


A Physician’s Perspective on New Permanent Reimbursement Pathways for Coronary Intravascular Lithotripsy
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
 How did the previous, temporary reimbursement pathways impact intravascular lithotripsy (IVL) utilization within your practice?
How did the previous, temporary reimbursement pathways impact intravascular lithotripsy (IVL) utilization within your practice?
The previous IVL codes were temporary pathways as part of a breakthrough technology designation from Centers for Medicare and Medicaid (CMS). The two pathways were New Technology Add-on Payment (NTAP) or Transitional Pass-Through (TPT). These codes were helpful in that they allowed IVL technology to reach the market and allowed the cost of the device to be accounted for. You weren’t losing money by using IVL, so the previous codes were very beneficial from that perspective.
I work in a larger academic model and many of our cases are referrals that have been unable to be treated elsewhere. There is an acceptance within the institution that certain cases are going to be exceptionally expensive because of the time, resources, and equipment required. It depends on your practice pattern as to how attuned you are to these issues, but we are all aware of an escalating cost when multiple different devices need to be used, such as a case using both atherectomy and IVL. Or perhaps there is an in-stent lesion or a chronic total occlusion, and you perform IVL but don’t put in a stent, which is another scenario where the previous reimbursement models would not necessarily have made it a profitable case for the institution.
There are a few important, overarching principles. Number one is you always use the right tool for the right patient to get the most optimal result. Number two, we do have a responsibility to behave responsibly in the way that we use resources. Having an overall awareness of reimbursement costs and health economics is important for physicians. The new IVL reimbursement pathways are cleaner, more straightforward, and easier for both physicians and administrators to understand.
