


Coil Embolization to the Right Side of the Heart After Elective Hypogastric Vein Embolization Requiring Open-Heart Surgery
Abstract
In the twenty-first century, minimally invasive procedures, including embolization procedures, have become widely available and used in a variety of disease treatments. Therapeutic embolization via a minimally invasive approach can be characterized as an occlusion of the vessel (artery or venous) to obtain a therapeutic benefit. Even with multiple technological advances, the procedure still has a small percentage of unwanted complications. Herein, we describe the case of a migrated coil to the heart after a hypogastric vein embolization that unfortunately attached to the tricuspid valve. The patient needed to undergo tricuspid valve replacement with coil retrieval via open thoracotomy after failed multiple attempts of percutaneous removal.
Case Report
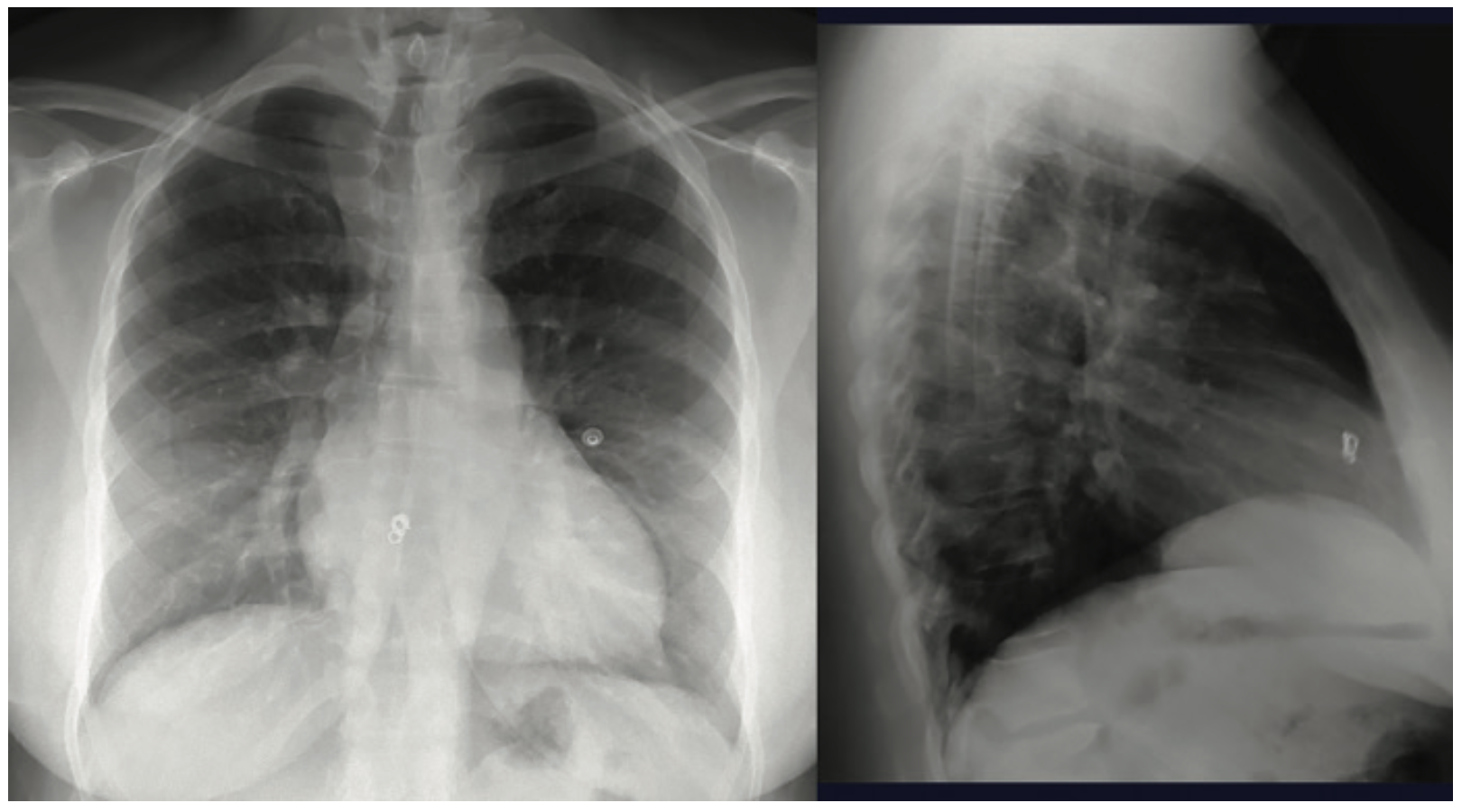
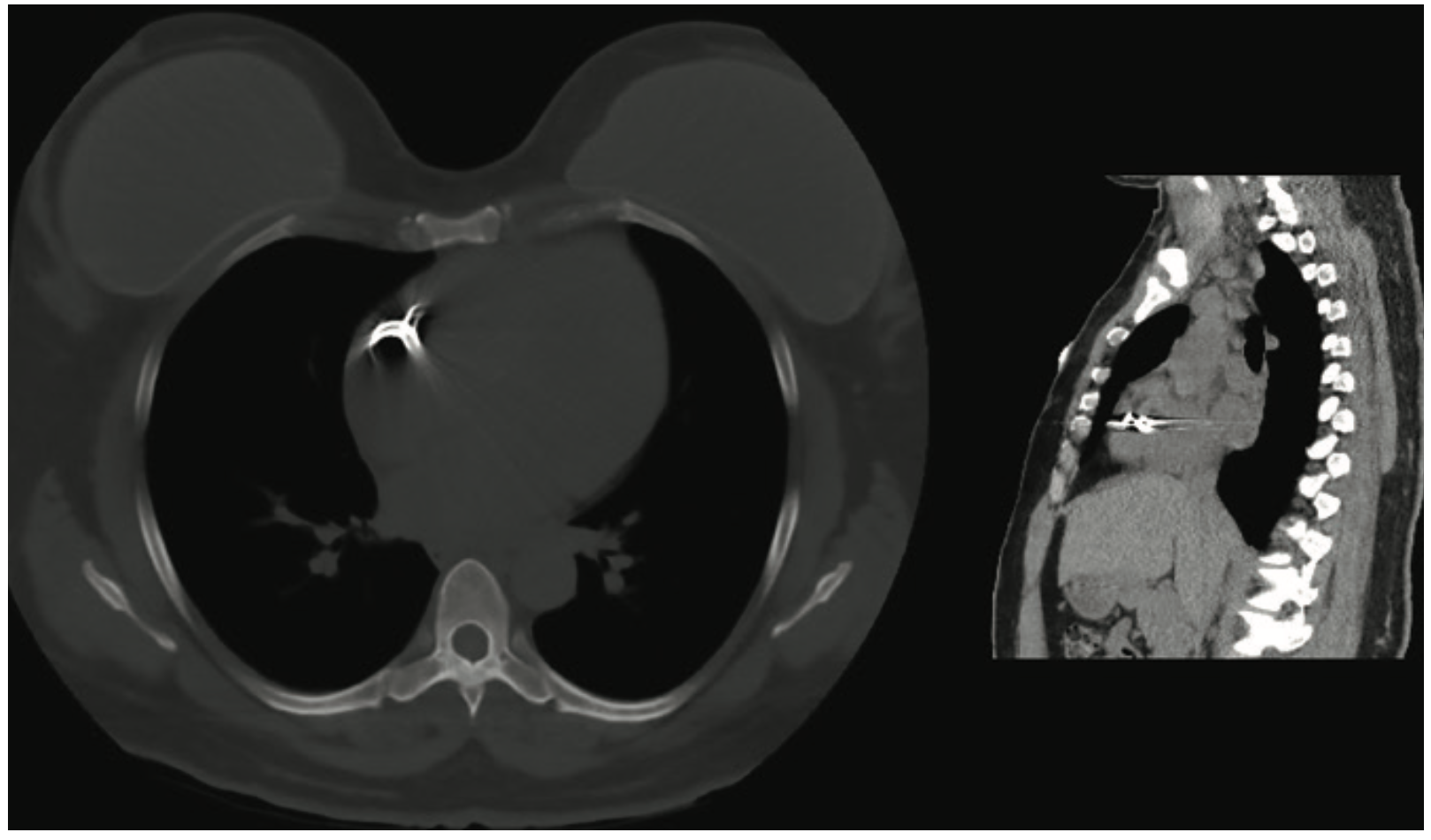
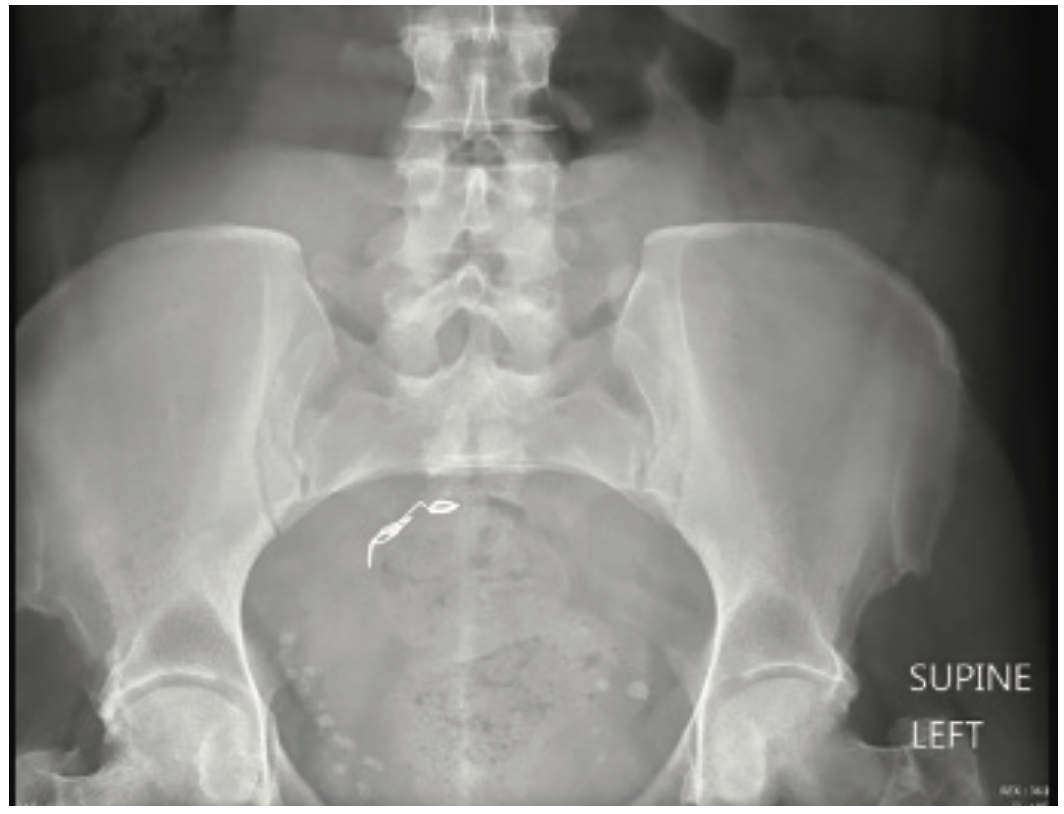
A 47-year-old woman with a medical history of hypertension and diabetes mellitus presented to the emergency department complaining of “something left in her heart.” Further history indicated that she had suffered from pelvic congestion syndrome and varicose veins in her legs, for which she underwent outpatient sclerotherapy and hypogastric vein embolization four days prior. Immediately after the procedure, coils dislodged from the performing instrument. Chest x-ray and a computed tomography chest scan revealed an approximately 11.7 mm coil located in the right atrium (Figures 1 and 2) and abdominal x-rays showed a coil implanted in the pelvis area (Figure 3). The patient was asymptomatic at that time. The day following her outpatient sclerotherapy and hypogastric vein embolization, coil retrieval via trans-jugular access was performed, but was unsuccessful even after a 5-hour attempt. The patient decided to come to our hospital emergency department (ED).
