.
Media Attention
Salari16 identified a potential causal connection when homicide-suicides occur in a particular geographical location. This may be an effect of media attention on the individual or a sense that such actions validate feelings of hopelessness in which death may be the only logical solution to the trauma of aging and infirmity. Zimmerman and Fridel17 cited many studies that address the role of media attention in inducing moral panic when a homicide-suicide occurs in a specific geographical location. The impact of this crime has far-reaching effects for the community and raises pertinent issues regarding the degree of social support and how the transition for both of the spouses could be meaningfully improved.17
Interventions for LTC Facilities
Watch for the “Four Ds”
LTC staff should watch for “The Four Ds,” which are primary risk factors in older adults, whether they reside in a facility or in the community:
- Depression
- Debility
- Access to deadly means
- Disconnectedness from society
Depression
LTC facilities commonly perform assessments for mood and depression symptomatology through the social services designee using the Patient Health Questionnaire-9 scale contained within the Minimum Data Set.18 Unfortunately, these assessments are focused exclusively on the individual who was admitted to the facility and do not include the individual who placed the resident in the facility. The social history of the resident must include an understanding of how and why placement occurred, what interventions had been attempted in the community to support the individual, the pressures placed on the community-dwelling spouse, and whether the spouse has sufficient support in the community, both socially and financially.
Debility
Malphurs and colleagues14 note the importance in identifying the stressors of caregiving and the caregiver’s own health issues as risk factors. As previously noted, according to Cohen, in situations where a male spouse is placing a female spouse in a care facility, the male may feel the need to control the life of his partner, an inability to protect her, or he could be strained by the financial pressures that that come with placement. He perceives there is a threat to the relationship due to placement. Additional stressful factors may include the burden of his own health, caregiver-related depression, real or perceived feelings of isolation, lack of purpose, and hopelessness.12
Access to deadly means
Older adults have the highest rates of suicide by a firearm, and a higher percentage of older adults own a gun—27% compared with 16% of those aged 18 to 25 years; therefore, access to deadly means is more common among older adults.19 States with higher rates of gun ownership have been associated with higher suicide rates as a consequence of the degree of proximity to a firearm.20
Disconnectedness from society
The community-dwelling spouse may experience intense feelings of disconnectedness with the placement of their spouse in LTC. For example, the husband’s abilities to cook, maintain the residence, and manage the finances may be significantly limited if these functions were primarily the responsibility of the wife, further compounding the community-dwelling spouse’s sense of loss.
Discuss the Decision for LTC With the Community-Dwelling Spouse
The complex emotions involved in agreeing to the placement of a spouse are frequently overlooked, because the primary focus on admission is the resident. The pressures placed on the community-dwelling spouse by the primary care provider or the hospital discharge planner are generally not discussed at the time of admission. Instead, the focus tends to be on the admission process, determinations of code status, the selection of a funeral home, and a host of other decisions.
The decision to place a spouse in LTC may be associated with significant feelings of guilt and inadequacy. Pressure from family members, primary care providers, hospitalists, or discharge planners to place the disabled spouse may have a significant negative effect on the community-dwelling spouse, an issue that may be evident on admission or arise during the course of the residency.
In addition, the financial impact of LTC on the spouse and their children, if any, should be acknowledged and discussed as part of the decision. The average out-of-pocket cost for a month of LTC services in 2016 was $6844.21 The cost of institutional health care services is prohibitive for many families, especially if the need extends for a protracted period. Support and resources for families, as well as an understanding of the impact (and perceived stigma) of taking charity money or money from a government program should be realistically discussed within a framework of understanding the government’s role in reimbursing LTC services.
LTC staff should have an understanding of the potential trauma associated with institutional placement of a loved one or companion, and they should attempt to ascertain how the spouse is handling the placement and their beliefs regarding the permanency of the residency. Asking the community-dwelling spouse the following questions (or ascertaining answers indirectly, depending upon the issue/situation) may help:
- What social supports are available in your community?
- Is there a trusted friend or family member who is in contact with you?
- Does the staff feel you are better able to care for your spouse than the NH staff?
- Do you believe your spouse would be happier if they were no longer living?
- Do you believe your spouse’s care is futile?
- Is there an overwhelming concern about payment for the residency?
- Have there been instances of homicide-suicide in this geographical area that have been publicized by the media?
- Does the community-dwelling spouse have a history of drug or alcohol issues or impaired problem-solving behaviors?
- Are depressive symptoms evident in the community-dwelling spouse?
Does the community-dwelling spouse acknowledge depression? Has he/she sought treatment? (NH staff should be attuned to statements such as “I am too old to still be living” or “She/he would be better off dead” as indicators of depression or suicidal or homicidal ideation.)
