


Coronary Interventions in the ASC: Now What? Does Your Health System Have an Ambulatory Strategy?
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Marc Toth, Vice President of Cardiovascular Services, Atlas Healthcare Partners
Derek Mitzel, DO, MBA, Phoenix, Arizona
Copyright Atlas Healthcare Partners 2020.
The authors can be contacted via Marc Toth at marc.toth@atlashp.com
By the time you read this article, hundreds, if not thousands, of Medicare patients will have had percutaneous coronary interventions (PCIs) in Medicare-accredited ambulatory surgery centers (ASCs) around the country. The Centers for Medicare and Medicaid Services (CMS)’ approval of PCI in the ASC setting is a watershed moment and will accelerate the outmigration of cardiovascular care from the hospital to ASCs. The addition of these codes by CMS may be part of a larger goal aimed at empowering patients through greater choice and helping them avoid unnecessary costs by offering alternatives to the hospital for cardiovascular care. In 2019, CMS allowed diagnostic angiograms; the 2020 inclusion of angioplasty and stenting signals their support of this service outside of the hospital. CMS data is clear on the advantages of outpatient care, both for the patient and for them as the payer. For calendar year 2020, CMS also added total knee replacement, which also indicates that CMS considers ASCs an important alternative site of service to the hospital in helping to reduce costs while improving patient satisfaction.
Why Should Health Systems Embrace the Cardiovascular Outmigration to ASCs?

First and foremost, it is all about the patient. It is no secret that an ASC provides a better overall patient experience. Getting a procedure done in a comfortable and convenient setting is appealing to patients, but saving money with a lower co-insurance rate is even better. The nimble nature of the ASC creates an environment better suited to engage patients on a one-on-one basis and provide a more patient-focused experience. Advancements like transradial access and same-day discharge for PCI have made interventional procedures safe and appropriate in the ASC setting. Implanting cardiac devices such as pacemakers, defibrillators, and loop recorders in the ASC setting is being rapidly adopted and has proven to be a safe, cost-effective site of service since these procedures were added to the ASC list several years ago.
The ASC site of service wholeheartedly upholds the triple aim of healthcare: improving the patient experience, reducing the cost of health care, and improving population health. For the health system patients covered under their health insurance plan, the ASC provides a lower-cost site of service. Moving routine, lower-risk cardiovascular procedures out of the hospital can free up valuable cath and electrophysiology (EP) lab time for complex PCI, EP procedures, and high margin structural heart procedures. ASCs also have a lower rate of post procedure infections and higher physician satisfaction related to a more convenient scheduling and flexibility in staff, equipment, and supplies.
The Society for Cardiovascular Angiography and Interventions (SCAI) and American College of Cardiology (ACC) Support PCI in the ASC