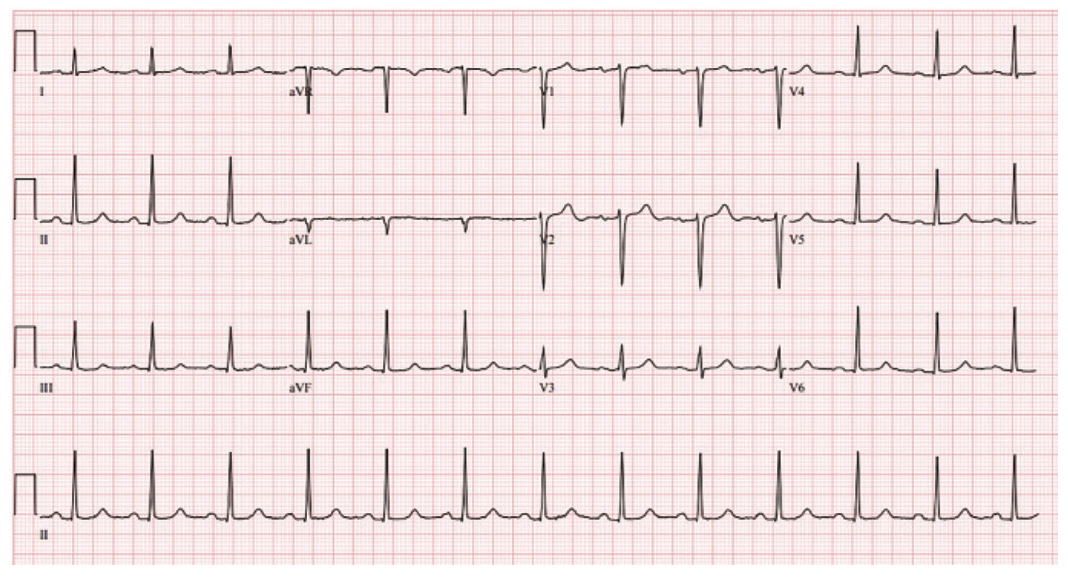
Upon arrival to the ED, she indicated some anxiety and denied chest pain, shortness of breath, palpitations, abdominal pain, or urinary symptoms. She was a lifetime nonsmoker, with no illicit drug usage. Remaining systems reviews were non-significant. Temperature was 98.2˚ F, heart rate 74 bpm, blood pressure 144/90mmHg, and oxygen saturation was 99% on room air. On examination, she was well-appearing but anxious, and resting comfortably in bed. Cardiovascular exam showed no jugular venous distension, and regular pulse rate without significant murmurs, rubs, or gallops. It was clear on lung auscultation, and the patient’s abdomen was soft, with normoactive bowel sounds without leg swelling. Electrocardiogram (EKG) showed normal sinus rhythm at 77 bpm without ST or T wave changes (Figure 4). Laboratory tests were significant with an elevated troponin I of 1.86 (normal <0.3 ng/ml), white blood cell of 7.4 x 109/L, hemoglobin of 13.1 g/dl, platelet count of 210,000 (normal 130-400 K/cmm), and serum creatinine of 0.8 (normal 0.7-1.3 mg/dl). Her coagulation panel was a PTT of 28.8, a PT of 10.7, and an INR of 1.0. A heparin infusion of 25,000 units/250 mL at a rate of 18 units/kg/hr was immediately started to prevent inadvertent blood clot formation secondary to the foreign body in the heart.
