


Nurses’ Compliance and Confidence With a Hand-Off Process for Patients Post Femoral Arterial Access Before and After a Standardized Approach
This study encompassed the Intensive Care Unit (ICU), Step Down Unit (SDU), and Progressive Care Units (PCU), along with the Heart Center staff, at Excela Health Westmoreland Hospital in Greensburg, Pennsylvania, which includes three community hospitals with 578 licensed beds. There are approximately 50 patients monthly who receive femoral arterial access for procedures in the Heart Center and who are then transferred to an inpatient critical care unit.
Abstract
Background: Accurate communication during the nurse hand-off process in patients receiving femoral artery access for procedures is crucial to prevent negative outcomes.
Following a sentinel event, a workgroup developed and tested a nurse handoff process with a standardized report form and two-party verification of the access site.
Objective: To measure changes in nurses’ self-reported compliance and confidence, observed compliance, and number of communication-related negative patient outcomes before and after the implementation of a standardized report form and two-party verification of the arterial access site during nurse hand-off.
Methods: RNs and technicians employed in a heart center and intensive care units completed a compliance and confidence survey at baseline, after an education session, and after the implementation of the revised hand-off process. Dyads were observed during nurse hand-off before and after the implementation of the revised hand-off process. An audit form measured negative patient outcomes.
Results: Seventy-eight nurses and technicians completed the pre (n=35) and post (n=43) surveys. A statistically significant difference in the survey mean scores and the mean ranks of two items were found before and after the implementation of the existing and standardized hand-off process. Eighteen dyad observations with the existing (n=9) and standardized process (n=9) found improvements in 11/16 (68.7%) hand-off components. Audit data of 461 eligible patients revealed a decrease in the number of negative outcomes from 12 at baseline to 0 at study completion.
Conclusion: Nurses’ self-reported and observed compliance with a standardized report form and two-party site verification during nurse hand-off improved.
Accurate and timely communication among caregivers during the nurse hand-off process is crucial for safe patient care and prevention of negative outcomes. The Joint Commission1 defines a hand-off as the transfer and acceptance of patient care responsibility through effective communication, occuring in real time, for the purpose of promoting patient safety and continuity of care. During the hand-off process, important patient-related data are communicated among nurses and staff. The reliability of this exchange hinges on a communication process that reduces data omissions and promotes data veracity.
The nurse hand-off process has been a topic of rigorous study for many years. Galatzan and Carrington’s systematic review2 of the research on the nurse hand-off process published between 2007 and 2017 identified six themes: standardized hand-off tools; nurses’ satisfaction with and perceptions of the hand-off; communication and communication patterns; electronic tool usage; nurses’ memory or cognition; and hand-off content. Using a Delphi approach, O’Rourke et al3 identified the core components of the nurse hand-off process as patient summary, action plan and nurse-nurse synthesis.
Standardized hand-off tools, such as checklists, and processes are the focus of published research studies and quality improvement projects. The effectiveness of a standardized nurse hand-off tool and process on communication efficiency and accuracy in the emergency department4 and operating room5, and in oncology care6 and acute care7, are recent examples showing that standardization of the nurse hand-off tool and process promotes effective communication during patient transfers in a variety of settings.
A lack of standardization in the nurse hand-off process may result in communication breakdowns that can lead to negative patient outcomes. The Joint Commission8 estimates that 80% of serious medical errors involve miscommunication among staff during patient transfers. In our heart center, we conducted a three-month medical record audit of patients requiring femoral arterial access for procedures who were transferred to inpatient critical care units. Of the 150 patient records audited, negative outcomes following the procedure occurred in 4% (6/150) patients, all of which may have been associated with communication breakdowns during the nurse hand-off process.
