


Increasing the Efficiency of Mechanical Thrombectomy Procedures for Deep Vein Thrombosis
Deep vein thrombosis (DVT) obstructs lower extremity venous outflow, often leading to acute and long-term reduction in quality of life.1,2 In fact, up to 40-50% of DVT patients experience chronic symptoms related to post-thrombotic syndrome (PTS).3-6 Fortunately, endovascular techniques to treat DVT are now available.7,8 One device designed specifically to treat DVT is the ClotTriever System (Inari Medical), which has shown promising results.9-14
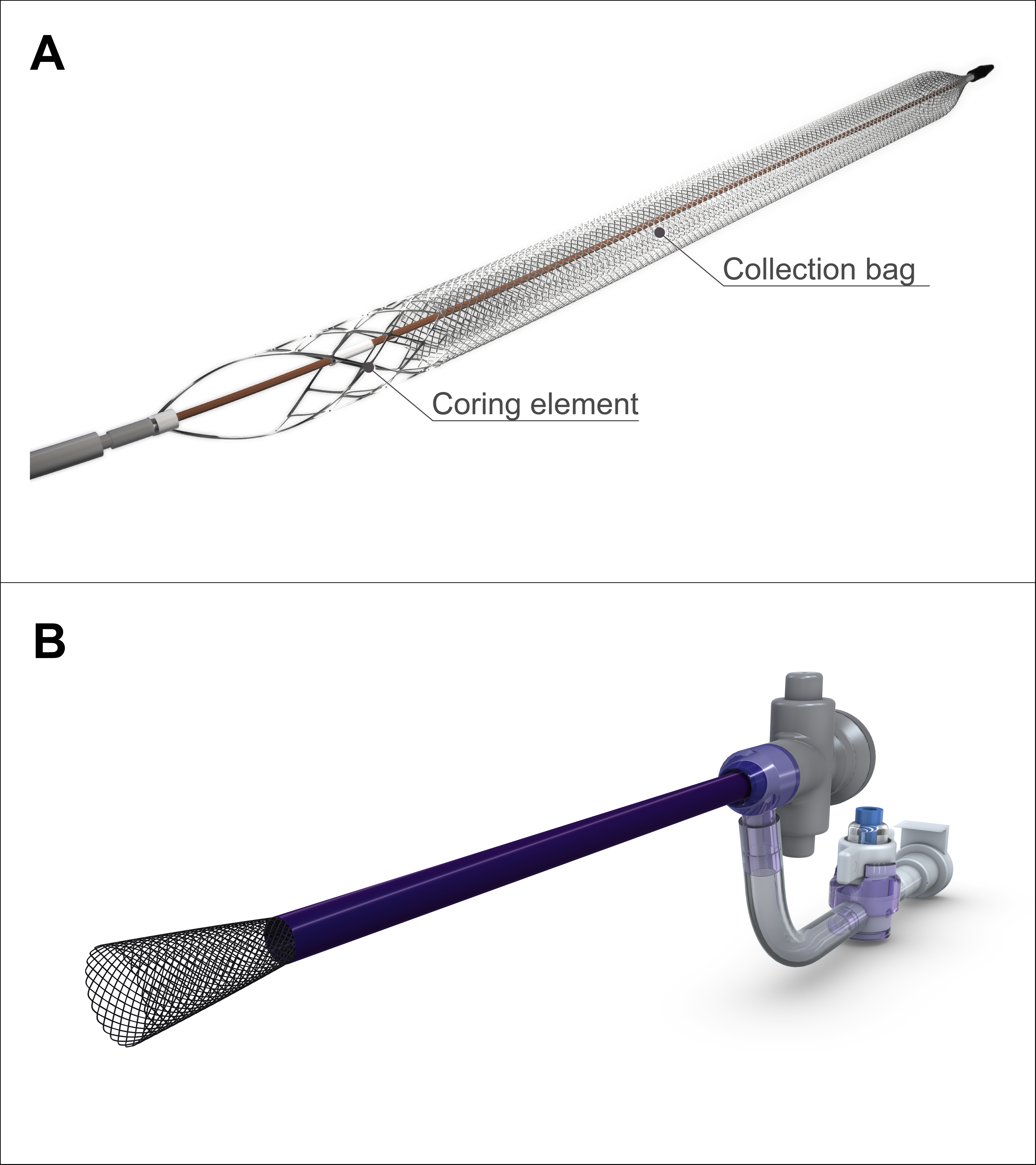
The ClotTriever System is comprised of two main components: a catheter with a nitinol coring element and mesh collection bag (Figure 1A) and a sheath to enable removal of the thrombus (Figure 1B). Once venous access is gained, the ClotTriever catheter is advanced over a guidewire and positioned above the location of the thrombus. The nitinol coring element and mesh collection bag are then expanded and subsequently pulled through the vessel, capturing thrombus in the collection bag as it is retracted toward the access site. The catheter is then removed from the body, at which point thrombus is cleaned off the collection bag and the catheter can then be reinserted for additional passes.