Both the American College of Cardiology (ACC) and the Society for Cardiovascular Angiography and Interventions (SCAI) provided letters of support for the changes during the public comment period following CMS’ release of the proposed addition of PCI in August. In their August 27, 2019 letter to Seema Verma, SCAI stated: “SCAI supports CMS’s proposed addition of percutaneous coronary angioplasty and coronary stenting to the list of ASC Covered Surgical Procedures for CY2020.”1
CMS recently stated: “After reviewing the clinical characteristics of these procedures and consulting with stakeholders and our clinical advisors, we determined that these…procedures would not be expected to pose a significant risk to beneficiary safety when performed in an ASC and would not be expected to require active medical monitoring and care of the beneficiary at midnight following the procedure.”2
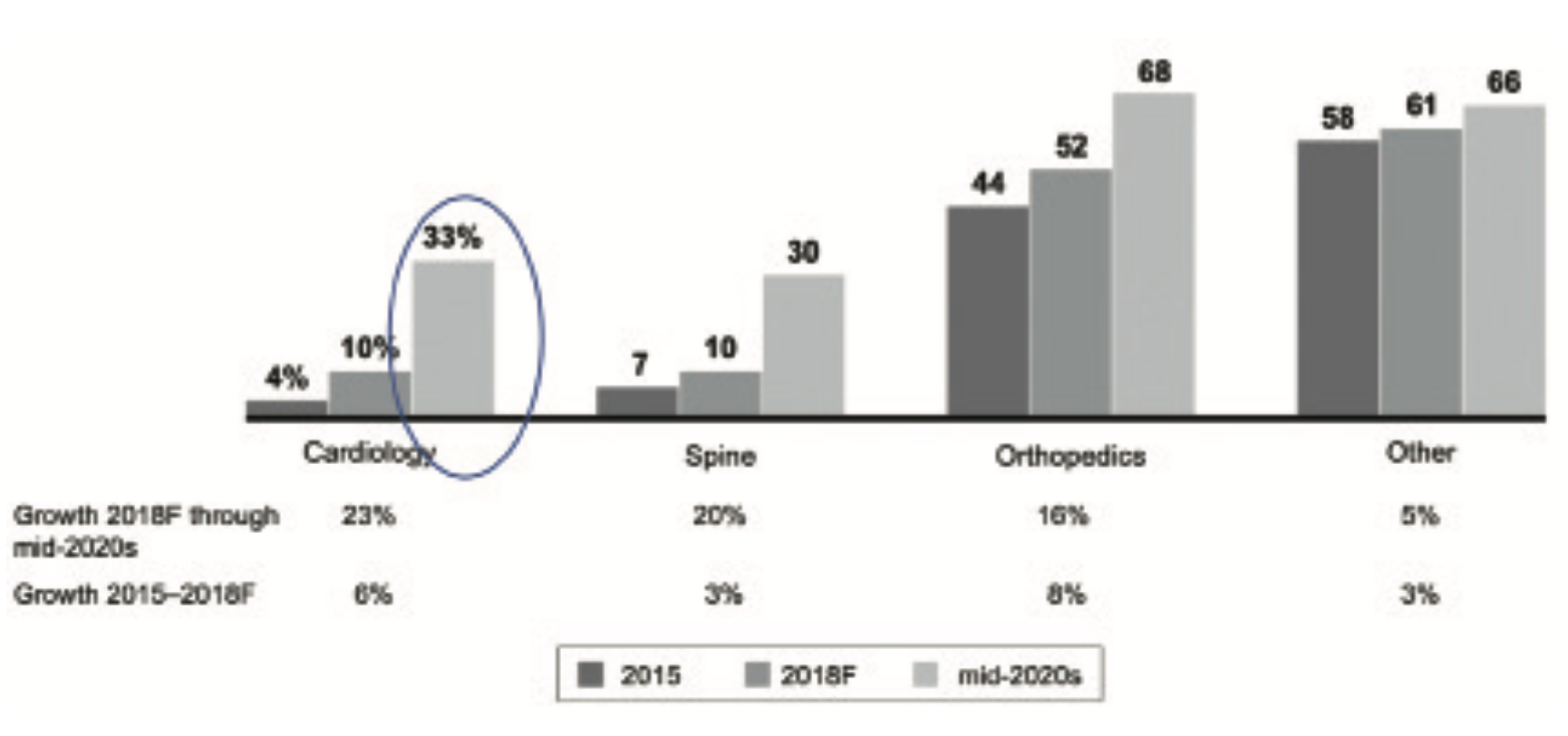
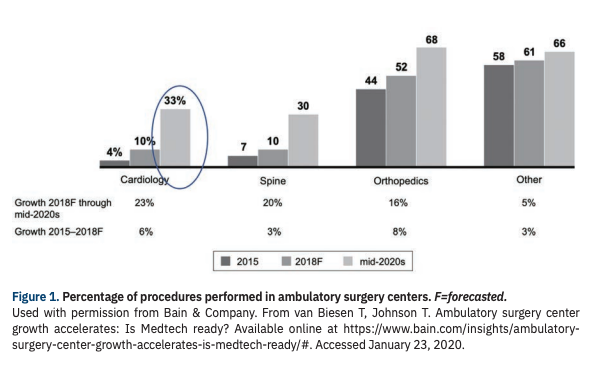
Used with permission from Bain & Company. From van Biesen T, Johnson T. Ambulatory surgery center growth accelerates: Is Medtech ready? Available online at https://www.bain.com/insights/ambulatory- surgery-center-growth-accelerates-is-medtech-ready/#. Accessed January 23, 2020.
Projections of the out migration of cardiovascular procedures vary, but Bain and Company projected that by the mid 2020s, 33% of cardiovascular cases will be performed in ASCs (Figure 1). This projection was published before CMS added PCI to its covered list for ASCs in 2020 — many believe the projected cardiovascular migration will rapidly approach 50%.
Economics
By focusing on routine, lower-risk procedures in a more comfortable and convenient setting, cardiovascular ASCs can offer the same cardiovascular procedures at a rate 35-50% lower than hospitals. Private payers have led the way in paying for PCI in the ASC setting. Shouldn’t Medicare patients receive the same opportunities to receive care in a lower cost, more comfortable setting? Medical bills are reported to be the number-one cause of U.S. bankruptcies. One study has claimed that 62% of bankruptcies were caused by medical issues.3 Another study claims that over 2 million people are adversely affected by their medical expenses.4
In its final rule, CMS estimated that moving 5% of coronary interventions from the hospital outpatient setting to ASCs would reduce Medicare payments by about $20 million and total beneficiary copays by about $5 million in calendar year 2020. In addition to economic concerns, patient engagement and satisfaction are vital pieces of the care equation, and the ASC setting typically improves measures in all categories.
The ACC has raised questions, however, about whether it would be “economically feasible” to perform these procedures in ASCs, stating that “CMS should consider whether updates to the ASC payment methodology are needed in order to provide sufficient and sustainable payment.”2
As always with new procedures, the reimbursement can and will vary from year to year. As CMS adds more PCI codes to ASCs, current ASC reimbursement rates may increase, closing the gap between the ASC and hospital outpatient department (HOPD) rates. Site neutrality is most likely coming, and it will be interesting to see how it will be implemented. Will ASC rates go up and/or will HOPD rates be reduced?