Patients treated in our heart center undergo a variety of procedures that require arterial access, such as stenting peripherial, coronary, and carotid arteries, and implantation of Watchman devices (Boston Scientific). All patients requiring arterial access for procedures or cardiac-related care can benefit from a standardized nurse hand-off checklist and process. Kaufman et al9 implemented a standardized handoff protocol for transfering patients from the pediatric cardiothoracic operating room to the cardiac intensive care unit, with a focus on unplanned extubations. Post hand-off standardization, there was a significant decrease in unplanned extubations. Similarly, Dixon et al10 evaluated a formalized hand-off process for patients undergoing cardiac surgery with transfer to the intensive care unit. Their findings demonstrated that a standardized checklist during nurse hand-off improves communication of vital information during patient transfer. McGrath11 implemented a standardized nurse hand-off process between certified registered nurse anesthetists (CRNAs) and registered nurses (RNs) in the cardiovascular intensive care unit. Results of this improvement project demonstrated a decrease in the omission of important patient information and a positive impact on patient safety.
Based on the published evidence, a standardized process and checklist for nurse hand-off assures that relevant information is passed along appropriately and consistently, thus reducing the opportunity for omitting salient data and decreasing the chance for negative patient outcomes. Prior to 2020, our heart center did not have a standardized nurse hand-off process. Following a sentinel event, the heart center began routine auditing of its patient medical records for negative patient outcomes. During staff education sessions, nurses in the critical care units disclosed they were not receiving a consistent, complete report on patients received from the heart center and did not feel confident caring for these patients without all of the relevant data required for a successful nurse hand-off. Furthermore, there was no formal notation of the arterial access site assessment during the hand-off process.
The root cause analysis of this significant vascular complication after a cardiac catheterization prompted the formation of a workgroup dedicated to the early identification and prevention of bleeding complications. We recognized the need for a standardized process to share information about patients transferred from our heart center to inpatient critical care units based on nurses’ concerns and our root cause analysis. The workgroup explored the revision of the nurse hand-off process for patients who undergo femoral access for a procedure and are admitted to an inpatient critical care unit. This collaborative workgroup was comprised of clinical nurses, information technology staff, coordinators and educators from the intensive care unit (ICU), step down unit (SDU), and progressive care units (PCUs), and heart center recovery room and in-procedure staff. The workgroup utilized the framework of implementation research12 to evaluate the existing nurse hand-off process and review the literature on components of a standardized checklist and nurse hand-off process. The outcome was a revised nurse hand-off process that included a standardized report form and a two-party verification of the arterial access site. Anticipated implementation research outcomes based on Peters et al12 included hand-off acceptability and adoption, the appropriateness of the hand-off process, hand-off feasibility for other patient care areas, and the cost of the standardized forms and sustainability after study completion. Anticipated care outcomes of instituting the revised hand-off process were compliance with the standardized nurse hand-off process, an increase in nurses’ confidence in caring for patients post-arterial access, and a decreased number of negative patient outcomes.
Our institutional review board-approved, quasi-experimental, pre-post intervention study compared nurses’ compliance with the existing and revised nurse hand-off process with a standardized report form and two-party verification of the arterial access site. The primary study outcome was compliance with the revised, standardized nurse hand-off process. The secondary outcomes were nurses’ confidence in caring for patients whose procedures required femoral access and reduction of negative patient outcomes that may be associated with communication breakdown during the nurse hand-off process. The research question was: Before and after the implementation of a standardized report form and two-party verification of the access site, are there changes in: nurses’ self-reported compliance with the hand-off process; nurses’ self-reported confidence in the hand-off process; observed compliance with the hand-off process; and the number of negative patient outcomes?
Methods
Setting and Participants. The study setting was the heart center of our health system, which includes three community hospitals with 578 licensed beds. There are approximately 50 patients monthly who receive femoral arterial access for procedures in the heart center and who then are transferred to an inpatient critical care unit. Included in the study were registered nurses (RNs) and advanced life support technicians (ALS techs) employed in the heart center, ICU, SDU, and PCU, and responsible for patients who required femoral arterial access for a procedure. Patient medical records included for audit were those patients who received femoral arterial access for a procedure in the heart center and then transferred to the ICU, SDU, or PCU. Patients requiring femoral arterial access were selected because the femoral approach requires the insertion of larger diameter catheters and additional arterial manipulation, resulting in the highest risk for major adverse cardiac events (MACE).13,14 MACE events include death, myocardial infarction, stroke, and emergent coronary bypass surgery.14
Data Collection Instruments. Data were collected using two investigator-developed surveys and one institution-approved audit form.