A recently presented analysis of 250 real-world DVT patients in the ongoing CLOUT Registry demonstrated consistent thrombus removal in the majority of patients treated with the ClotTriever System, including 85.8% who achieved complete or near complete (≥75%) thrombus removal.15 The median thrombectomy time was 28 minutes and a median of 4 device passes were used. Almost all (99.6%) procedures were completed in a single session, with no thrombolytics used and a median blood loss of 50 mL. At 6 months post procedure, 91.3% of patients were free from moderate or severe post-thrombotic syndrome (PTS).
Although the data surrounding the use of ClotTriever System are promising, one of the most challenging aspects of the procedure is removing adherent thrombus from the ClotTriever collection bag between passes. This can be time consuming and, anecdotally, can require up to several minutes per thrombectomy pass. Traditional techniques for removing thrombus include gently flicking or tapping the bag and coring element while holding the device upright, which not only takes time, but can be quite frustrating and can even kill the momentum of the procedure.
We present herein a new technique, coined locally as the “Turboflick”, which allows for rapid thrombus removal and a quick return to the thrombectomy procedure after each ClotTriever pass.
Turboflick Technique
The following steps are needed to perform the Turboflick optimally:
Step 1. Carefully remove the ClotTriever catheter from the body. Open the coring element and desiccate the extracted thrombus using the typical technique. For most operators, this means rolling the collection bag and coring element inside a dry sterile towel. Note: For more acute (i.e., stickier) thrombus, more emphasis should be placed on desiccation.
