


Right Distal Radial Artery Access for Cardiac Cath: Just a Fad?
 Distal radial access (DRA) has become increasingly popular for vascular access. Since being brought to the forefront by Dr. Ferdinand Kiemeneij several years ago, specifically for left radial procedures, DRA has been one of the most fashionable facets of vascular access to study, and in fact, several studies have demonstrated DRA to be safe and feasible.1-3
Distal radial access (DRA) has become increasingly popular for vascular access. Since being brought to the forefront by Dr. Ferdinand Kiemeneij several years ago, specifically for left radial procedures, DRA has been one of the most fashionable facets of vascular access to study, and in fact, several studies have demonstrated DRA to be safe and feasible.1-3
There have been a few points of contention regarding which approach (distal or conventional radial access) offers lower rates of radial artery occlusion (RAO), access-site crossover, hemostasis time, and access-site related complications. Recently published and presented at EuroPCR, the DISCO RADIAL study sought to assess the superiority of distal compared with conventional radial access with respect to forearm RAO. Researchers found that with a rigorous hemostasis protocol, distal and traditional radial artery access have equally low RAO rates. DRA is associated with a higher crossover rate, but a shorter hemostasis time.1 Shorter hemostasis times can potentially get patients out of the hospital sooner and require less post-operative care. Another study found that RAO occurred in 4.8% (41/837) of patients undergoing standard radial access and in 0% (0/326) of those undergoing the distal approach (P<.0001). DRA was associated with higher percentage of flow preservation (97.2% vs 78.5% in the transradial access group, P<.0001) and reduced time to hemostasis (147±99 minutes [min] vs 285±138 min, P<.0001).2 The RATATOUILLE study found hand function post DRA procedures was not associated with hand function impairment.3 DRA may also spare the radial artery for fistula implantation in the future should patients need it and be used to recanalize a previous RAO.
The conventional right radial artery (RRA) has been and remains the preferred access route for interventional cardiologists due to longstanding practices, familiarity working from the right side of the catheterization table, and standard historical laboratory equipment configurations.4 Aside from shorter hemostasis times (and possible decreased rates of RAO), are there other reasons to consider use of the right distal radial access (RDRA) versus traditional forearm access?
Operator Radiation Exposure and Ergonomic Rationale (Interventionalists and Patients)
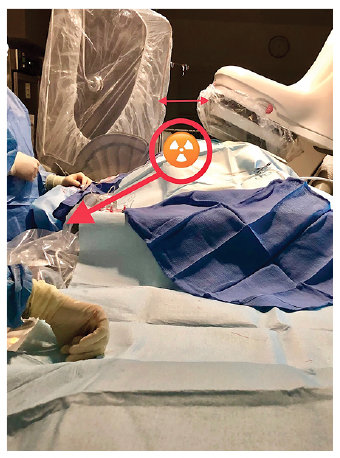
Operator radiation exposure is one of the biggest occupational health hazards faced by interventional cardiologists. Significant dose reduction to the operator was observed with the right arm situated close to the body versus arm setup further away from the body (110.4 µSv abducted vs 46.1 µSv adducted P=.02) in the RAD-MATRIX study. Interestingly, this significant dose reduction was achieved with only a very small adjustment to patient and equipment setup.5 If we look deeper into the mechanisms for dose reductions in the RAD-MATRIX study, two key factors emerge. The first is better apposition between the ceiling-mounted shield and the patient (and improved protection for the operator). With an abducted right arm, the shield typically lies over the arm, leaving a window of scatter radiation directed towards the operator (Figure 1).
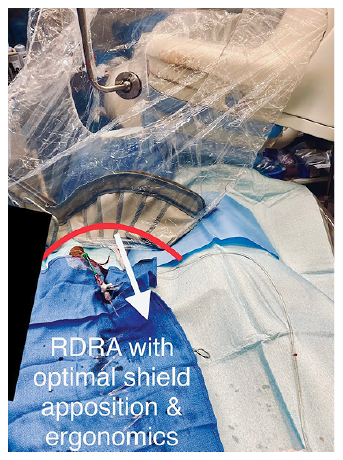
An adducted right arm/wrist situated closer to the right femoral access site will promote better shield apposition to the patient and reduced radiation exposure to the operator (Figure 2). The second factor is that an adducted arm/wrist increases the distance between the operator and the radiation source. This distance (2-3 inches) may seem small. However, as radiation exposure is cumulative, 2-3 inches of distance multiplied by 1000 procedures has a significant long-term dose-reduction effect. While the patient’s arm abducted is commonplace for many conventional radial access procedures, operators may also be exposed to additional radiation if the table-mounted lead shield does not reach far enough to protect the operator from radiation under the table.6
With the use of RDRA, it is much easier to position the arm close to the body without compromising patient comfort. With the hand supinated and secured in place, patients become increasingly uncomfortable while maintaining adduction close to the body. When the arm moves toward the right flank, the hand naturally pronates, therefore, the positioning required by a RDRA can be more convenient for patients. This may be especially true for obese patients that have excessive axillary adipose tissue, because it becomes increasingly difficult to adduct the arm with the hand in a supinated fashion as required for a conventional radial access procedure. Using RDRA can consistently bring the patient’s arm close to the body so operators can gain a radiation reduction advantage in a population that generates the largest amount of occupational exposure.