Self-Reported Compliance and Confidence With the Nurse Hand-off Process for Patients Post-Arterial Access Survey. The dual purpose of this 6-item Likert-type survey was to measure staff compliance with the nurse hand-off process for patients receiving femoral arterial access, as well as staff confidence in caring for these patients, based on the information received post hand-off. Five items measured self-reported compliance with the elements of the nurse hand-off process. One item measured self-reported confidence in caring for patients based on the information received during the nurse hand-off process. Two demographic items were the unit of employment (heart center, ICU, SDU, PCU) and staff role (RN or ALS Tech). Items were scored 1 (never) to 5 (always); scores ranged from 6 to 30. Content, construct. and face validity were established by having the survey evaluated by two master’s-prepared nurses and members of the workgroup.
Observed Compliance Checklist. This 16-item checklist was utilized by the principal investigator and co-investigator to evaluate the nurses’ compliance with the components of the nurse hand-off process. Item scores were 0 (not observed) and 1 (observed), with a range of 0 to 18. This checklist was derived from the report form’s patient data communicated during the hand-off process. Content, construct, and face validity were established by having the checklist evaluated by two master’s-prepared nurses and the workgroup. Reliability was established by third-party verification of observed nurse hand-offs with a co-investigator or with the RN receiving or giving report.
Arterial Access Audit Form. The Arterial Access Audit Form is a health system-sanctioned tool that tracks the documentation of patient care following a procedure requiring arterial access. Only the audit information of patients receiving femoral access were included; the audit elements evaluated for this study were date of procedure, critical care admitting unit. and negative outcome (yes/no).