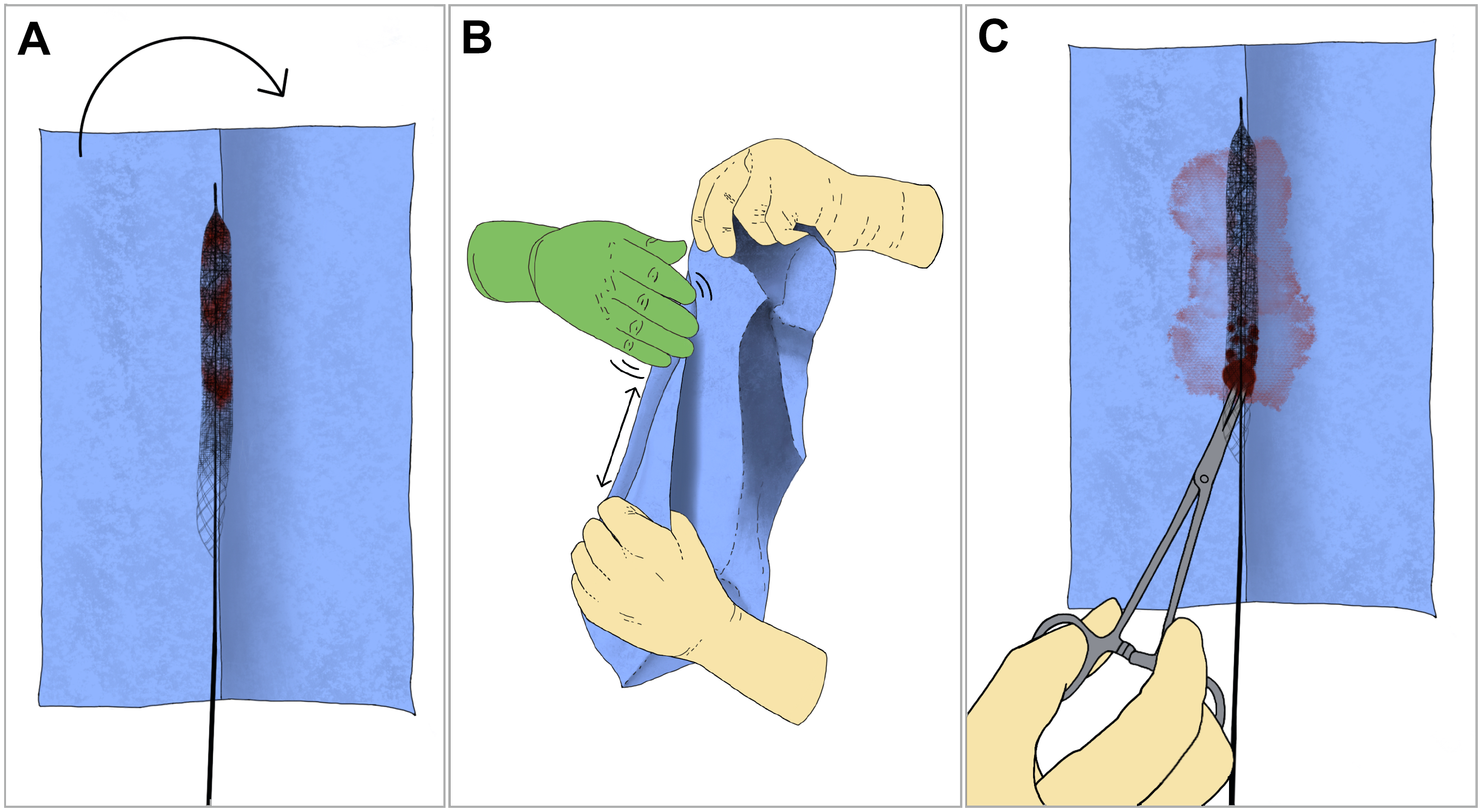
Step 2. Cover the catheter with a sterile towel, which will prevent scattering of thrombus during the maneuver (Figure 2A).
Step 3. Have an assistant or second operator hold the towel-wrapped ClotTriever catheter vertically by pinching the tip with one hand and the base (below the coring element) with the other. Pull the catheter taut, with enough tension to maximize rigidity of the collection bag, like a tightly drawn guitar string.
Step 4. The primary operator should flick or slap the bag and coring element rapidly in a back-and-forth motion at a frequency of at least 5-6 flicks per second. Start at the tip of the catheter and move slowly downwards to the coring element (Figure 2B). Repeat this “Turboflick” maneuver 2-3 times. Note: More adherent thrombus may require additional cycles.
Step 5. Remove the sterile towel. In many instances, thrombus will fall out of the coring element onto the table. If it does not, use curved Kelly clamps or a similar tool to extract the thrombus collected within the coring element (Figure 2C).
Step 6. Rinse the ClotTriever collection bag and coring element in sterile saline. Retract the ClotTriever catheter and re-insert into the patient for the next pass of thrombectomy.
View a video explaining the Turboflick Technique here.
Case Vignette
A 62-year-old female with a history of hypertension, recent plastic surgery with abdominoplasty and liposuction, and recent long-haul travel, presented with left leg pain, swelling, inability to stand or ambulate, and altered sensation in the left ankle and foot.