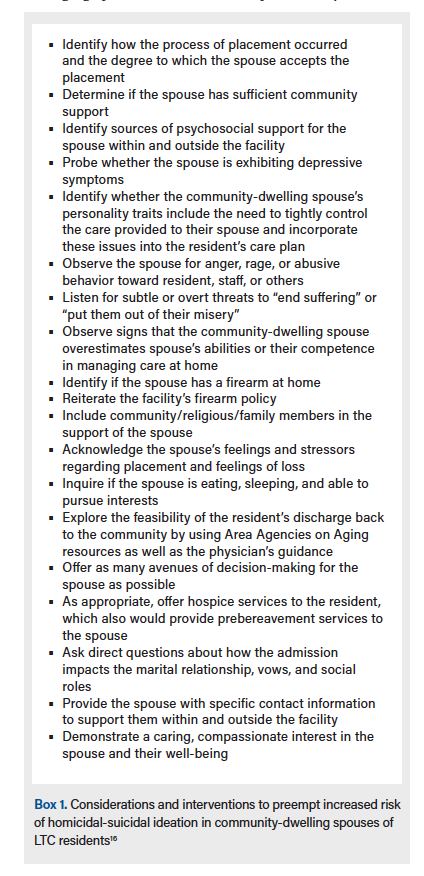
In addition to these questions, Salari16 identified areas of consideration within the husband-wife dyad that may help LTC staff monitor and address possible homicide-suicide ideology (Box 1).
Providing Access to Support
It is vital to appreciate the dynamic between the older adult and their spouse residing in LTC. Providing counseling and support that focuses beyond the needs of the resident to those of the spouse will be crucial in identifying the potential for harm. Such support can be provided in the following ways:
- Form a spousal support group at the facility, in which common feelings of loss and isolation can be discussed.
- Include the spouse at mealtime and explore other avenues from inclusion to encourage feelings of empowerment.
- Encourage the spouse to attend to their own health needs.
- Help the spouse determine ways to maintain connections with outside groups of friends, family, neighbors, and other social groups.
Strengthening the Spouse’s Role in Care
Research examining the adjustment to LTC suggests that adopting a model where family members remain involved in the care of their loved one may be beneficial. Zimmerman and colleagues, for example, implemented a randomized trial to evaluate a group intervention aimed at reducing staff burden and improving family and resident outcomes.22 The purpose was to assist families in creating meaningful roles for themselves in LTC communities as well as to improve family-staff relationships. Over a 6-month span, families and staff provided data regarding family involvement, family and staff well-being and attitudes, and resident quality of life. Intervention individuals participated in workshops and created service plans to identify family roles. Study results suggest that the intervention was correlated with decreased caregiver/family burden and improved quality of life for residents. In addition, decreased burnout and improved partnership with families were reported by staff members. These findings illustrate the importance of engaging family members in resident care to offset feelings of loss and to improve adjustment to LTC.
Consider a Facility-Wide Policy to Ban Weapons
The overarching requirement for all care facilities is the protection and safety of the residents living in the community. There is no constitutional amendment preventing LTC facilities, continuing care retirement communities, or assisted living facilities from developing and implementing policies to prohibit weapons on their campuses. The United States’ Second Amendment applies to an individual’s right to bear arms; however, this applies to individuals and not to private entities. Private businesses, including LTC facilities, are not governed by the Second Amendment, allowing entities to create and implement a weapons ban.23 Although facilities may accept federal funds through Medicare and Medicaid, an NH is still considered a private entity. Because the laws vary from state to state, facilities should verify concealed carry and open carry regulations, as well as laws requiring permits for individuals who possess firearms, specifically regarding storage in apartments or in vehicles located in the facility’s parking lot.
Conclusion
Placing a loved one in an assisted living facility or an NH is a significant source of distress for residents and their families. The decision to admit an older adult to an institution is often traumatic, particularly for a community-dwelling male spouse. It is vital that LTC providers have a clear grasp of the coping mechanisms of residents, spouses, and other family members, as well as an appreciation of the stressors involved in placement. Prevention of homicide-suicides requires an understanding of the far-reaching impact of spousal separation due to illness, coupled with providing access to resources that are available to support individuals in the community.
Affiliations, Disclosures, & Correspondence
Authors: Ilene Warner-Maron, PhD, RN-BC, NHA1 • Katherine E Galluzzi, DO, CMD, FACOFP dist2 • Anna Zacharcenko, PsyD3
Affiliations:
1Department of Geriatrics and Palliative Medicine, Philadelphia College of Osteopathic Medicine, Philadelphia, PA
2Department of Geriatrics and Palliative Medicine, Philadelphia College of Osteopathic Medicine, Philadelphia, PA
3Department of Clinical Psychology, School of Professional Psychology, Philadelphia College of Osteopathic Medicine, Philadelphia, PA
Disclosures:
Authors report no relevant financial relationships.