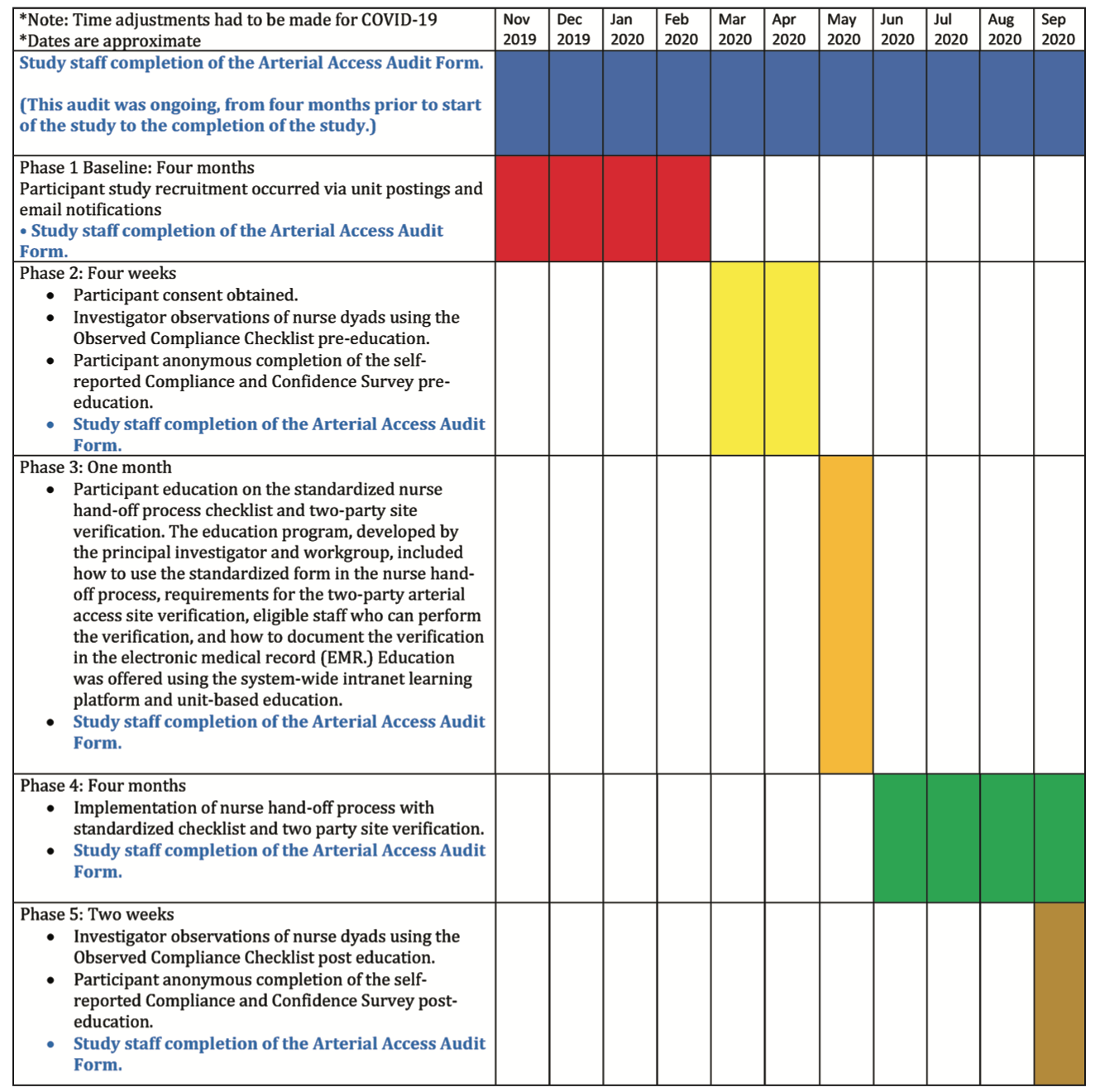
Data Collection Procedure. Figure 1 outlines the data collection procedure.
Sample Size. There were 197 registered nurses and five ALS techs eligible for the study (15 in the heart center, 108 in the PCU, 53 in the ICU, and 26 in the SDU). We assumed a 30% pre and post survey response (60 staff) and a 30% (30 dyads or 60 staff) pre and post observation rate. We anticipated 50 medical records per month (10-month study period, 500 records) of patients receiving femoral arterial access for a procedure who were then transferred to an inpatient critical care unit.
Statistical Analyses. Data were analyzed using parametric and nonparametric statistical tests using the Statistical Package for Social Sciences Version 24 (SPSS v. 24.). The level of significance was set at P≤.05.
Results
Eighty-three staff, of which 80 [96.4%) were RNs and 3 [3.6%) were ALS technicians, participated in the study.
The Self-Reported Compliance and Confidence Survey was administered pre and post education. Survey total scores were calculated on those respondents with complete data. Thirty-five staff completed the survey pre education, with a mean score of 23.05 (standard deviation [SD] = 4.56, range = 12-30); 43 staff completed the survey post-education (mean = 25.02, SD = 3.32, range = 18-30). There was a statistically significant difference between the pre- and post-education mean scores (t= -2.129, P=.037). The Survey total mean rank score was 34.39 pre education and 43.66 post education. Using the Mann-Whitney U test, there was no statistically significant difference between the pre- and post-education mean ranks, despite the increased mean rank post education.
