


The Consensus for Intravascular Ultrasound Use in Peripheral Vascular Intervention
This article has been updated from the print version to reflect the publication of the global consensus study.
What is intravascular ultrasound, and why is it important to the diagnosis and treatment of peripheral vascular disease?
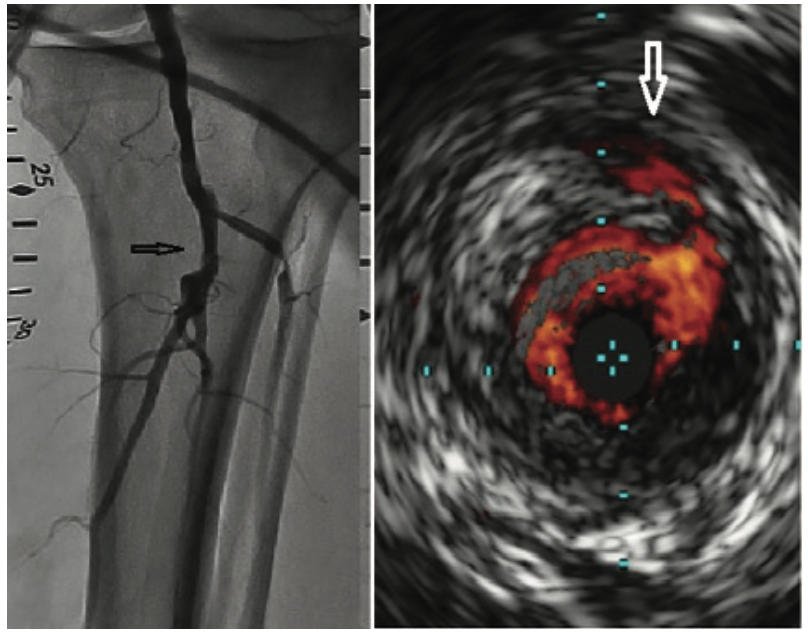
Intravascular ultrasound (IVUS) is an imaging device that provides a 3-dimensional view of what we normally see as a 2-dimensional vascular structure. The device goes over a wire into the vessel, and allows us to see the characteristics inside the vessel looking outward, including the vessel wall, some of the plaque that builds up in the vessel wall, the composition of the plaque, and other characteristics surrounding the vascular structure that are often missed with the 2-dimensional image from angiography (Figure 1). IVUS can be used in any vascular structure. We have been using it in coronary intervention for some time, but we can also use IVUS in the arteries of the lower extremities, in the aorta and other arterial branches, and in the venous system.
What are the limitations of angiography alone? What does IVUS add that is not seen on angiography?
When we take a picture of a vessel using 2-dimensional reconstruction, it lacks some of the details necessary for making an accurate assessment in terms of how to proceed and optimize a revascularization procedure. For example, on the arterial side, we often rely on calcium showing up on an x-ray image, but often that calcium is either not visible due to underlying structures like bone, muscle, or tissue, or it is not completely captured in the angiographic view. IVUS allows us to better see the degree of calcium in the vessel. It is the same issue for a lesion. In some views, a lesion can look moderate or mild. In some views, a lesion can look severe. If you don’t take the right view, then you may be unable to classify the severity of that lesion. An intravascular imaging device allows us to see the severity of the actual disease compared to what the vessel should look like when evaluated with a normal reference. We can understand the composition of the disease and how to treat it. Intravascular imaging is in an evolving role for the lower extremity space. The question is how do we use it, not necessarily to replace angiography, but to complement angiography, and to provide a more meaningful and complete picture in regards to determining how best to revascularize and optimize treatment for our patients with peripheral vascular disease.
At the 2021 Vascular InterVentional Advances (VIVA) meeting, you presented the results of the first global consensus for the appropriate use of IVUS, as put together by 40 cross-specialty medical experts. Can you tell us about it?