Address correspondence to:
Ilene Warner-Maron, PhD, RN-BC, NHA
Department of Geriatrics and Palliative Medicine
Philadelphia College of Osteopathic Medicine
4170 City Avenue
Philadelphia, PA 19131
Phone: (215) 871-6371
Fax: (215) 871-6374
Email: Ilenewa@pcom.edu
References
1. Sharp A, Kuang J, Holveck. Woman, 79, and man, 82, dead after shooting at ManorCare nursing home near Wilmington. The News J. July 20, 2019. Updated July 21, 2019. Accessed February 28, 2021. https://www.delawareonline.com/story/news/local/2019/07/20/breaking-police-respond-shooting-manorcare-nursing-home/1786050001/
2. Sault Ste. Marie police investigate murder-suicide. 9and10news.com. July 11, 2019.Accessed February 28, 2021. https://www.9and10news.com/2019/07/11/sault-ste-marie-police-investigating-murder-suicide/
3. Associated Press. 2 dead in apparent murder-suicide at Carmichael care home. The Press Democrat. August 7, 2019. Accessed February 28, 2021. https://www.pressdemocrat.com/article/news/2-dead-in-apparent-murder-suicide-at-carmichael-care-home/
4. Gill J. Elderly couple dead in apparent murder-suicide in Texas City nursing home. Houston Chronicle. March 8, 2020. Accessed February 28, 2021. https://www.houstonchronicle.com/news/houston-texas/houston/article/Elderly-couple-dead-in-apparent-murder-suicide-in-15115649.php
5. Sheriff’s department investigating murder-suicide at nursing home. CBS Sacramento YouTube page. May 27, 2020. Accessed February 28, 2021. https://www.youtube.com/watch?v=y04P1rqQIp4
6. Reckdenwald A, Simone S. Injury patterns for homicide followed by suicide by the relationship between victims and offenders. Homicide Studies. 2006;21:111-132. doi:10.1177/1088767916671350
7. Schwab-Reese LM, Peek-Asa C. Factors contributing to homicide-suicide: differences between firearm and non-firearm deaths. J Behav Med. 2019;42:681-690.
8. Large, M, Smith G, Nielssen O. The epidemiology of homicide followed by suicide: a systematic and quantitative review. Suicide Life Threat Behav. 2009;39(3):294-306. doi:10.1521/suli.2009.39.3.294
9. Alphs L, Brashear HR, Chappell P, et al. Considerations for the assessment of suicidal ideation and behavior in older adults with cognitive decline and dementia. Alzheimers Dement (NY). 2016;23;2(1):48-59. doi:10.1016/jtci.2016.02.001
10. Cosgrove C. Murder-suicides in elderly rise. WebMD. Accessed February 28, 2021. https://www.webmd.com/depression/features/murder-suicides-in-elderly-rise
11. Bourget D, Gagne P, Whitehurst L. Domestic homicide and homicide-suicide: the older offender. J Am Acadm Psychiatry Law. 2010;38(3):305-311.
12. Cohen D, Llorente M, Eisdorfer C. Homicide-suicide in older persons. Am J Psychiatry. 1998;155(3):390-396. doi:10.1176/ajp.155.3.390
13. Violence Policy Center. American roulette: Murder suicide in the United States. July 2020. Accessed February 28, 2021. https://vpc.org/studies/amroul2020.pdf
14. Malphurs JE, Eisdorfer C, Cohen D. A comparison of antecedents of homicide-suicide and suicide in older married men. Am J Geriatric Psychiatry. 2001;9(1):49-57. doi:10.1097/00019442-200102000-00008
15. Malphurs JE, Cohen D. A statewide case-control study of spousal homicide-suicide in older persons. Am J Geriatric Psychiatry. 2005;13(3):211-217. doi:10.1176/appi.ajgp.13.3.211
16. Salari S. Patterns of intimate partner homicide suicide in later life: strategies for prevention. Clin Interv Aging. 2007;2(3):441-452.
17. Zimmerman GM, Fridel EE. Contextualizing homicide-suicide: examining how ecological gun availability affects homicide-suicide at multiple levels of analysis. Homicide Studies. 2010;24(2):151-177. doi:10.1177/1088767919878478
18. Patient Health Questionnaire (PHQ-9). Stanford Medicine. Accessed February 28, 2021. https://med.stanford.edu/fastlab/research/imapp/msrs/_jcr_content/main/accordion/accordion_content3/download_256324296/file.res/PHQ9%20id%20date%2008.03.pdf
19. Mertens B, Sorenson SB. Current considerations about the elderly and firearms. Am J Public Health. 2012;202(3):396-400. doi:10.2105/AJPH.2011.300404
20. WISQARS™-Web-based Injury Statistics Query and Reporting System. US Centers for Disease Control and Prevention. Updated July 1, 2020. Accessed February 28, 2021. http://www.cdc.gov/injury/wisqars/index.html
21. Costs of care. LongTermCare.gov. Accessed February 28, 2021. longtermcare.acl.gov/costs-how-to-pay/costs-of-care.html
22. Zimmerman S, Cohen LW, Reed D, et al. Families matter in long-term care: results of a group-randomized trial. Seniors Hous Care J. 2013;21(1):3-20.l
23. Weapons Policies in Aging Services Organizations. Leading Age. 2018. Accessed February 28, 2021. https://www.leadingage.org/sites/default/files/Weapons%20Policies%20in%20Aging%20Services%20Organizations.pdf