Can you describe the current status of IVL reimbursement?
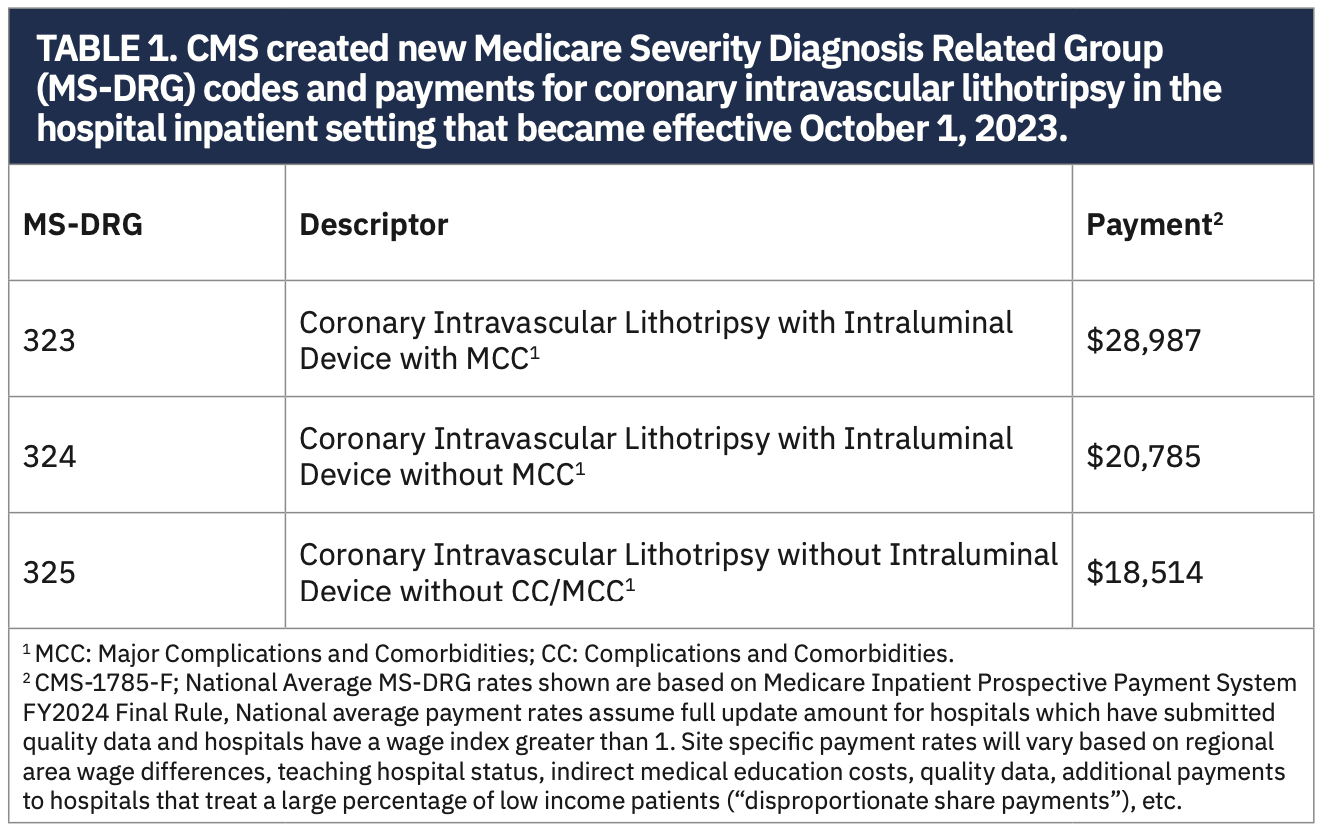
The two main changes that people need to be aware of are first, for inpatient cases, there are new, dedicated diagnosis-related groups (DRGs) for IVL (Table 1). The new DRG codes are not based on any other technologies, codes, or pathways. What this means for inpatient procedures is that if you use IVL, the new DRG gives you an uplift in reimbursement. The exact amount of uplift depends on specific geographic and other factors, but on average, it appears that it will be around $8000 per case, which obviously more than offsets the cost of the IVL balloon. That number was reached by Medicare from reviewing the cases where IVL technology was used, which overall tend to be more complex cases. The other thing that is worth mentioning for this inpatient reimbursement is that the code for IVL exists independent of whether a stent is placed. There are two buckets: Percutaneous Coronary Intervention (PCI) With Stent Placement and PCI Without Stent Placement. For each of those categories, there now exists a separate DRG for IVL. The new DRGs came into effect from October 1st, 2023, so these have already been established.
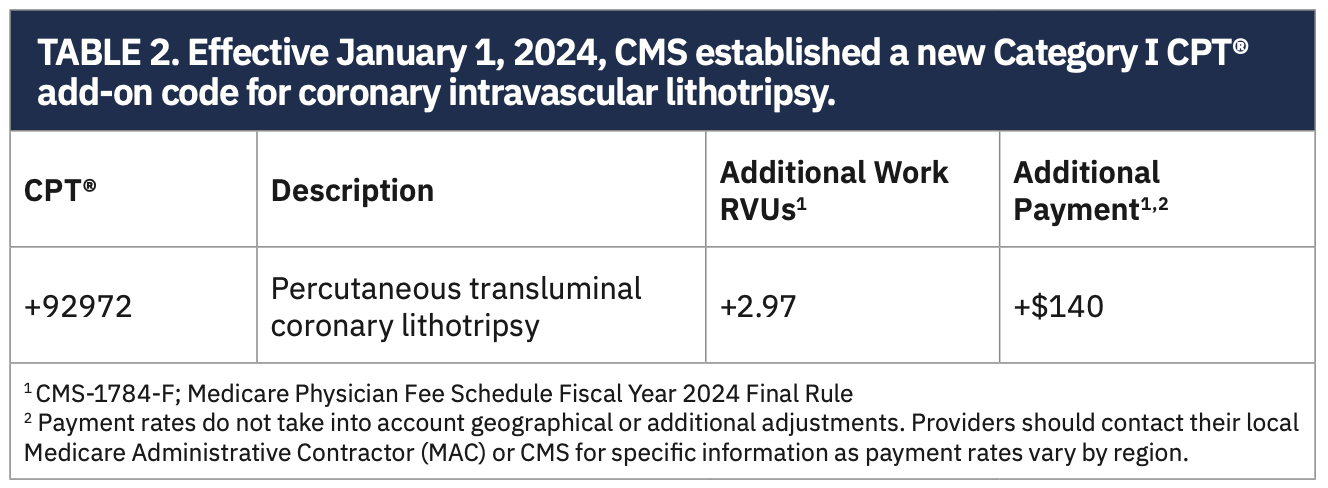
The other new pathway is physician reimbursement, which came into effect from January 1, 2024. IVL has a new Current Procedural Terminology (CPT) code that is unique to IVL (Table 2). It is an add-on code and not bundled with any other procedures. No matter what else you have done in the case, if you use IVL, there is now an add-on code that you bill in addition to everything else. The CPT code provides just under three additional work Relative Value Units (RVUs) per case.