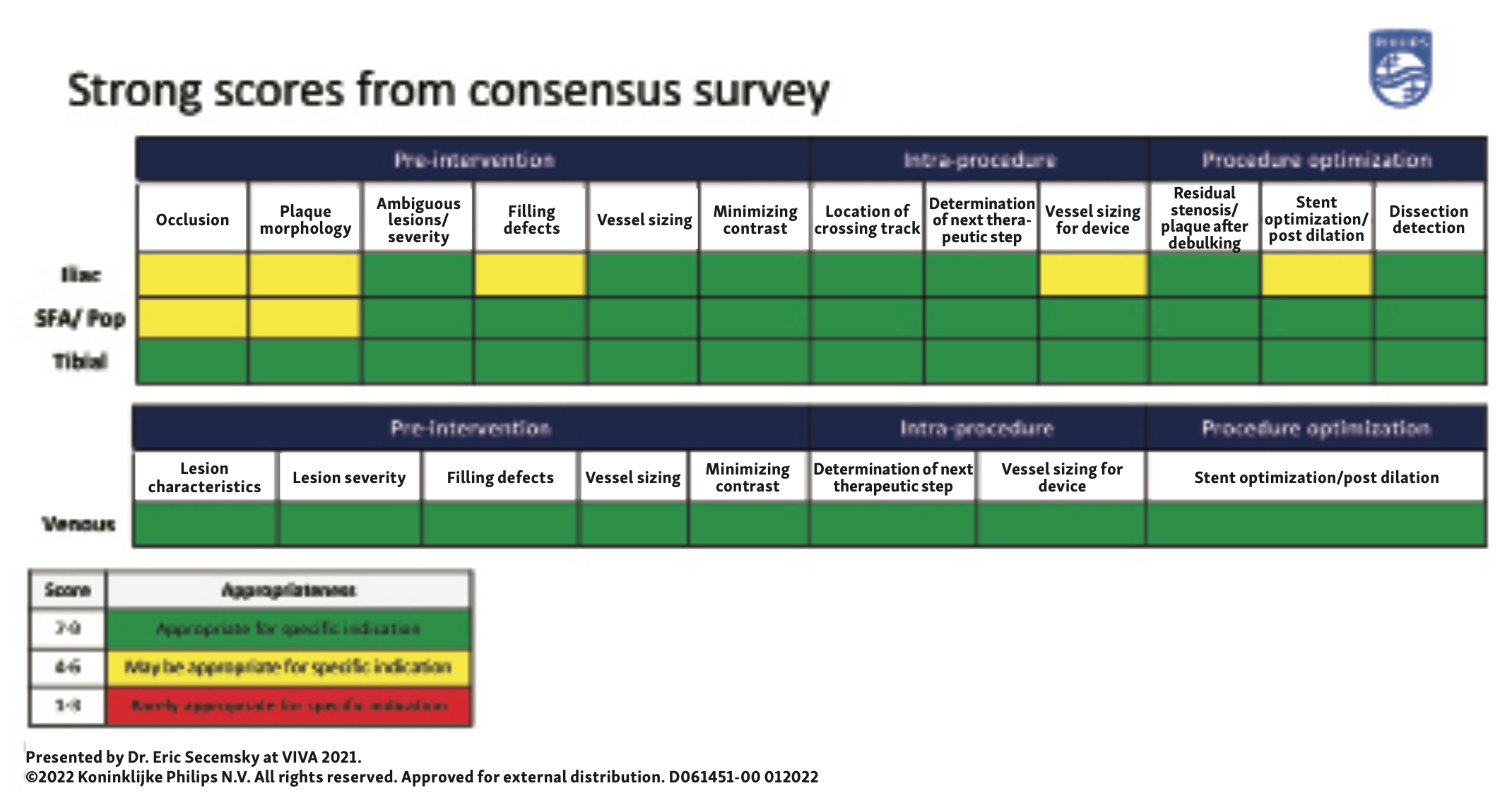
The global consensus document† is a novel approach to determining next steps on how to use intravascular imaging for peripheral revascularization. We have already seen the success of IVUS in the coronary space during percutaneous coronary intervention. We have a fair amount of observational cohort data examining the benefits of IVUS for lower extremity arterial and venous intervention. We have dedicated peripheral imaging catheters that have been developed specifically to guide lower extremity arterial and venous revascularization. Yet we have not seen a clear document outlining where IVUS technology can be particularly useful. As we have continued to build the evidence around IVUS and how it is meaningful in the treatment of our patients, it is important to supplement that evidence with expert opinion that captures how IVUS has been used and where it can best be used. We were able to develop a consensus document that was independent of external influence and involved a core group of 12 physician leads, who all are specialists in either peripheral vascular disease or intravascular imaging. This core group represents multiple disciplines, including vascular surgery, interventional radiology, interventional cardiology, vascular medicine, and angiology, and is representative of many locations, both inside and outside of the United States. We put together an exhaustive list of clinical scenarios where IVUS may or may not be useful, and allowed our experts to decide. We curated two different surveys, one looking at lower extremity arterial revascularization, and one looking at lower extremity venous revascularization. We then found 15 experts on the arterial side and 15 experts on the venous side, nominated based on their experience in the peripheral vascular space, diverse clinical specialties, and geographic locations inside and outside the United States. These experts were blinded to each other and to us, and were asked to complete this survey and present their opinion of when IVUS can be most useful. On the arterial side, the survey was divided based on the arterial segment involved: iliac, femoropopliteal, and tibial. On the venous side, the survey focused on iliofemoral venous intervention. We compiled the results and shared them with each of the two groups, arterial and venous separately, to come to a full consensus where everyone was in agreement.