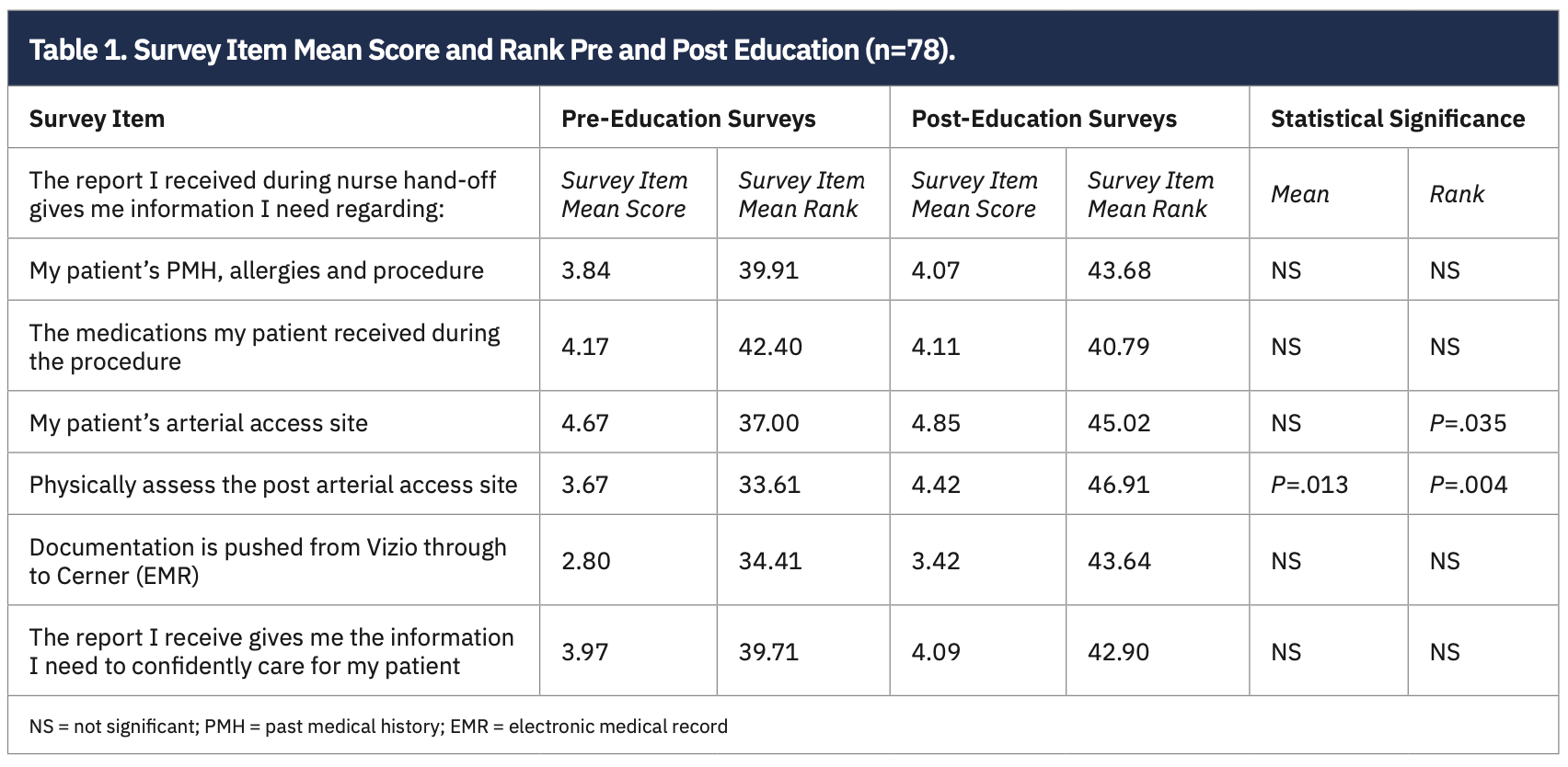
The t-test for independent groups and the Mann-Whitney U test were performed to determine differences in the means and ranks of the item scores, respectively. Two items reached statistical significance for their mean scores and ranks:
• “The report I received during nurse hand-off gives me information I need regarding my patient’s arterial access site”;
• “The report I received during nurse hand-off gives me information I need (to) physically assess the post arterial access site.”
Both items’ mean scores and ranks improved after the education (Table 1). Nurses’ confidence in caring for patients post arterial access based on the nurse hand-off report remained unchanged.
