


Peripheral Vision: Evaluating Vascular Procedures in Ambulatory Surgery Center (ASC) Settings
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Joyce Froetschel
Account Manager, Corazon, Inc.
Corazon is the national leader in program development for the heart, vascular, neuroscience, spine, orthopedic, and surgical service lines, offering services in consulting, recruitment, interim management, and accreditation. Corazon provides a full continuum of consulting, software solution, recruitment, and interim management services for hospitals, health systems and practices of all sizes across the country and in Canada. To learn more, visit www.corazoninc.com or call (412) 364-8200. To reach the author, email jfroetschel@corazoninc.com.
Navigating the delivery of patient care related to peripheral vascular procedures can be complex. While advancements in technology, improvements in patient outcomes, and expanding reimbursement have opened new opportunities, it’s important to note that peripheral vascular procedures are typically adjunctive offerings within ambulatory surgery centers (ASCs) that already perform cardiac interventions. The establishment of an ASC dedicated exclusively to peripheral vascular procedures is relatively rare, as reimbursement rates tend to be slightly more favorable in physician-owned office-based labs (OBLs). This financial advantage makes OBLs a more attractive setting for performing peripheral vascular intervention compared to ASCs. Therefore, for providers already engaged in coronary work within an ASC setting, integrating peripheral vascular procedures may represent a strategic extension of services. Determining whether this transition is right for your practice requires careful consideration of multiple factors and a thoughtful approach. When incorporating peripheral vascular intervention procedures into an existing ASC, it is important to carefully evaluate the feasibility of a hybrid lab model. This approach involves operating the lab as an ASC on days when procedures are more financially advantageous in that setting, and as an OBL on days when procedures such as peripheral vascular interventions yield higher reimbursement in an OBL environment. However, implementing a hybrid model requires the facility to function as two distinct entities, with no overlap in services. This separation entails maintaining completely independent documentation, including patient records, policies and procedures, and even signage. Due to the operational complexity, a thorough assessment of projected procedure volumes and a detailed financial analysis should be conducted to determine whether the hybrid model offers a sustainable financial benefit.
Source: Clinical & Operational Benchmarking Survey. Ambulatory Surgery Center Association. 2025. Accessed August 22, 2025. https://www.ascassociation.org/asca/asc-operations/benchmarking/clinical-ops
Financial Considerations
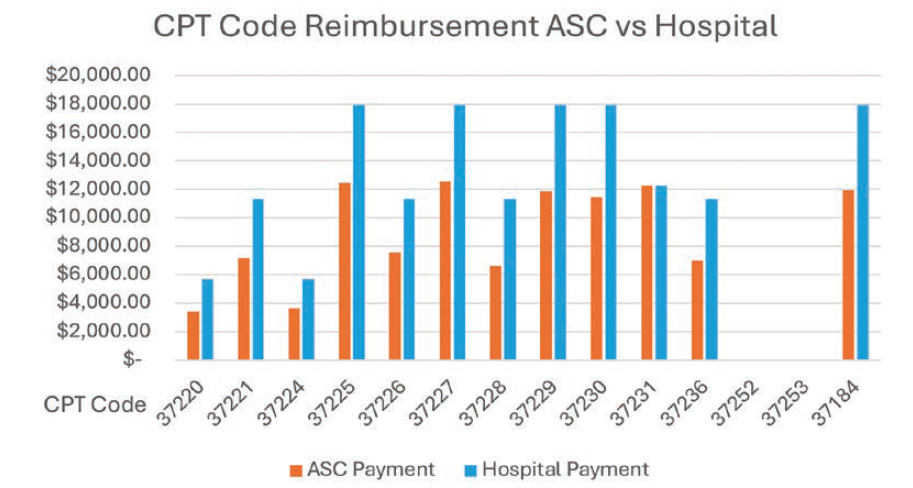
At first glance, reimbursement rates for peripheral vascular interventions appear significantly higher in hospitals compared to ASCs (Figure 1). Looking at the reimbursement alone may suggest that hospitals are the more profitable setting. However, a deeper analysis reveals that ASCs can offer a compelling financial advantage.