Imaging in the emergency department revealed segmental pulmonary embolism in the right lower lobe as well as deep venous thrombosis throughout the left lower extremity. Left lower extremity thrombotic burden spanned from calf veins to the femoral vein, common femoral vein, external iliac vein, common iliac vein, and inferior vena cava (IVC). A computed tomography (CT) scan of the abdomen/pelvis was also performed, demonstrating compression of the left common iliac vein by the crossing right common iliac artery, in keeping with May-Thurner Syndrome.
After clinical evaluation, the decision was made to perform mechanical thrombectomy with the ClotTriever System while providing embolic protection (because of the IVC thrombus) with the FlowTriever catheter (Inari Medical).
Procedure
The patient was positioned prone on the angiography table. Ultrasound guidance was used to access both the right and left popliteal veins. A 4 French (Fr) microcatheter was advanced, followed by insertion of a 5 Fr vascular sheath into each vein.
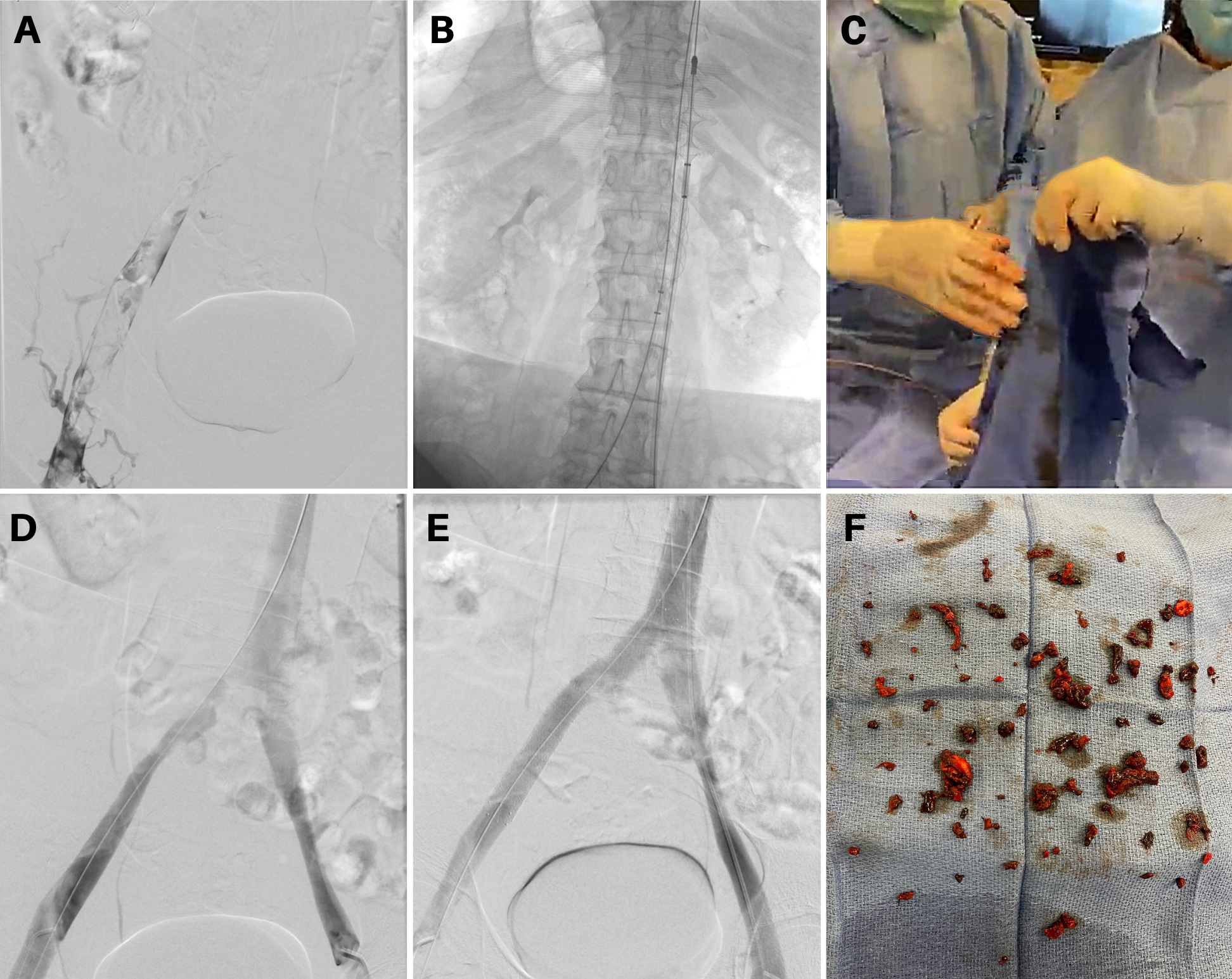
A venogram from the left popliteal vein access confirmed extensive thrombosis of the left lower extremity (Figure 3A). A catheter and wire were used to cross thrombosed segments into the IVC and, subsequently, the SVC. An Amplatz wire (Boston Scientific) was placed into the right internal jugular vein for stable access. This process was repeated for the right popliteal vein access.