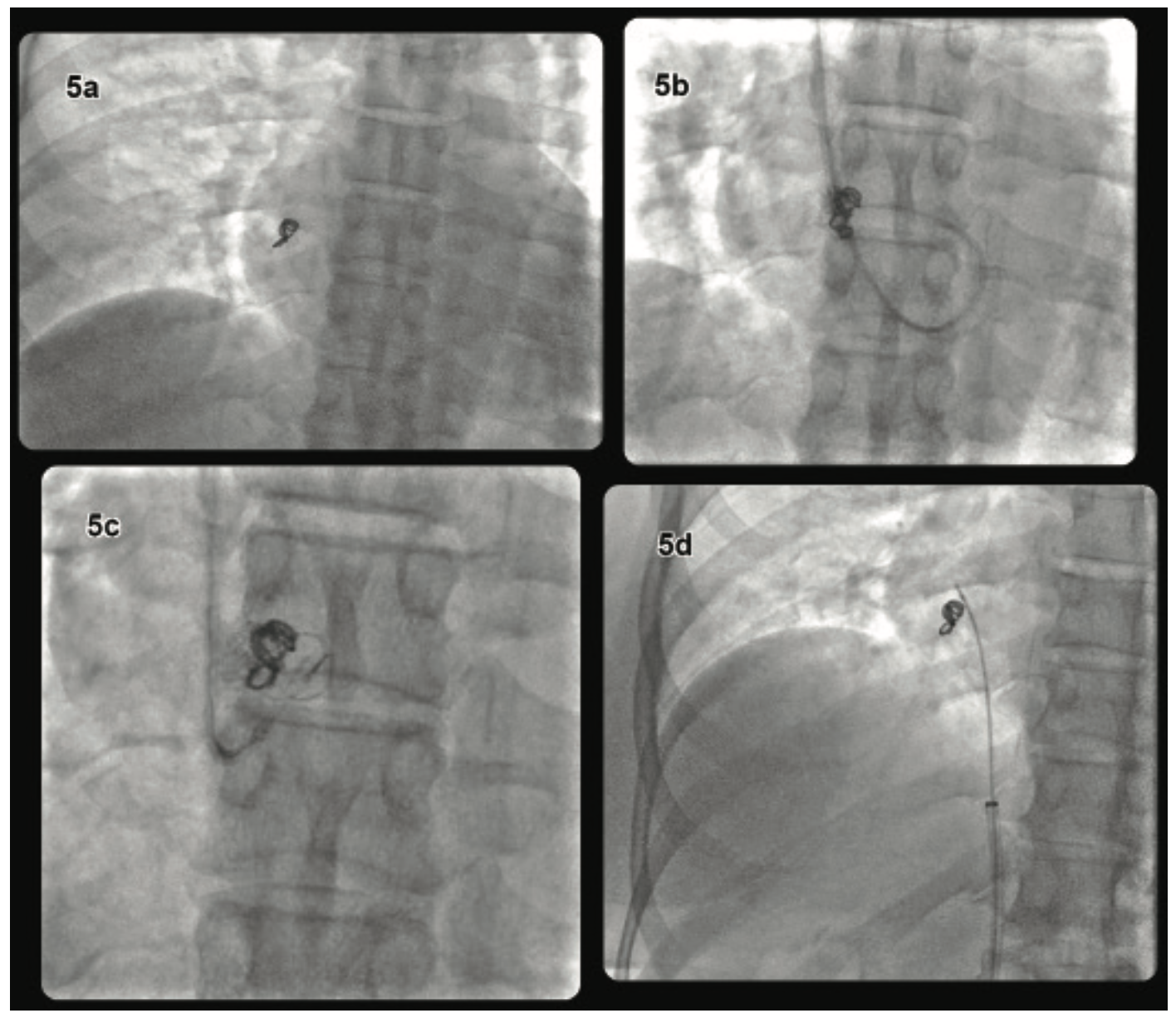
An attempt to retrieve the migrated coil was done via a percutaneous approach. Intravenous access was obtained through the right internal jugular vein and a 5 French (Fr) central venous sheath was inserted. A J-wire was advanced, followed by serial dilatation, and a 9 Fr venous sheath was placed. A Bentson starter wire (Cook Medical) was advanced and a 7 Fr Ansel 2 guide catheter (Cook Medical) was inserted. When the Ansel 2 catheter reached the right atrium, a 25 mm Amplatz Goose Neck snare (Medtronic) was introduced through the guide catheter to try to seize the coil, but this was unsuccessful, despite multiple attempts. Subsequently, a 7 Fr Atrieve 18-30 mm vascular snare set (Argon Medical Devices) was used in an attempt to capture the loop, also without success. Finally, we opted to try a different approach through the right common femoral vein in a similar fashion. Unfortunately, it was also unsuccessful, even after a one-hour attempt (Figure 5).