For iliac arterial revascularization, the majority of the operators who participated in the survey considered IVUS an important adjunct to iliac intervention. For clinical scenarios involving the preprocedural phase, such as determining the plaque morphology or filling defect where it may not be clear, there was more of a range of opinions, summarized by determining that IVUS “may be appropriate” in these scenarios. However, IVUS was considered to be particularly useful for delivering definitive therapy like stent implantation and evaluating post intervention for issues like haziness at the end of the stent. In the femoropopliteal segment, this expert panel again felt that IVUS “may be appropriate” for clarifying filling defects and understanding plaque morphology. IVUS was felt to be “appropriate” for delivering definitive therapy and optimizing femoropopliteal intervention care. Remarkably, in the tibial vessels, IVUS was found to be appropriate across the entire survey. We also see this in our own practice, that IVUS can be useful for every step of the procedure, in particular, sizing the vessels appropriately, because we tend to undersize tibial vessels based on angiography alone. IVUS was universally felt to be critical for delivering definitive therapy and ensuring that our therapy was delivered safely.
In summary, for the arterial side of the survey, experts supported IVUS use throughout lower extremity arterial revascularization, independent of the arterial segment. The strongest support for IVUS use in all phases of intervention was in the tibial vessels, while IVUS was felt to be more consistently appropriate for the iliac and femoropopliteal arterial segments in the intraprocedure and post procedure phases.
On the venous side, with a separate expert panel of 15 operators representing a diversity of clinical specialties and blinded to each other when completing the survey, there was near-unanimous agreement that IVUS was appropriate and would improve procedural outcomes. This includes more definitively answering questions like, how severe is the lesion? What is the cause of extrinsic compression? Where is the reference vessel that is normal or abnormal to land your definitive therapy? Operators were in agreement that IVUS was appropriate at every phase to further define next steps and also to conclude the revascularization procedure.
In this consensus survey, we learned that there are specific clinical scenarios still requiring work in order to determine the exact role for IVUS. More importantly, we learned that the current sentiment across operators participating in revascularization procedures in the lower extremities is that IVUS is strongly supported, has a role in many if not all of our revascularization procedures, and that it is strongly endorsed by this group of global experts. We believe this consensus document is timely and will have a meaningful impact on clinical care.