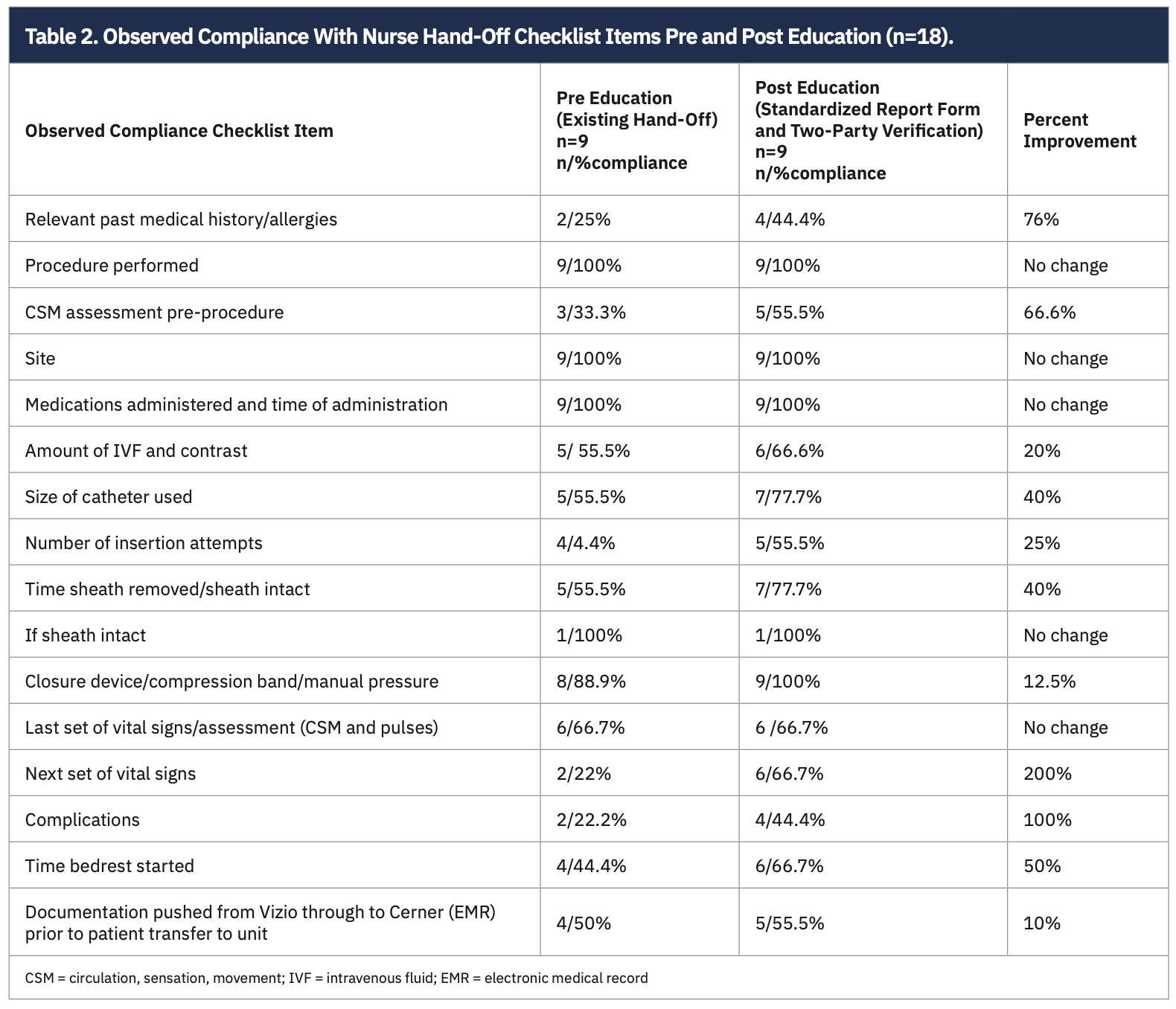
The Observed Compliance Checklist was completed on 9 nurse dyads pre education and 9 nurse dyads post education. Table 2 compares the pre and post education (standardized report and two-party site verification) findings. Improvements were found in 11 out of the 16 (68.7%) of the checklist items.