Importantly, the new coding pathways are agnostic to the use of any other adjunctive devices. Earlier I mentioned those cases when you need to use multiple devices like atherectomy and IVL, where you are really aware of the cost racking up. Atherectomy and IVL are expensive devices, but at least at the physician level, the new pathway will allow you to get reimbursed for the use of both devices. If there is a case where you do atherectomy, stent placement, etc., there are codes for those. As of January 1, 2024, if you also use IVL, then you add on the CPT code for IVL use. It also counts whether there is stent placement or no stent placement, treatment of a chronic total occlusion, use of imaging, use of atherectomy, and so on. Whatever you do, the CPT code brings an uplift for using IVL as well.
Is there anything specific to non-clinical stakeholders in terms of what they should know about coronary IVL reimbursement?
Cath lab managers, administrators, and people looking at the overheads should be aware of this change because it is going to alter the landscape. If you are doing a complex case using multiple devices, there is no longer the potential for a financial penalty from using certain technologies like IVL, either at the institutional level or at the physician level, which means that we are now liberated. You never want to make treatment decisions based on economic implications, but the reality is that you have to be at least aware of the financial and economic implications. Removing these potential barriers to use of IVL is a good thing. The last thing you want is either whoever’s running the cath lab or the physician to pause and think, do I want to pull this off the shelf because of the cost? That thinking can go by the wayside because the reimbursement means it should no longer be a factor. As long as physicians document that they used IVL, then reimbursement should be very straightforward.
What do you think about the pairing of the new reimbursement pathways for coronary IVL with the launch of Shockwave C2+?
Occasionally we saw, certainly with the C2, that you might finish your 80 pulses in one lesion and it hadn’t fully modified the calcium. This should certainly be less of an issue with C2+ and the 50% extra pulses. Having 120 pulses rather than 80 does unlock the ability to treat longer lesions. It is also very helpful for treating multiple vessels with one catheter. Let’s say you have lesions in the circumflex and left anterior descending coronary arteries. You could ration your pulses between the two, and as long as the catheter can be delivered, the extra pulses allow you to effectively modify multiple lesions and multiple vessels with a single catheter.
The new reimbursement hasn’t changed my strategy or practice pattern, but particularly for the combination therapy cases, it is reassuring that you can get reimbursed for atherectomy and lithotripsy, which is a strategy I employ frequently. In complex cases, you often need to use multiple devices to get an optimal result. The new codes will allow for that without potential of it being financially punitive.
Have the 40 additional pulses available with the Shockwave C2+ IVL catheter changed how you approach cases?
For a longer lesion that needed calcium modification, I might have previously defaulted to atherectomy because of the challenges in modifying a long lesion with only 80 pulses (and while it is rare, it was certainly not unheard of to use multiple IVL catheters in a case for a long lesion). There is a huge portion of cases that I still treat with atherectomy for other reasons, but if lesion length was the only reason why I was using an atherectomy device, then I now have the option to use only IVL and just use the C2+.
Any final thoughts?
Reimbursement for hospital outpatient procedures will be looked at next by CMS. Inpatient and physician reimbursement have been addressed. The C2+ is now available throughout the country. The only other thing to mention about the C2+ is that everything else about this device is the same: crossability, deliverability, and ease of use are identical to the C2. The cost is the same. The C2+ just adds 40 extra pulses.
This interview is sponsored by Shockwave Medical. Dr. Ahmad is a paid consultant for Shockwave Medical.
Find More:
Peripheral Artery Disease Topic Center
Cardiovascular Ambulatory Surgery Centers (ASCs) Topic Center
Grand Rounds With Morton Kern, MD
The Latest Clinical & Industry News
Podcasts: Cath Lab Conversations



