


Feasibility of Coronary Re-Access and Repeat TAVR After Sapien 3 TAVR Stratified By Implant Depth: A CT Simulation Study
This study looked at the implant depth of the Sapien 3 (Edwards Lifesciences) and used CT simulation to evaluate feasibility for coronary re-access and a second TAVR. Can you tell us more about it?
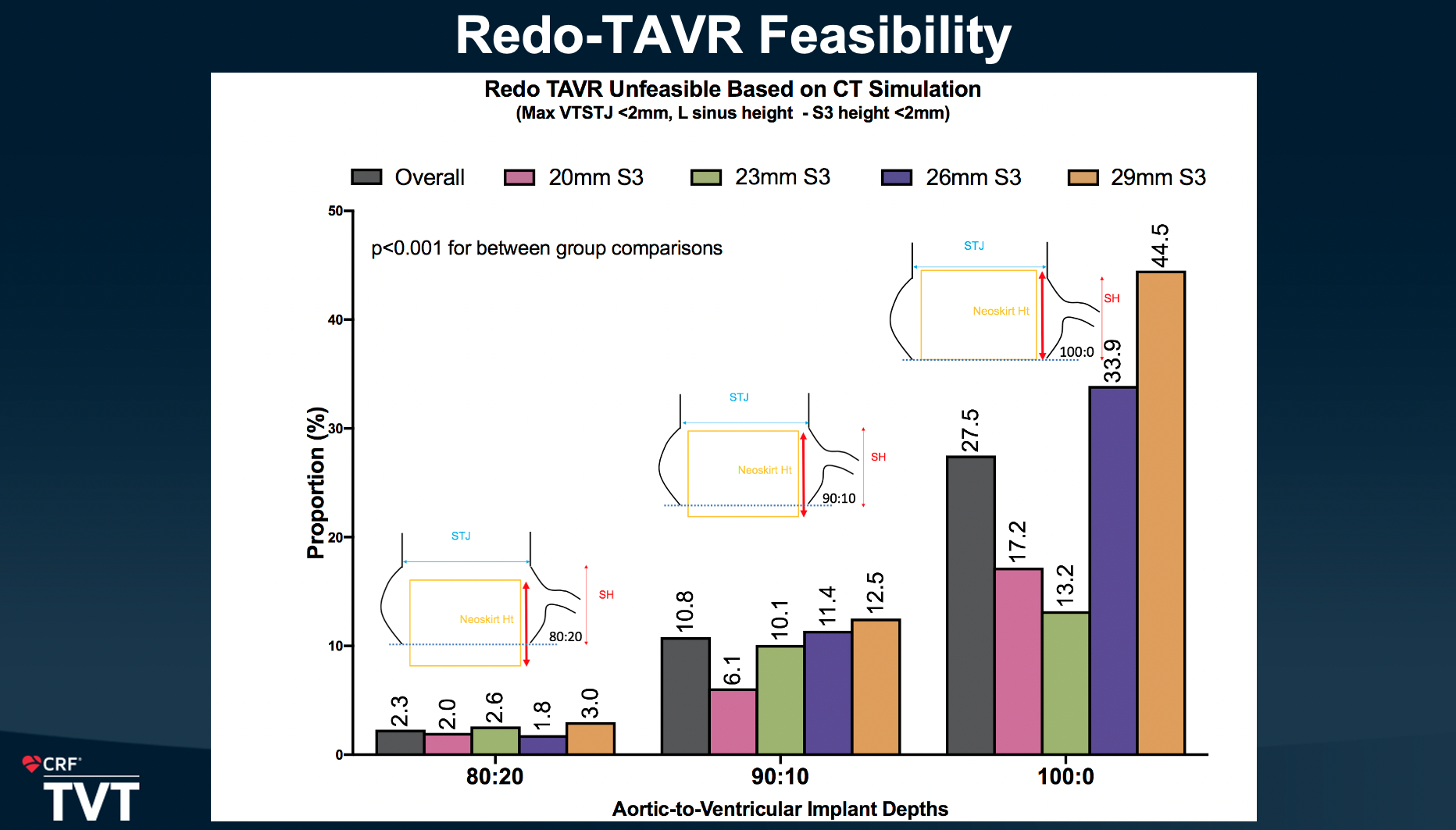
 Gilbert Tang, MD: We had almost 2000 CT scans that had been collected over the last 5 years. Looking retrospectively, we wanted to find out if we were to do a redo TAVR on these patients with the Sapien 3 transcatheter heart valve (THV) only, based on the target implant depth, what percentage of the patients would not be feasible to do TAVR-in-TAVR afterwards when the Sapien 3 valve fails? We looked at the aortic root anatomy, and placed a virtual valve at the 80:20, 90:10, or 100:0 position (aortic‐to‐ventricular implant depth) right through the annulus, and then determined whether there was room to clear for a second valve without obstructing the coronary artery. We had to establish definitions on the feasibility basically by predefining the ability to advance a 6 French catheter through the opening to be able to perfuse the coronary. We found that the root anatomy changes as you implant higher, because now, rather than below the sinotubular junction, if you implant, let's say a 100:0, the Sapien 3 valve would end up being above the sinotubular junction. So, you have to measure what we call valve to sinotubular junction distance to determine if there will be sufficient flow to avoid coronary obstruction and sinus sequestration. So, essentially what we found was that as you go higher on the implant, the feasibility of the TAVR-in-TAVR with a Sapien 3 being the first valve goes down. It may be the first time that anyone has studied this with the implant depth. There have been previous studies looking at TAVR-in-TAVR with prior Sapien 3 using CT modeling and others, but they did not look at the impact of implant depth.