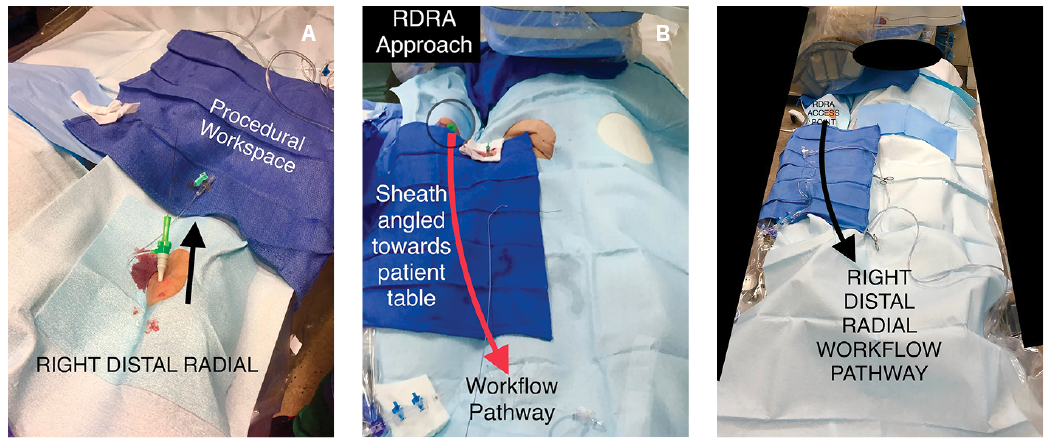
Ergonomically, using RDRA does something interesting for operators. The “angle of attack” of the needle and wire entry create an ergonomic workflow pathway that biases catheters over the patient table (Figure 3A-C), potentially eliminating the need for dedicated radial boards and equipment. It also allows for the patient table to be a working platform, providing significantly more working space than any specialized apparatuses. The setup is almost identical for cath lab staff, so any learning curve is minimal. One disadvantage is that cath labs would need to keep 125 cm catheters on hand to accommodate taller patients and/or patients that have significant tortuosity in the right upper extremity and subclavian.
Discussion
Dr. Karsten Schenke, an interventional cardiologist in Hamburg, Germany, commented, “Conventional right radial has been my go-to for some time now, with right distal being a bailout for patents with renal failure and orthopedic issues. Left distal is my standard with previous right RAO and coronary artery bypass graft surgery patients with a left internal mammary graft.” He goes on to say, “After talking to some enthusiastic distal radial operators during the German Cardiac Society meeting, I transitioned to RDRA as my standard access. The transition was smooth, with good puncture times and little crossover rate.” Not all interventional cardiologists see RDRA with the same enthusiasm. One possible reason is limited data supporting an access site. Another might be a reluctance to change after successful use of the conventional radial approach.
Interventional cardiologist Dr. Robert Yeh from Beth Israel Deaconess Medical Center in Boston, Massachusetts, said, “I tend to use left distal frequently, particularly in our dual access chronic total occlusions (CTOs), where the improved ergonomics really help since cases are long. I haven’t moved to RDRA, since ergonomics are less of an issue, and the stick tends to be a little more difficult and time consuming.”
Professor of Interventional Cardiology Dr. Jim Nolan, at the University Hospital of North Midlands in the United Kingdom, noted, “Conventional proximal radial access is a well-established access technique supported by a large body of favorable data. But the interventional community is always looking to improve the procedure. Distal radial access has a number of theoretical and practical advantages over the conventional technique, and initial data suggests excellent outcomes for this innovation. As more data accumulate, many operators will be motivated to move to routine distal access. The potential to reduce operator radiation exposure through the operation of the inverse square law is a particularly important benefit of distal radial access.”
For many, a distal radial approach makes the most sense for a left extremity procedure. There are several documented advantages from the left radial approach (LRA) when compared with the right, such as reductions in fluoroscopy time, contrast dose, operator radiation exposure, and stroke reduction.7-10 These advantages have been primarily attributed to better shield apposition during an LRA procedure and less tortuosity from the LRA approach when compared to a right radial approach. However, left distal’s desired advantage is the creation of an ergonomic working atmosphere for the operating physician. The hub of the sheath is not hidden in the drapes because of overpronation of the patient’s left hand, and the operator does not have to lean across the table to manipulate catheters and equipment. If set up properly, the hub is secured at the patient’s midline axis (Figure 4).