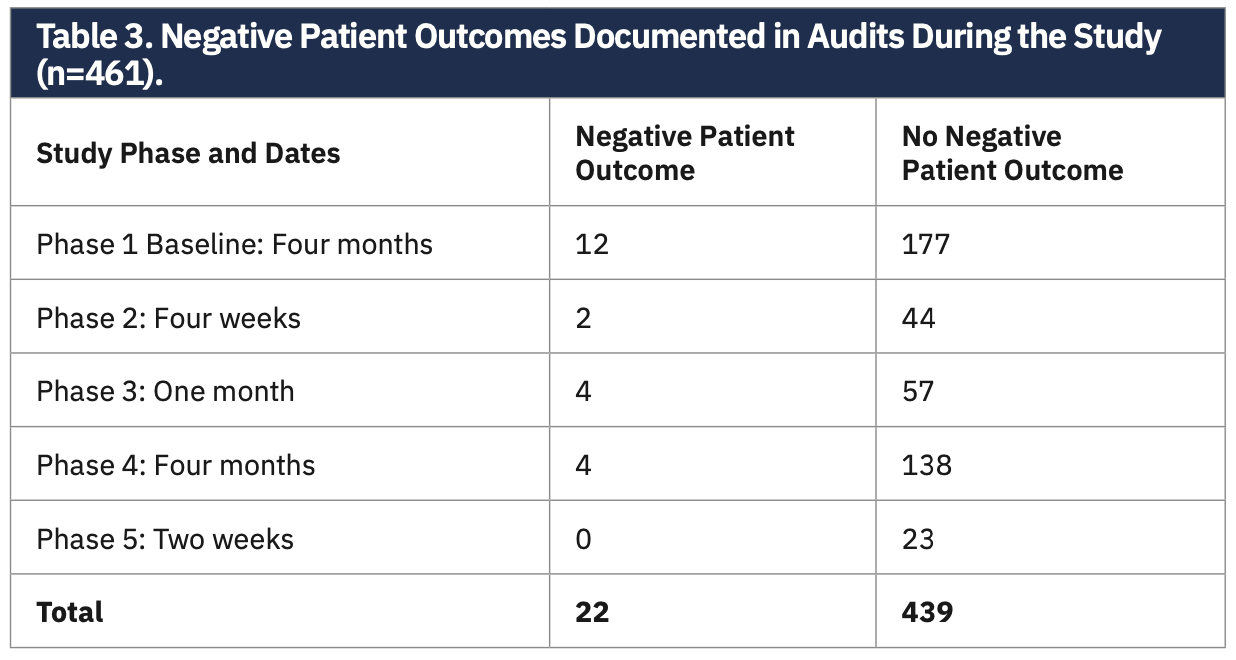
The Arterial Access Audit Form was completed on 461 patients who were admitted to the critical care units, following femoral arterial access for a procedure in the heart center. There were no statistically significant differences in the proportion of negative patient outcomes before and after the implementation of the standardized nurse hand-off process with two-party site verification. However, the number of negative outcomes found during the audits decreased from 12 at baseline to 0 at the conclusion of the study period (Table 3).
Discussion
A standardized handoff report form was designed by nurse stakeholders involved in caring for patients post femoral arterial access for procedures performed in our heart center. Numerous iterations and changes were undertaken until the final standardized form and two-party verification process were approved.
The combined pre and post survey completion rate met our anticipated 30% completion (78/202 = 38.6%), but the pre (35/202 [17.3%]) and post (43/202 [21.2%]) education participation rates were below the 30%. Despite the low survey participation rates, nurses’ self-reported compliance improved with the introduction of the revised hand-off process. Improvement in the standardized of two critical patient care activities (report about and assessment of the arterial access site) also improved with the introduction of the standardized report form and two-party site verification. These care elements were specific to the femoral arterial site, which should decrease potential negative outcomes associated with a femoral arterial access site. This implication is borne out in the absence of negative outcomes found in the audit after the introduction of the standardized report form and two-party verification of the site.
