


Serranator PTA Serration Balloon Utilized in CLTI Patient: Wound Healed
Patient Presentation
A 61-year-old patient with type 2 diabetes and end-stage renal disease on hemodialysis was referred from podiatry with a worsening left foot wound for the last year. He previously had right foot wounds that had healed after successful treatment with tibial atherectomy and angioplasty. At this time, the left foot had an approximately 3 cm x 3 cm wound affecting the left lateral hindfoot, see image (Figure 1).
Initial non-invasive testing showed a right ankle-brachial index (ABI) of 0.39 and a left ABI of 0.65. A left leg arterial duplex demonstrated calcific, diseased, largely occluded anterior tibial and peroneal arteries. The posterior tibial artery was suggested as largely patent.

Intervention
The presence of the left foot non-healing wound and the positive non-invasive testing results led to a diagnostic angiogram. The procedure began with a right femoral contralateral access. Inflow was visualized as largely patent and intact including the aortoiliac segment as well as the femoral-popliteal segment.
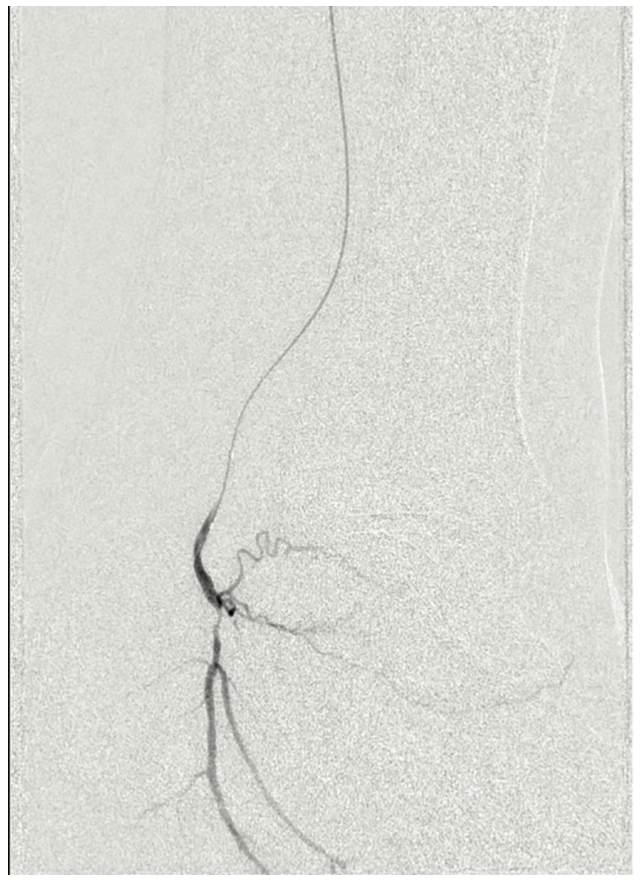
The patient had known infrapopliteal disease which was imaged as part of the initial diagnostic portion of the procedure. The angiogram revealed a chronically occluded long segment of the left anterior tibial artery. The peroneal artery had a focal occlusion in the proximal portion of the left calf and appeared to be relatively preserved in its mid and distal segments. The posterior tibial artery had a high-grade, approximately 99% narrowing at the left ankle mortise at the transition from the ankle into the foot (Figure 2).
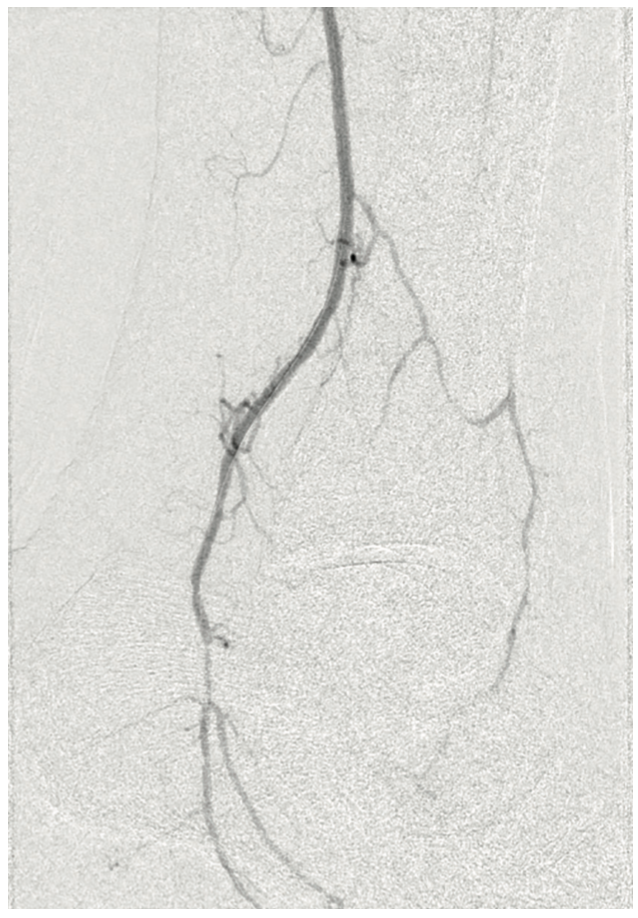
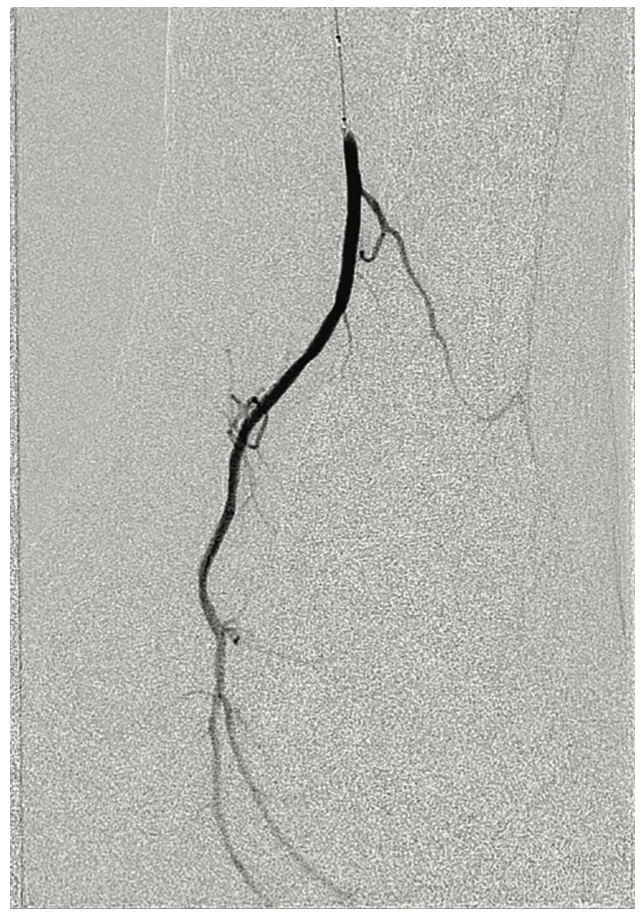
The patient was heparinized. A long 6 French Destination sheath (Terumo Interventional Systems) was used to cannulate the femoral-popliteal artery with an .035-inch system. We then selectively cannulated the posterior tibial artery with an .014-inch Grand Slam wire (Asahi Intecc). Using an .014-inch catheter and wire, we were able to pass through the distal posterior tibial artery stenosis into the pedal vessels. We started with a 2.0 mm plain balloon (POBA), resulting in recoil (Figures 3-4). We then used a 2.5 mm diameter Serranator PTA Serration Angioplasty Balloon (Cagent Vascular) (Figure 5) and achieved significant lumen gain without recoil. The peroneal artery lesion was also treated with angioplasty. The posterior tibial artery was considered to be the most important for wound healing, as the peroneal artery mostly terminated at the ankle level and the posterior tibial artery had strong dominant flow into the left foot. In addition, the anterior tibial and dorsalis pedis pathway was chronically occluded and essentially clinically nonexistent.