Your consensus survey presentation at VIVA was followed by the largest ever real-world clinical analysis on IVUS use in lower extremity peripheral intervention at the 2021 Transcatheter Cardiovascular Therapeutics (TCT) meeting. Can you share more about those results?
Before creating our survey, we did a systematic review1 of the literature that helped inform our consensus document. We found that there were a number of studies evaluating IVUS-guided intervention versus standard of care, but most were cohort studies that were small in size. Some were from 2000s and a few were more contemporary. We thought we could supplement these data with a contemporary, national evaluation of the role of IVUS in determining outcomes in lower extremity arterial and venous interventions, and did an analysis (in press) of a several-year span of Medicare data across the United States, looking at all lower extremity arterial procedures performed.
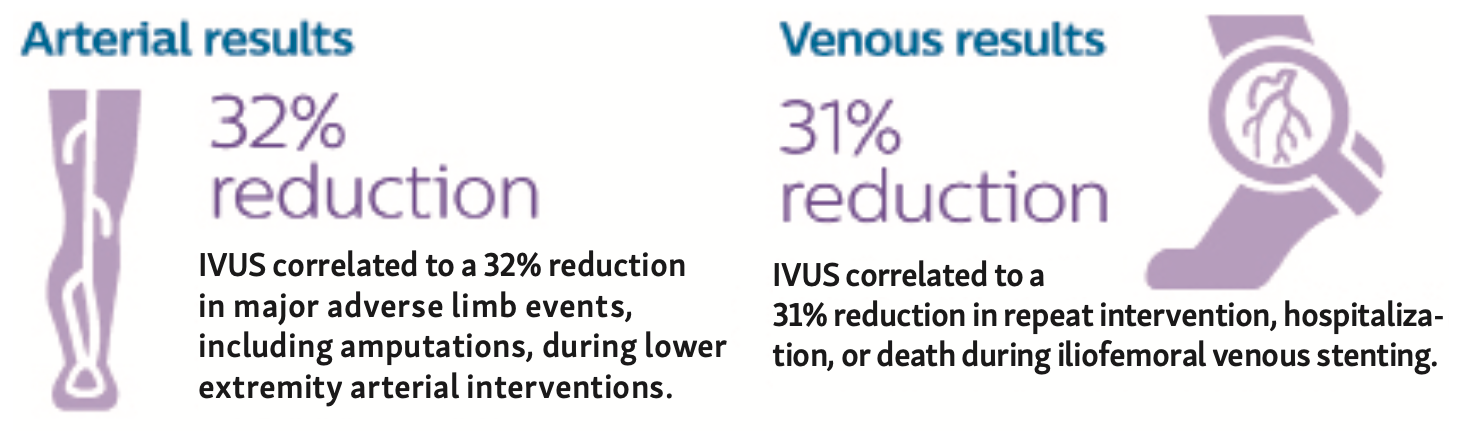
On the arterial side, we looked at everyone who had a lower extremity arterial intervention in the last four years. We looked at where they were revascularized, (iliac, femoropopliteal, and tibial intervention), their presenting diagnosis (chronic limb-threatening ischemia [CLTI] versus claudication versus other), and where the patient underwent the procedure (in the hospital, in a hospital outpatient center, or in a privately owned clinic). We then evaluated what the outcomes looked like compared with a matched population of people who did not have IVUS as part of the revascularization strategy. What we found on the arterial side was a ~30% reduction in major adverse limb events (Figure 2), defined as arterial thrombosis and embolism or major amputation, if IVUS was incorporated as part of that procedure. When we looked at it by arterial segment, by severity of presenting peripheral arterial disease (PAD) illness, or the location of where the patient was treated, we found a similar signal of safety if IVUS was utilized as part of the treatment strategy. With the use of IVUS, we also saw that people underwent less surgical intervention and seemed to have a longer, endovascular-based program for the revascularization of their peripheral arterial disease. What stood out was that IVUS was only used in ~12% of all procedures. I think that number should be at least three times that amount, if not higher. The amount of information we get from IVUS, the data now supporting the role of IVUS, and the expert consensus document have all shown that there are a lot of vulnerable patients who can benefit with IVUS-guided intervention. I see that number growing, but we are still in the infancy of IVUS use in this arterial bed.