The cardiothoracic surgeon team was consulted and recommended open-heart surgery. The patient was transferred to a tertiary center where she underwent another percutaneous removal attempt without success. Open-heart surgery was performed to retrieve the foreign body from the right ventricle, but eventually, additional tricuspid valve repair was required, as the coil was firmly attached to a leaflet of the tricuspid valve. The patient recovered without further complications and went home four days after surgery.
Discussion
Pelvic vein embolization (PVE) is mainly performed in women with pelvic venous disorders that include pelvic vein congestion syndrome (PCS) and pelvic vein reflux disease associated with varicose veins in the legs. The use of coils in vascular embolization was introduced in approximately 1975, but in recent years, it has been used in the treatment of various pathologies, including PCS.2 Edwards et al reported the first case of ovarian vein embolization in 1993, while different approaches such as internal iliac (hypogastric) vein embolization and pelvic varices sclerotherapy have been proposed more recently.3,4 Although endovascular embolization is relatively safe procedure with modern instruments and technical maturity, the risk of coil migration still exists.
Coil migration to the heart, as in our patient, is unexpected but not uncommon. Ratnam et al questioned the role of PVE in lower limb varicosities management. In their study, 218 patients with PCS underwent PVE successfully, with a 1.4% risk of coil or stent displacement.5 Kwon et al studied the effectiveness of coil embolization via ovarian veins in those with PCS, achieving an 82% symptomatic improvement, but with a 3% risk of coil embolization.6 Turek et al presented a retrospective cohort study regarding intracranial aneurysm embolization in which the risk of coil or stent migration occurred in 0.75% of procedures.7
There are similar cases of coil entrapment and migration in previous literature. Leitman et al published a review article regarding 104 cases of foreign bodies in the heart, with a reported mortality rate of 3.8%.8 The majority of the foreign bodies were found in the right side of the heart and 88% traveled to the heart via migration. In those cases, 54% underwent surgical removal, while 29% were percutaneously removed, and 14% of cases were treated with conservative management.8 The presence of a foreign body in the heart brings increased risks of injury to endothelial structures, thrombosis, infection, and perforation. Immediate removal of the foreign body is usually required to prevent unwanted complications.
Lu et al reported the incident of a migrated coil to the left atrium after pulmonary arteriovenous malformation embolization where the coil retrieval via a percutaneous approach was successful.9 Various percutaneous removal methods have been used to extract migrated coils or foreign bodies. Oh et al reported a case of a migrated coil trapped in the chordae of the mitral valve after pulmonary arteriovenous malformation embolization.10 Percutaneous endovascular removal was performed through the right femoral vein and went into the left atrium via transseptal puncture, where the coil was successfully retrieved with a 25 mm Amplatz Goose Neck snare.10 An entrapped guidewire in the right side of the heart was described by Padiyath et al.11 Percutaneous removal was attempted by a right femoral venous approach. A 5 mm Amplatz Goose Neck snare catheter set was initially used to try and grasp the coil without success. A 6 Fr Atrieve 9-15 mm vascular snare was inserted and the wire fragment was then retrieved.11 Although percutaneous removal is feasible in contemporary practice, the rate of success is not high, even with technical and instrumental advances. Singh et al calculated that the success rate of percutaneous coil retrieval is approximately 50%.12
After thorough review and analysis of the previously published literature, the ability to extrapolate an ideal method or technique to remove a foreign body that has migrated to the heart remains uncertain. However, the procedure success rate can be increased by knowing the exact anatomy related to the migrated coil, careful case planning, and the availability of different equipment. Among different vascular snares, the Amplatz Goose Neck is generally the first choice, followed by the Atrieve vascular snare and intravascular retrieval forceps. Retrieval of the foreign body should first be attempted with a percutaneous approach, followed by surgical intervention if the percutaneous approach fails.
In our case, accidental coil dislodgment with migration to heart occurred directly after the hypogastric vein embolization procedure, resulting in damage to the tricuspid valve requiring open-heart surgery. Since 1993, PVE has been used to treat pelvic vein congestion. However, the effectiveness of PVE is unclear with the scarcity of large, randomized clinical research trials. At the same time, procedure-related risks are still present and could lead to a devastating event. Careful patient selection and pre-procedural planning with a proper understanding of risk and benefit remain crucial to prevent any untoward complications.