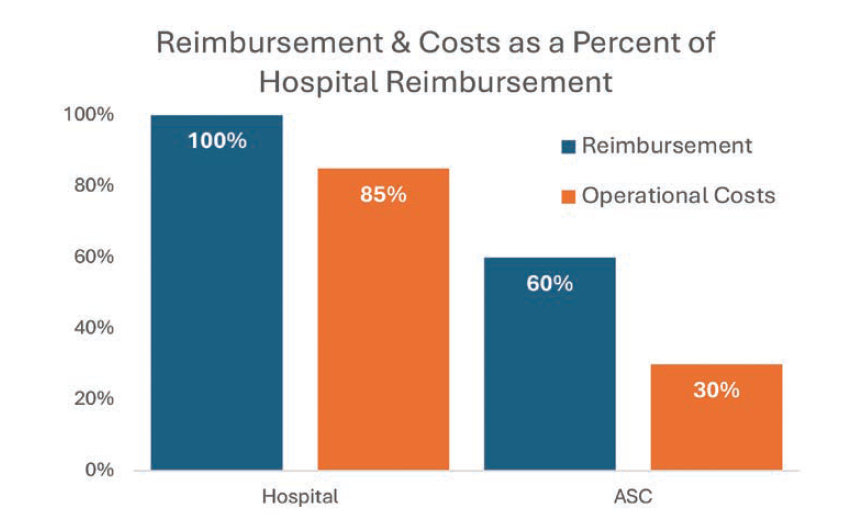
Hospital reimbursement rates account for their higher operational (expense) overhead. In contrast, ASCs — when efficiently managed — can achieve higher profit margins despite lower reimbursement rates, thanks to leaner operations and more effective resource utilization.1 The graph in Figure 2 illustrates how ASC operational costs are approximately 50% of the reimbursement, and conversely, departmental costs in the hospital setting are almost 85% of the reimbursement figure, leaving much leaner operating margins in the hospital setting.
Source: Church M, Serwer B, Needleman M, Thomas S. Strategies for maximizing cardiovascular profitability. Corazon Spring Conference: Healthcare Highway: The Right Lane for Service Line Success. Held May 1-2, 2025; Walter E. Washington Convention Center, Washington, DC.
Market Analysis
The first step in evaluating the feasibility of moving peripheral vascular intervention (PVI) procedures to an ASC is conducting a thorough market analysis. This analysis will answer the question of whether there is a viable patient population to support a PVI procedures program.
An estimated 12-14% of the global population, including 8 million Americans, suffer from PAD.2 Over 12 million Americans are currently affected by peripheral arterial disease (PAD), and among individuals over the age of 75, the prevalence increases to 20%.3 Sixty-three percent of vascular patients have coronary artery disease (CAD), and one-third of CAD patients have PAD.3
These statistics present a compelling case for cross-modality patient screenings. Although peripheral vascular disease is a chronic condition, it often remains undiagnosed until it becomes critical, necessitating complex treatments or even amputation. There is a clear shortage of individuals undergoing screening, and a possible lack of providers and locations where these patients can receive supportive treatment, including PVI. However, while the data suggests strong demand, the decision to shift peripheral interventional procedures to an ASC remains complex and multifaceted.
The first requirement is to assess local demographics. Are patients in your area meeting clinical eligibility for outpatient care? Many individuals with peripheral vascular disease are elderly and have comorbidities such as diabetes, kidney disease, or cardiovascular conditions that may necessitate hospital-based treatment. A comprehensive patient evaluation is essential to identify risk factors and determine the appropriateness of ASC-based care.
Other important considerations include:
• Social determinants of health: race, ethnicity, socioeconomic status, and potential healthcare disparities.
• Local competition: Are other facilities offering similar services? Are they meeting demand or leaving gaps in care?
A detailed market assessment reviews the exact number of PVI procedures in your geographic area that receive treatment, regardless of which facility or provider performs the care. It is important to map and quantify the outmigration of PVI cases that are occurring, but this can be challenging, as most PVI procedures are already conducted on an outpatient basis. Corazon has found significant gaps in the availability of outpatient market information versus inpatient data. Completing the best possible market assessment will help define the regional landscape and patient needs.
State Regulatory Environment
State regulations can play a critical role for the expansion of procedures in an ASC or if you are considering starting an ASC from the ground up. Is your state a Certificate of Need (CON) state?4 Are there restrictions on the types of procedures allowed in ASCs? For example, in Corazon’s home state of Pennsylvania, any procedure on the Medicare Covered Procedure List (CPL) for an ASC is permitted to be performed in that setting with minimal regulatory oversight that includes adherence to strict state-regulated building and operational requirements. What are the building and operational requirements for your particular state? State-specific guidelines, such as those from the Pennsylvania Department of Health or the Michigan Department of Community Health, as well as local building departments and zoning boards, may outline requirements for developing an ASC. However, due to the complexity and regional nuances involved, it is strongly recommended to engage an architectural firm with experience in ASC design within the proposed geographic area. These firms are well-equipped to navigate the intricacies of regulatory compliance, including the separation of documentation, patient records, policies, and signage when dual-use models are considered. Some states have fewer regulatory hurdles, making ASC procedural expansion more attractive. Understanding your state’s specific requirements is essential, as these regulations will shape the planning and development process.