The FlowTriever System was advanced over the guidewire from the right popliteal vein access into the IVC beyond the thrombus and the FlowTriever disks were deployed for embolic protection. The ClotTriever sheath was then placed into the left popliteal access and then the ClotTriever catheter was advanced beyond the thrombus (Figure 3B). The coring element and collection bag were deployed, and the catheter was retracted toward the access site to capture and extract the thrombus.
Once the ClotTriever collection bag was removed from the body, the Turboflick technique was employed to quickly clear the extracted thrombus (Figure 3C). The catheter was reintroduced through the left popliteal access, and the process of thrombus extraction and clearing the collection bag was repeated for a total of 8 passes over a period of approximately 30 minutes. Nearly all of the visualized thrombus was removed; however, there is a severe narrowing of the central aspect of the left common iliac vein in keeping with May-Thurner Syndrome (Figure 3D).
Venoplasty was performed up to 16 mm and a 16 mm x 120 mm VICI stent (Boston Scientific) was placed to treat the May-Thurner compression in the left common iliac vein. Additionally, after a venogram confirmed that no thrombus was trapped in the FlowTriever discs, the discs were captured and removed.
Completion venogram showed rapid antegrade flow with patent left pelvic and lower extremity veins; no significant thrombus remained (Figure 3E). All wires and catheters were carefully removed and manual compression and a stitch were used to achieve hemostasis. A large amount of thrombus was extracted during the procedure (Figure 3F).
Following the procedure, the patient rapidly experienced significantly reduced pain and swelling. The following morning, she was ambulating with no pain. She was discharged on hospital day 2 on enoxaparin and low-dose aspirin. At 3-month clinic follow-up, she had no residual swelling in her left lower extremity and had resumed her normal activities of daily living.
Discussion
A patient presented with extensive thrombus burden involving the IVC and the entire left lower extremity. This challenging case was tackled using mechanical thrombectomy with the ClotTriever System and embolic protection with the FlowTriever System, followed by venoplasty and stenting. The procedure resulted in essentially complete recanalization of the left lower extremity veins, leading to quick resolution of patient symptoms.
Notably, the overall efficiency of the procedure was improved by the Turboflick technique. The technique was utilized for each of 8 passes with the ClotTriever System, allowing for rapid removal of adherent thrombus from the collection bag between passes with the ClotTriever device. Despite an especially large thrombus burden, a large number of passes were able to be managed in a timely fashion due to the Turboflick technique. Regular application of the Turboflick technique has been instrumental in our facility’s ability to perform venous thrombectomy procedures with increasing speed.
Conclusion
Endovascular techniques are increasingly common for DVT, and need to be made simple and efficient. The ClotTriever System is an excellent tool for extracting thrombus; however, removing thrombus from the collection bag is the most challenging aspect of its use. The Turboflick is a promising new technique to increase efficiency and decrease frustration while performing an extremely important intervention.