PTA Serration Balloon Catheter (Cagent Vascular).
The final imaging of the posterior tibial artery demonstrated a surprisingly positive angiographic result with brisk blood flow and was clinically satisfactory (Figure 6). We were encouraged with this outcome, and optimistic for eventual wound healing.
Conclusions
This patient had limb-threatening ischemia of the left lower extremity requiring intervention, with successful healing of his wound. The procedure was technically straightforward, involving catheter and wire manipulation for crossing tibial occlusive disease, using pre-dilation with angioplasty, and then serration angioplasty. This is in contrast to more complex techniques involving atherectomy for distal tibial vessels. The angiographic result was surprising to the operators, demonstrating a result that was previously thought to be unachievable with an angioplasty-only technique.
In this case, we used an undersized POBA to predilate for easy delivery of the Serranator, allowing the Serranator to do the bulk of the work for a long-term durable outcome. My strategy with extremely distal lesions is to perform a less aggressive POBA followed by the Serranator to achieve an optimized luminal gain, controlled dissection, and reduced recoil.
The patient continued with wound care managed by the podiatrist and clinical follow-up visits by vascular surgery. A photograph taken at 3 months post procedure shows a healed wound, achieving limb salvage (Figure 7). This result was impressive considering the initial presentation of a large wound and the patient’s high-risk comorbidities of longstanding end-stage renal disease and diabetes.

This case is sponsored by Cagent Vascular.
---
Q&A With the Operator
Robert J. Meisner, MD, FACS
How important is avoiding dissection for successful treatment of below-the-knee (BTK) arteries? Do you see a difference in performance between the Serranator and a plain angioplasty balloon (POBA)?
 Preventing a dissection in the BTK arteries is extremely important. We have limited bailout options in the event of a flow-limiting dissection in the tibial anatomy. For this reason, the controlled dissection along with exceptional lumen gain seen with the Serranator becomes incredibly important and has been one of the major reasons we have been happy with serration angioplasty. We have become huge believers in this mechanism of action.
Preventing a dissection in the BTK arteries is extremely important. We have limited bailout options in the event of a flow-limiting dissection in the tibial anatomy. For this reason, the controlled dissection along with exceptional lumen gain seen with the Serranator becomes incredibly important and has been one of the major reasons we have been happy with serration angioplasty. We have become huge believers in this mechanism of action.
When it comes to recoil, what have you observed when using a Serranator versus when using POBA?
I have not seen significant recoil after tibial angioplasty with the Serranator. I believe it physically alters the vessel and thereby increases vessel compliance and minimizes recoil.
What makes the Serranator different?
The most important differentiation is that the results have been very predictable and consistent in creating a robust lumen gain. The device has worked well on calcium, with the serrated edges being instrumental in creating a controlled angioplasty result.
How do you utilize the Serranator?
The Serranator balloon has earned room on our shelf. We have been using it often in conjunction with a pre-dilation and in some cases as a standalone therapy in the tibials. In many cases, the Serranator has replaced tibial atherectomy. In the femoral-popliteal segment, however, I use the Serranator balloon as a vessel prep followed by a drug-coated balloon. Overall, we have been very happy with its performance.
Find More:
Bilateral Lower Extremity Treatment With the Serranator PTA Serration Balloon Catheter
Total Vessel Imaging With the Gentuity High-Frequency Optical Coherence Tomography System