On the venous side, we have seen a big explosion in the use of IVUS during iliofemoral venous intervention. We looked at that Medicare dataset for a population of patients undergoing deep venous stenting. Here, the majority who underwent deep venous stenting did have IVUS as part of their procedure. It is great to see consensus and clinical use go hand in hand. Probably everyone would benefit from IVUS-guided venous stenting, but there has been a nice evolution in how we do deep venous stenting, learning from past mistakes of stent embolization and other aspects of care that have suffered because of our reliance solely on 2-dimensional angiography imaging. We found that when IVUS was used as part of a deep venous stenting procedure, there was a reduction in important endpoints, including repeat intervention, hospitalization, and death. Notably, for more obscure and less well-characterized endpoints like stent embolization, which are captured poorly in prior studies because the rates of stent embolization are so small, we saw that when IVUS was used, there was a meaningful reduction in the risk of stent embolization.
These two studies nicely represent patients who we all treat in practice. The studies contain all our patients who are in the Medicare database. We looked at hundreds of thousands of patients on the arterial intervention side and just over 15,000 patients on the venous side. Size doesn’t mean quality necessarily, but the nice thing about the size of these databases is that it allows us to look at many different data cuts. Looking at different arterial segments, indications for peripheral artery disease, and the settings where patients were treated is only doable with a meaningful-sized cohort. It is one of the largest IVUS studies ever done and shows that IVUS, as part of a revascularization strategy, has a meaningful influence on both mid- and long-term outcomes for our patients. This large clinical analysis is a nice supplement and complement to the consensus document and other work done in this space.
When you think about these data collectively, how do you see this information influencing the use of IVUS by the interventional community?
We all feel like the time is now to start using this technology. We are in a unique situation where these devices are available and we have seen people using them, but we haven’t seen the widespread understanding that IVUS can have a significant influence on our procedures and our patients. We needed a tipping point of, “Now is the time to change our practice and start thinking about other ways to improve care.” This work will help us move that mentality forward. Remember, on the coronary side, we have spent a long time talking about the role of coronary IVUS and how it improves outcomes, and we have seen adoption increase. It has been slow, but for those people doing high-risk procedures, taking care of high-risk patients, working at large hospital systems, IVUS is now a mainstay of their practice. IVUS use is how you make sure a procedure is done safely and with an optimal outcome. We know that IVUS can have the same influence in our lower extremity procedures, but we need to get people using it. We have fewer standardized approaches to lower extremity revascularization care than in most other procedures. It is time now to use these data, use the expert consensus document as a framework, understand how to adopt IVUS technology into your practice, understand how it can be best used to treat your patients, and understand how to incorporate this information to make the best determinations on how to optimize the procedure. We hope this is the tipping point.
One objection to the use of IVUS was a lack of randomized, controlled trial data. How do these data affect that discussion?
That is always a question. How do we generate the right evidence to prove this therapy is effective and then also allow for it to be generalizable to our practices? We have been frustrated on the coronary side because there have been meaningful IVUS-guided randomized trials that should have made a greater impact on operator practice. We always have to weigh how valuable those investments are and how meaningful the data can be in a randomized trial to employ them into our clinical practice. That being said, we need data in peripheral IVUS and March of 2022 marked the first publication of a prospective, randomized trial on the arterial side, a study that was done out of Australia by Allan and colleagues.2 They looked at 150 patients who were treated for femoropopliteal artery revascularization and were randomized to an IVUS-guided strategy versus a routine angiography-guided strategy. At one year, there was nearly a 17% reduction in binary restenosis when IVUS was incorporated as part of the revascularization procedure. For people who were randomized to IVUS, that information changed strategies in up to 78% of all treatment plans. When IVUS imaging was incorporated, operators responded with, “Wow, I’m going to use a larger balloon,” or “I’m going to cover a little bit longer because I didn’t see that disease on the angiogram,” or “I’m going to do plaque modification.” IVUS use changed practice in this trial and those practice-changing moves resulted in a reduction in binary stenosis at one year. I like to use randomized trial data along with our real-world data that look at harder endpoints like major adverse limb events. A randomized trial showing reduction in restenosis can now also translate in the real world to fewer limb-related events over time. More prospective data are already available on the venous side, including the VIDIO study3, which really showed us how IVUS changed practice for venous intervention. Prospective data like these were not available on the arterial side until the randomized trial by Allan and colleagues was performed.