Conclusion
Minimally invasive procedures should be approached with the same level of caution as those that are more invasive. The risks of complication and patient safety should be thoroughly discussed prior to the procedure. In this case, we have discovered a seldom-discussed procedure-related complication and hope to increase awareness of the dangers of what has been marketed as a minimally invasive cosmetic procedure.
References
- Di Segni R, Young AT, Qian Z, Castaneda-Zuniga WR. Embolotherapy: agents, equipments and techniques. In: Castaneda-Zuniga WR, ed. Interventional Radiology. Baltimore: Williams and Wilkins; 1992:29-103.
- Gianturco C, Anderson JH, Wallace S. Mechanical devices for arterial occlusion. Am J Roentgenol Radium Ther Nucl Med. 1975 Jul; 124(3): 428-435.
- Edwards RD, Robertson IR, MacLean AB, Hemmingway AP. Case report: pelvic pain syndrome—successful treatment of a case by ovarian vein embolization. Clin Radiol. 1993; 47: 429-431.
- Lopez AJ. Female pelvic vein embolization: indications, techniques, and outcomes. Cardiovasc Intervent Radiol. 2015 Aug; 38(4): 806-820. doi: 10.1007/s00270-015-1074-7.
- Ratnam LA, Marsh P, Holdstock JM, et al. Pelvic vein embolisation in the management of varicose veins. Cardiovasc Intervent Radiol. 2008 Nov-Dec; 31(6): 1159-1164. doi: 10.1007/s00270-008-9402-9.
- Kwon SH, Oh JH, Ko KR, et al. Transcatheter ovarian vein embolization using coils for the treatment of pelvic congestion syndrome. Cardiovasc Intervent Radiol. 2007 Jul-Aug; 30(4): 655-661.
- Turek G, Kochanowicz J, Lewszuk A, et al. Early surgical removal of migrated coil/stent after failed embolization of intracranial aneurysm. J Neurosurg. 2015 Oct; 123(4): 841-847. doi: 10.3171/2015.1.JNS132788.
- Leitman M, Vered Z. Foreign bodies in the heart. Echocardiography. 2015 Feb; 32(2): 365-371. doi: 10.1111/echo.12795.
- Lu TL, Qanadli SD. Percutaneous retrieval of a migrated coil in the left atrium. Radiol Case Rep. 2015 Nov 6; 5(4): 335. doi: 10.2484/rcr.v5i4.335.
- Oh PC, Kang WC, Choi DY, et al. Successful percutaneous endovascular retrieval of a coil in the left ventricle which migrated during embolization for pulmonary arteriovenous malformation. Int J Cardiol. 2013 Feb 20; 163(2): e33-e35. doi: 10.1016/j.ijcard.2012.08.045.
- Padiyath A, Fontenot EE, Abraham BP. Removal of a retained intracardiac radiolucent guidewire fragment using an Atrieve™ vascular snare using combined fluoroscopy and transesophageal echocardiography guidance in an infant. Ann Pediatr Cardiol. 2017 Jan-Apr; 10(1): 65-68. doi: 10.4103/0974-2069.197068.
- Gulati S, Singh AK. Coil migration to pulmonary vasculature: case report and review. SM Radiol J. 2015; 1(1): 1001.
1Division of Cardiology, The Brooklyn Hospital/Mount Sinai Beth Israel Hospital, Academic Affiliate of The Icahn School of Medicine at Mount Sinai, Clinical Affiliate of The Mount Sinai Hospital, Brooklyn, New York; 2Division of Cardiology, Mount Sinai Hospital, New York, New York; 3Division of Cardiothoracic Surgery, Mount Sinai Hospital, New York, New York; 4Department of Internal Medicine, The Brooklyn Hospital Center, Academic Affiliate of The Icahn School of Medicine at Mount Sinai, Clinical Affiliate of The Mount Sinai Hospital, Brooklyn, New York
Disclosures: The authors have no conflicts of interest or financial relationships to disclose.
The authors can be contacted via Htoo Kyaw, MD, at htookyaw2007@gmail.com.