Acknowledgements: Melissa Alvarez, Robyn Brook, Caroline Kragh, Gaejeong Lee, Craig Markovitz, Taylor Scheinblum, Brian Strauss, Shanthi Vandrangi
References
1. Jaff MR, McMurtry MS, Archer SL, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. Apr 26 2011; 123(16): 1788-1830. doi:10.1161/CIR.0b013e318214914f
2. Dronkers CEA, Mol GC, Maraziti G, et al. Predicting post-thrombotic syndrome with ultrasonographic follow-up after deep vein thrombosis: a systematic review and meta-analysis. Thromb Haemost. Aug 2018; 118(8): 1428-1438. doi:10.1055/s-0038-1666859
3. Ashrani AA, Heit JA. Incidence and cost burden of post-thrombotic syndrome. J Thromb Thrombolysis. Nov 2009; 28(4): 465-476. doi:10.1007/s11239-009-0309-3
4. Prandoni P, Lensing AW, Cogo A, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med. Jul 1 1996; 125(1): 1-7. doi:10.7326/0003-4819-125-1-199607010-00001
5. Kahn SR, Shapiro S, Wells PS, et al. Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial. Lancet. Mar 8 2014; 383(9920): 880-888. doi:10.1016/S0140-6736(13)61902-9
6. Carter CJ. The natural history and epidemiology of venous thrombosis. Prog Cardiovasc Dis. May-Jun 1994; 36(6): 423-438. doi:10.1016/s0033-0620(94)80051-0
7. Enden T, Haig Y, Klow NE, et al. Long-term outcome after additional catheter-directed thrombolysis versus standard treatment for acute iliofemoral deep vein thrombosis (the CaVenT study): a randomised controlled trial. Lancet. Jan 7 2012; 379(9810): 31-38. doi:10.1016/S0140-6736(11)61753-4
8. Vedantham S, Goldhaber SZ, Julian JA, et al. Pharmacomechanical catheter-directed thrombolysis for deep-vein thrombosis. N Engl J Med. Dec 7 2017; 377(23): 2240-2252. doi:10.1056/NEJMoa1615066
9. Abramowitz S. Effective removal of chronic thrombus with the ClotTriever System: results from the CLOUT Registry. Journal of Vascular Surgery: Venous and Lymphatic Disorders. 2021; 9(2): 544-545. doi:10.1016/j.jvsv.2020.12.028
10. Bertino FJ, Shin DS, Monroe EJ, et al. Thrombectomy of malignant thoracic central venous occlusive disease using Inari ClotTriever System. J Vasc Interv Radiol. 2021 Sep; 32(9): 1398-1400. doi: 10.1016/j.jvir.2021.05.018
11. Daub AC, Shin DS, Meissner MH, et al. Transient arterial insufficiency and neurologic deficit following external iliac vein stent reconstruction for malignant compression. J Vasc Surg Cases Innov Tech. 2021 May 21; 7(3): 469-473. doi: 10.1016/j.jvscit.2021.05.007
12. Fortich S, Ritchie C, Shaikh ME, et al. Deep vein thrombosis in the setting of Klippel-Trenaunay syndrome and sirolimus treatment. J Vasc Surg Cases Innov Tech. 2021 Jul 17; 7(3): 524-528. doi: 10.1016/j.jvscit.2021.06.014
13. Kumar G, Effoe VS, Kumar A, Verma I, Sachdeva R. Intravascular ultrasound-guided catheter-based aspiration thrombectomy in patients with acute submassive pulmonary embolism: A case series. Cardiovasc Revasc Med. 2021 May 19: S1553-8389(21)00260-8. doi: 10.1016/j.carrev.2021.05.016
14. Beasley R. ClotTriever mechanical thrombectomy for chronic deep vein thrombosis: subgroup analysis from the CLOUT Registry. Journal of Vascular and Interventional Radiology. 2021; 32(5): S25. doi:10.1016/j.jvir.2021.03.474
15. Beasley, R. An Update On the CLOUT Registry presented at: New Cardiovascular Horizons; June 4, 2021; New Orleans, LA.
Disclosure: Dr. Misono reports he is a consultant to Inari Medical, NXT Biomedical, and TriSalus Life Sciences.
He can be contacted at amisono@newportradiology.com