Facility and Infrastructure
Once market viability is established, the next step is to evaluate the physical and logistical aspects of a peripheral vascular ASC:
• New construction vs. renovation: Will the ASC be a new build, a conversion, or part of a hospital campus?
• Proximity to emergency services: Access to a full-service hospital is crucial for patient safety when managing cardiovascular conditions.
• Design and compliance: Engage architects familiar with ASC development, which includes state regulatory requirements and Facility Guidelines Institute (FGI) guidelines. Include a designer who is familiar with the unique workflow of an interventional suite. Involving clinicians in the design process to ensure the space meets procedural needs is essential.
• Expansion opportunities: Include the potential of additional services such as renal denervation and cardiac procedures.
The number and size of procedure rooms should align with the projected market demand as described in your completed market analysis.
Equipment and Capital Investment
Capital equipment is a major cost driver. Outfitting a single peripheral vascular lab can exceed $2 million. However, cost-saving opportunities for ASCs do exist:
• Scaled-down or refurbished imaging systems from vendors like Philips, Siemens, and GE.
• Lower-cost product lines for catheters, balloons, and stents.
• Consignment agreements and ASC-specific contracts with your supply-chain vendors that reduce upfront costs.
Often, a start-up ASC will build shell space for two interventional labs, but outfit only one of those labs with the capital equipment necessary for PVI. This bolsters a strategy for the future installation of the equipment in the second lab as procedure volumes increase.
Understanding these aforementioned options can significantly reduce startup expenses.
Administrative and Operational Planning
Establishing a strong administrative foundation is not only key but a requirement for any new ASC to achieve accreditation that remains compliant with Centers for Medicare and Medicaid Services (CMS) payment mandates. The following operational parameters are the necessary foundational components to be outlined throughout the implementation process of any new ASC:
• Governance structure: Define leadership roles and reporting lines between the physician leaders and the administrative leaders (eg, nursing executive administrator) with a clear delineation of shared responsibilities.
• Emergency protocols: Build and document relationships with local hospitals and EMS providers in case of potential emergent transfer.
• Scope of services: Delineation of case types must be documented to both the ASC team and any regulatory bodies to ensure there is no confusion on the cases being performed. The ASC may consider offering complementary procedures to maximize utilization of the procedural space, which will also need to be validated against the delineation of procedures done sporadically (ie, “not less than annually”).
• Physician compensation: Outline the number of physicians [interventionalists] needed. Are they owner/operators or employed? Diligent ASC operators will research the market to ensure competitive compensation packages. The range of compensation for a physician provider is usually greater than $500k, and can create inequities among physicians where ASC procedures have decreased reimbursement (vs. hospital rates).
• Staffing: Anticipated capacity (room) needs will be forecasted using the volumes from the market analysis. This will also help to determine the appropriate mix (ie, RNs, RTs, MAs, etc.) and the correct full-time employees (FTEs) of staff. Competitive ASCs have budgets for competitive salaries, benefits, paid time off, and leave.
• Quality: Implementation of a strong quality program will ensure the best patient outcomes. Options include an internal audit process and participation in a clinical data registry such as VQI (Society for Vascular Surgery’s Vascular Quality Initiative). Outsourcing for external peer review should also be part of the quality program.
• Cath lab accreditation: Quality recognition is attractive to patients, providers, and staff, and provides greater reimbursement / decreased expense potential.
• Outsourcing services: Evaluation should be conducted to determine if engaging outside services for payroll, coding, and billing will alleviate the added expense and time commitment of administrative tasks.
• Facility and equipment maintenance: Determining whether the maintenance will it be onsite (ie, direct employment) or a contracted service is key. Maintenance support must include plant operations, bio-medical, capital equipment such as imaging systems, and software upgrades.
• Software and databases: Software that assists with EMR / data reporting to registries represents an initial expense that can be significant. The newly opened ASC must also budget for ongoing upgrades.
• Indirect expenses: These are often not top of mind for those providers that have not experienced running their own practice(s). These expenses include office and cleaning supplies, operational expenses, and janitorial expenses.