Gilbert Tang, MD: We had almost 2000 CT scans that had been collected over the last 5 years. Looking retrospectively, we wanted to find out if we were to do a redo TAVR on these patients with the Sapien 3 transcatheter heart valve (THV) only, based on the target implant depth, what percentage of the patients would not be feasible to do TAVR-in-TAVR afterwards when the Sapien 3 valve fails? We looked at the aortic root anatomy, and placed a virtual valve at the 80:20, 90:10, or 100:0 position (aortic‐to‐ventricular implant depth) right through the annulus, and then determined whether there was room to clear for a second valve without obstructing the coronary artery. We had to establish definitions on the feasibility basically by predefining the ability to advance a 6 French catheter through the opening to be able to perfuse the coronary. We found that the root anatomy changes as you implant higher, because now, rather than below the sinotubular junction, if you implant, let's say a 100:0, the Sapien 3 valve would end up being above the sinotubular junction. So, you have to measure what we call valve to sinotubular junction distance to determine if there will be sufficient flow to avoid coronary obstruction and sinus sequestration. So, essentially what we found was that as you go higher on the implant, the feasibility of the TAVR-in-TAVR with a Sapien 3 being the first valve goes down. It may be the first time that anyone has studied this with the implant depth. There have been previous studies looking at TAVR-in-TAVR with prior Sapien 3 using CT modeling and others, but they did not look at the impact of implant depth.
The other finding we had was in regard to coronary access after TAVR-in-TAVR. If you have a Sapien 3 already in place at a certain implant depth and place a second valve afterwards, usually a taller frame valve, we looked at how difficult it might be theoretically to do coronary access. The difficulty is defined as follows. If the top of the neoskirt height from the Sapien 3 is at or below the coronary takeoff, the coronary height, then it should be easy after you put a second valve in, especially a taller frame valve, because you have the opening to go through directly. However, if the top of the valve, the neoskirt height of the Sapien 3, is above the coronary, then the second valve will create a barrier on top of the Sapien 3, being now completely like a cylindrical barrier to access the coronary. We found that if you implant higher, the percentage of difficult coronary access would be higher as well, but more so for the left main than the right coronary, because the right coronary sits higher. So, fewer patients will be found difficult.
Our conclusion is that implanting high is not a good idea for everybody, especially thinking about lifetime management and TAVR-in-TAVR, even with the Sapien 3. We need to look at the CT scan, look at the patient, and determine ahead of time what target implant type to aim for to potentially get the best of all worlds, which means avoiding a pacemaker and avoiding left bundle branch block, but at the same time being able to facilitate anatomically TAVR-in-TAVR in the future.
Why is lifetime management and TAVR-in-TAVR a hot topic?
Gilbert Tang, MD: We are seeing more patients coming back with TAVR failure needing potentially TAVR-in-TAVR or TAVR explant surgery. We have already seen more of these patients last year and this year. It is not that the valves are not durable and failing early. It's just that TAVR, at least in the United States, has been around now for more than 10 years, since the first commercialization. Patients with TAVR valves, just like surgical valves, are not going to last forever. We are now seeing patients coming back with TAVRs that were performed at least within 5 or more years ago, coming back with failure. We need to find a solution to that, but also, at the same time, we are treating younger patients or lower risk patients who we expect will have a longer life expectancy. A 65-year-old will have a life expectancy of, well, probably 20 years, a 70-year-old would be at least 15 years. We need to do the first valve right so that we can preserve options for these patients such that in the future they would not need surgery to remove the first valve.
The first step in doing so is to look at the patient's CT anatomy. For example, if the anatomy is very generous for the Sapien 3 valve, then of course you can implant 100:0 or as high as possible to avoid pacemaker risk for conduction system issue. However, if the patient will likely not be able to get a TAVR-in-TAVR in the future because of the sinus sequestration and coronary obstruction, then maybe an intentional, slightly deeper implant, I don't mean by 60:40 or 70:30, but maybe an 80:20 ratio. Based on our analysis, at 80:20, the ability to redo TAVR with Sapien 3 is almost over 95%. It could be a better option in some of these patients in terms of pursuing lifetime management.
Find more: TVT Newsroom (With a Special Focus on TAVR)
Find Dr. Tang’s presentation slides here.
Read a previous CLD interview with Dr. Tang:
Transcatheter Aortic Valve Positioning: A Simple Technique to Ensure Future Coronary Access