Concerns – Appropriate Use Criteria
The ACC supported the addition of the coronary interventions to the list of covered procedures but noted that “Some amount of caution is necessary to ensure appropriate infrastructure and protocols are in place. Specific guidance for PCI performed without surgical backup exists and should serve as a framework for PCI in the ASC setting.”2
SCAI went a step further, stating “It is imperative that patients undergoing PCI in the ASC setting receive the same quality of care afforded to cardiovascular patients receiving PCI in the hospital outpatient setting. We urge CMS to support the establishment of minimum facility standards that will assure quality of care in the ASC setting including a mandate for participation in a quality registry that will track outcomes for PCI procedures performed in the ASC site of service.”1
The inclusion of these interventions in ASCs comes despite the fact they may involve major blood vessels, which has been considered an exclusion for CMS coverage at ASCs in some states. Many states are currently reviewing such archaic language in their department of health regulations. Georgia is reviewing EP implants in ASCs, Mississippi is reviewing their certificate of need (CON) status for single-specialty ASCs, Pennsylvania is reviewing peripheral arterial disease (PAD) in the ASC, and there are lobbying efforts underway in California and Michigan to change regulations related to cardiovascular procedures in ASCs.
CMS weighed in on the ‘major blood vessels’ issue, noting: “Although the proposed coronary intervention procedures may involve blood vessels that could be considered major, …we believe the involvement of major blood vessels is best considered in the context of the clinical characteristics of individual procedures, and we do not believe that it is logically or clinically consistent to exclude certain cardiac procedures from the list of ASC-covered surgical procedures on the basis of the involvement of major blood vessels, yet continue to provide ASC payment for similar procedures involving major blood vessels that have a history of safe performance in ASCs.”2
In support of their decision, despite some state regulations exclusion of procedures involving major blood vessels, CMS cites CPT codes for “mechanicochemical destruction of insufficient vein of arm or leg, accessed through the skin using imaging guidance” and “insertion of stents into groin artery, endovascular, accessed through the skin or open procedure.”
Models for Health Systems
Many health systems have a robust ASC strategy and already have joint ventures in multi-specialty ASCs. This strategy should support the development of cardiovascular ASCs, since it can help hospitals free up crowded cath lab schedules for the higher acuity, higher margin cases. Cardiovascular physicians who are employed by or are aligned with health systems that have existing multispecialty ASCs are likely to have an easier time establishing a joint-venture cardiovascular ASC. If the health system has their own insurance product, it’s a win-win for all parties: the patient, payer, and provider.
A joint-venture model for cardiovascular ASCs offered by a large health system in the southwest is gaining traction. It allows employed, independent, and aligned physicians to participate in ownership of the cardiovascular ASC joint venture with the health system. The health system provides the space for the ASC — frequently on the hospital campus in a medical office building — and can often provide access to managed care contracts and contracts with vendors that the physicians can’t negotiate on their own. The health system can offer their network of primary care physicians and participation in their health insurance plans as well. The physicians have the ability to offer a lower coinsurance payment to their patients and perform the procedures in a more convenient comfortable stetting. As owners, physicians also will be able to participate in distributions.
Conclusion
CMS has taken a proactive approach to providing cardiovascular care in the ambulatory surgery center setting by adding PCI to the already approved implantable devices. It is now time for health systems to solidify their ASC cardiovascular strategy and develop dedicated ASCs for their cardiovascular care or to expand their existing ASCs into other innovative outpatient ventures. We all win in this new paradigm: the patient, the payer, and the provider.
References
- Society for Cardiovascular Angiography and Interventions (SCAI) Letter to Seema Verma. RE: “Medicare Program: Proposed Changes to Hospital Outpatient Prospective Payment and Ambulatory Surgical Center Payment Systems and Quality Reporting Programs; Price Transparency of Hospital Standard Charges; etc. [CMS-1717-P]”. August 27, 2019. Available as pdf download at https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=2ahUKEwjhga_SypLnAhVKXKwKHctqB-4QFjAAegQIARAB&url=http%3A%2F%2Fwww.scai.org%2FAssets%2F83842d7c-201b-4c2c-b557-ad4a8be7bf76%2F637051828896330000%2Fsr-scai-2020-hopps-comment-letter-final-edit-ag-pdf&usg=AOvVaw0DT_A6Q-iz9ZItWbibiFtx. Accessed January 20, 2020.
- Neale T. CMS finalizes rule allowing reimbursement of PCI in ambulatory centers. TCTMD. November 4, 2019. Available online at https://www.tctmd.com/news/cms-finalizes-rule-allowing-reimbursement-pci-ambulatory-centers. Accessed January 20, 2020.
- Himmelstein DU, Thorne D, Warren E, et al. Medical bankruptcy in the United States, 2007: results of a national study. Am J Med. 2009 Aug;122(8):741-746.
- Hamel L, Muñana C, Brodie M. Kaiser Family Foundation/LA Times Survey Of Adults With Employer-Sponsored Insurance. May 2, 2019. Available online at https://www.kff.org/private-insurance/report/kaiser-family-foundation-la-times-survey-of-adults-with-employer-sponsored-insurance/. Accessed January 20, 2020.
Find More:
Cardiovascular Ambulatory Surgery Centers (ASCs) Topic Center