Source: Clinical & Operational Benchmarking Survey. Ambulatory Surgery Center Association. 2025. Accessed August 22, 2025. https://www.ascassociation.org/asca/asc-operations/benchmarking/clinical-ops
Conclusion
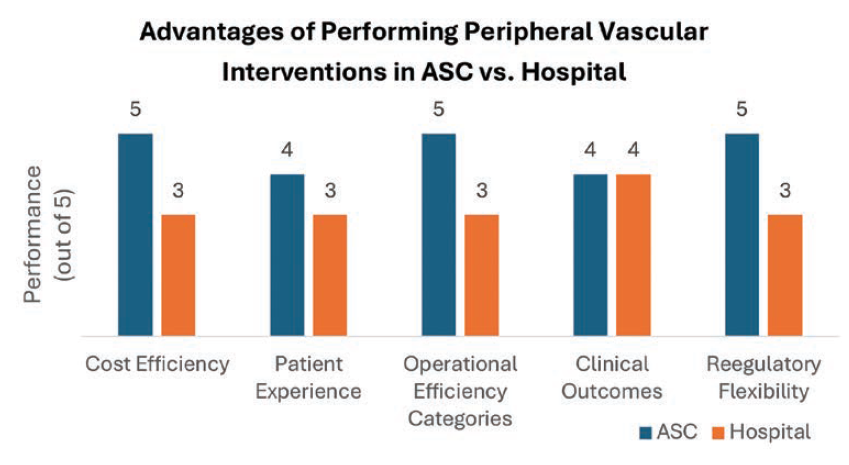
The operations of an ASC (vs. hospital setting) often benefit from more efficient workflows, fewer delays, and shorter patient stays, thus leading to higher patient satisfaction and often increased volumes over time.1 There are several factors contributing to the overall cost and potential profitability when opening a peripheral vascular program in an ASC setting, but if managed correctly, an ASC will outperform a hospital in cost efficiencies, patient experience, operational efficacy, and clinical outcomes (Figure 3).1
Corazon’s data collected from working with clients across the country reveals that the average direct cost per peripheral intervention ranges from $15,000 to $21,000, while the average contribution margin is between $4,600 and $10,500. Based on total cost data from Definitive Healthcare,1 these financial figures present a compelling argument for transitioning peripheral vascular services to the ASC setting.
In a 2023 report from healthcare analysis company Sg2, ASCs were projected to grow by 12% in five years and 22% in ten years.5 With this shift already underway, now is the time to evaluate your strategy.
References
1. Church M, Serwer B, Needleman M, Thomas S. Strategies for maximizing cardiovascular profitability. Corazon Spring Conference: Healthcare Highway: The Right Lane for Service Line Success. Held May 1-2, 2025; Walter E. Washington Convention Center, Washington, DC.
2. Cook Medical. “10 facts about peripheral arterial disease”. Accessed August 14, 2025. https://www.cookmedical.com/peripheral-intervention/10-facts-about-peripheral-arterial-disease/
3. Allison MA, Armstrong DG, Goodney PP, et al; American Heart Association Council on Peripheral Vascular Disease; Council on Hypertension; and Council on Lifestyle and Cardiometabolic Health. Health disparities in peripheral artery disease: a scientific statement from the American Heart Association. Circulation. 2023 Jul 18; 148(3): 286-296. doi:10.1161/CIR.0000000000001153
4. 50-State Scan of State Certificate-of-Need Programs National Academy for State Health Policy. Accessed August 14, 2025. https://nashp.org/state-tracker/50-state-scan-of-state-certificate-of-need-programs/
5. Summer report forecasts significant growth in ASC volume in the next 10 years. Outpatient Surgery Magazine, A Division of AORN. Published August 21, 2023. Accessed August 14, 2025. https://www.aorn.org/outpatient-surgery/article/summer-report-forecasts-significant-growth-in-asc-volume-in-the-next-10-years
Sources
1. Church M, Newell A. A shift in cardiovascular care: ambulatory surgery centers (ASCs), peripheral arterial disease (PAD), and peripheral vascular interventions (PVI). Cath Lab Digest. 2024 Feb. Accessed August 22, 2025. https://www.hmpgloballearningnetwork.com/site/cathlab/cath-lab-management/shift-cardiovascular-care-ascs-pad-and-pvi
2. Gornik HL, Aronow HD, Goodney PP, et al; Peer Review Committee Members. 2024 ACC/AHA/AACVPR/APMA/ABC/SCAI/SVM/SVN/SVS/SIR/VESS Guideline for the Management of Lower Extremity Peripheral Artery Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024 Jun 11; 149(24): e1313-e1410. doi:10.1161/CIR.0000000000001251
3. Mihatov N, Secemsky EA. Peripheral and coronary artery disease: two sides of the same coin. American College of Cardiology Cardiology Magazine. September 20, 2019. Accessed August 22, 2025. https://www.acc.org/latest-in-cardiology/articles/2019/09/14/24/42/peripheral-and-coronary-artery-disease-two-sides-of-the-same-coin