If someone is interested in learning more about using IVUS, where do you recommend they start?
We are hoping that the consensus document and some of the published literature coming out will provide a framework. We have recently published a manual on peripheral intravascular imaging4 with images to reference some of the data, really a nice summary of all the information I discussed. On top of that, we are involved in workshops and symposiums at all the major conferences that will provide opportunities to ask questions and further learn about imaging interpretation. Obviously, company representatives for intravascular imaging devices are well prepared to walk through some of the basic elements such as how to measure the reference vessel and how to interpet the image. There are layers of information and industry partners are working through their own team of educators.
What are the next steps? Are more data coming?
The goal thus far has been to present information, listen to what people have to say, and understand what we need to do to address any of the obstacles or perceived barriers that exist. We have taken that to heart and are trying to address perceived barriers to IVUS use. One of the first things that we are working on is a better clarification of the costs associated with IVUS and helping people understand that the device, at least in the United States, is fairly reimbursed. Outcomes with the use of IVUS can drive financial benefits for our healthcare system and then obviously for our patients. Fewer hospitalizations and lower target vessel revascularization rates have meaningful cost implications, and we are going to spend some time looking at costs.
The other perceived barrier is time. Putting an IVUS catheter down a vessel involves setup time and time to interpret the image. IVUS has been utilized in the coronary space without increasing procedural time. Many of us already using IVUS in the arterial and venous space do so without a big impact on our procedural time. In my own experience, the use of IVUS reduces time, because I am already sizing my vessels and determining how I am approaching my procedure as I am acquiring the intravascular images.
Finally, we are always talking about evidence generation, whether through prospective studies, randomized trials, or more real-world studies. How do we continue to supplement what we know? How do we create some algorithms for areas that are not as clear? We will be spending a lot of time on this as well.
†Secemsky EA, Mosarla RC, Rosenfield K, et al. Appropriate use of intravascular ultrasound during arterial and venous lower extremity interventions. JACC Cardiovasc Interv. 2022 Aug 8;15(15):1558-1568. doi: 10.1016/j.jcin.2022.04.034
This article is supported by Philips.
D061857-00
*Venous use may be available in select markets.
References
1. Natesan S, Mosarla RC, Parikh SA, Rosenfield K, Suomi J, Chalyan D, Jaff M, Secemsky EA. Intravascular ultrasound in peripheral venous and arterial interventions: a contemporary systematic review and grading of the quality of evidence. Vasc Med. 2022:1358863X221092817. doi: 10.1177/1358863X221092817
2. Allan RB, Puckridge PJ, Spark JI, Delaney CL. The impact of intravascular ultrasound on femoropopliteal artery endovascular interventions: a randomized controlled trial. JACC Cardiovasc Interv. 2022; 15(5): 536-546. doi: 10.1016/j.jcin.2022.01.001
3. Gagne PJ, Tahara RW, Fastabend CP, et al. Venography versus intravascular ultrasound for diagnosing and treating iliofemoral vein obstruction. J Vasc Surg Venous Lymphat Disord. 2017;5(5):678-687. doi: 10.1016/j.jvsv.2017.04.007
4. Secemsky EA, Parikh SA, Kohi M, et al. Intravascular ultrasound guidance for lower extremity arterial and venous interventions. EuroIntervention. 2022: EIJ-D-21-00898. doi: 10.4244/EIJ-D-21-00898
Related Media