In a recent Twitter poll (n=85), 24% of respondents said they use right distal access regularly, while 11% said they will only use it for patients with orthopedic problems. Sixty-five percent of respondents found standard radial access to be satisfactory or indicated that they do not see the point of right distal access. While a Twitter poll is clearly not the best indicator to determine the uptake of distal right access, it was used to get an idea of the existing opinions of some cath lab physicians and staff.
Physicians and staff may be resistant because they are comfortable with the setup and ergonomics from the standard right radial approach and are reluctant to change from longstanding practices that work. A United States Navy rear admiral coined the phrase, “the most dangerous phrase in the English language is ‘we’ve always done it this way.’” Our goal is not to promote one access point over the other, but to point out the need to remain vigilant in seeking out best practices, regardless of whether something has worked well for a long period of time.
Conclusion
While the right distal radial artery approach is still teetering on the verge of popularity (or obscurity), it remains to be seen if operators will take up this approach as a primary access point. It has not yet been embraced the same as its “contralateral counterpart.” Currently, the major advantage for RDRA is its shorter time to hemostasis. Secondarily advantageous are the reduction in operator radiation exposure and ergonomic advantages.
Distal radial access emblematizes the innovative access techniques that emerge in the field of interventional cardiology. Ultimately, it is up to operators if they want to change practice from conventional radial access.
Special thanks to Drs. Karsten Schenke, Robert Yeh, and Jim Nolan for contributing.
Disclosures: Richard Casazza reports he is Director of R&D for Tesslagra Design Solutions.
Richard Casazza, MAS, RT(R)(CI), can be contacted at all4ugq@aol.com or on Twitter at @Tesslagra.
References
1. Aminian A, Sgueglia GA, Wiemer M, et al. Distal Versus Conventional Radial Access for Coronary Angiography and Intervention: The DISCO RADIAL Trial. JACC Cardiovasc Interv. 2022 Jun 27; 15(12): 1191-1201. doi: 10.1016/j.jcin.2022.04.032
2. Pacchioni A, Mugnolo A, Sanz Sanchez J, et al. Radial artery occlusion after conventional and distal radial access: Impact of preserved flow and time-to-hemostasis in a propensity-score matching analysis of 1163 patients. Catheter Cardiovasc Interv. 2022 Feb; 99(3): 827-835. doi: 10.1002/ccd.30005
3. Sgueglia GA, Hassan A, Harb S, et al. International Hand Function Study Following Distal Radial Access: The RATATOUILLE Study. JACC Cardiovasc Interv. 2022 Jun 27; 15(12): 1205-1215. doi: 10.1016/j.jcin.2022.04.023
4. Rao SV, Cohen MG, Kandzari DE, et al. The transradial approach to percutaneous coronary intervention: historical perspective, current concepts, and future directions. J Am Coll Cardiol. 2010 May 18; 55(20): 2187-2195. doi: 10.1016/j.jacc.2010.01.039.
5. Sciahbasi A, Frigoli E, Sarandrea A, et al. Determinants of radiation dose during right transradial access: Insights from the RAD-MATRIX study. Am Heart J. 2018 Feb; 196: 113-118. doi: 10.1016/j.ahj.2017.10.014.
6. Casazza R, Truesdell AG. Hyper Adducted Right Radial Artery (HARRA) method to reduce radiation exposure and promote ergonomics. Cath Lab Digest. 2020 Apr; 28(4): 20-25. Accessed August 16, 2022. https://www.hmpgloballearningnetwork.com/site/cathlab/content/hyper-adducted-right-radial-artery-harra-method-reduce-radiation-exposure-and-promote-ergonomics
7. Xia SL, Zhang XB, Zhou JS, Gao X. Comparative efficacy and safety of the left versus right radial approach for percutaneous coronary procedures: a meta-analysis including 6870 patients. Braz J Med Biol Res. 2015 Aug; 48(8): 743-750. doi: 10.1590/1414-431X20154571
8. De Rosa S, Torella D, Caiazzo G, et al. Left radial access for percutaneous coronary procedures: From neglected to performer? A meta-analysis of 14 studies including 7603 procedures. Int J Cardiol. 2014 Jan 15; 171(1): 66-72. doi: 10.1016/j.ijcard.2013.11.046.
9. Sciahbasi A, Romagnoli E, Burzotta F, et al. Transradial approach (left vs right) and procedural times during percutaneous coronary procedures: TALENT study. Am Heart J. 2011 Jan; 161(1): 172-179. doi: 10.1016/j.ahj.2010.10.003.
10. Rashid M, Lawson C, Potts J, et al. Incidence, determinants, and outcomes of left and right radial access use in patients undergoing percutaneous coronary intervention in the United Kingdom: a national perspective using the BCIS dataset. JACC Cardiovasc Interv. 2018 Jun 11; 11(11): 1021-1033. doi: 10.1016/j.jcin.2018.01.252.