The paucity of data with the observed compliance to the checklist items was directly related to the COVID-19 pandemic. Due to the restrictions on personnel entering the inpatient units during COVID-19, the completion of observations during nurse hand-offs was not possible. Some observations were conducted via speakerphone, with the principal investigator listening in to complete the observation checklist. Despite this restriction, there remained improvements in 11 checklist items and no change in five items.
Study findings reinforce that a standardized report form and visual verification of the arterial access site improved nurses’ self-reported and observed compliance in communication during nurse hand-off in patients undergoing femoral procedural access. The standardized report form assists staff in establishing a baseline and provides a consistent method for communication regarding care provided during and after the procedure. The two-party verification of the femoral insertion site provides caregivers the opportunity to observe any changes at the procedure site in real time, potentially minimizing any negative outcomes.
Our study’s findings answer or support conclusions drawn from the systematic review conducted by Galatzan and Carrington2. One conclusion was that a standardized hand-off tool should be flexible enough to meet the needs of nurses using the tools, the patients receiving the care, and the environment in which the care is given, further supported by our study findings. The standardized checklist included patient-specific information crucial to the safe transitions of patients post-procedure who received femoral access, in particular, the two-party verification of the access site. Galatzan and Carrington2 identified a gap in research connecting the use of a standardized hand-off process to patient outcomes. We audited our patients’ charts in real time and found a significant decrease in negative outcomes that could be attributed to miscommunication during the hand-off process.
While nurses’ self-reported confidence in caring for patients post femoral arterial access improved after the education, the finding was not statistically significant. This finding may be attritubed to a misperception that if nurses’ confidence was reported as lacking, there may be consequences, despite the surveys being anonymous and confidential.
Outcomes associated with the implementation research framework12 supported our study. The standardized hand-off process has been accepted by RNs and ALS technicians in the heart center and critical care units. Nurses continue to comply with the standardized hand-off process and two-party verification for patients with both arterial and femoral access for procedures. Anecdotal evidence from staff in the heart center and critical care units shows that staff are pleased with and have accepted the standardized hand-off process, making the transition between staff more reliable and safe. Since the completion of this study, the implementation of the standardized hand-off process continues to demonstrate positive outcomes in communication and documentation among staff, as well as decreased vascular complications among patients. This practice standard has been adopted throughout our health system with similar results in other patient populations.
Critical care nurses receiving heart center patients report that this standardized approach is an added benefit to the nurse knowledge exchange process, allowing the receiving nurse to focus on relevant information in an unhurried manner. Patient data are readily reported to the oncoming nurse with ease, making this hand-off process feasible and cost effective. Thus, having a standardized approach to nurse hand-off in practice can prevent miscommunication and promote a safe transition of care, making it a sustainable process.
The most significant limitation to this study was the onset of the COVID-19 pandemic at the commencement of the study. Our study was delayed for three months while we prepared for COVID-19 patient admissions. All non-emergent procedures and non-essential programs were placed on hold, changing our heart center census. Nurse dyads could not be observed on the study units due to COVID-19 restrictions. The study units were particularly affected with increased COVID-19 patient admissions and decreased heart center admissions. Once our study concluded, audit data were no longer collected routinely due to the surge in COVID-19 patient admissions. However, there has not been an increase in the number of patient cases with negative outcomes brought to the attention of the Interventional Cardiology Quality Committee.
Nurses can replicate our study methods to create or revise their nurse hand-off process to include a standardized report form and visual assessment component. Ongoing audits are imperative to track compliance with the hand-off process and presence of negative patient outcomes. In the near future, our heart center will be performing more complex procedures, including transcatheter aortic valve replacement.
Conclusion
Testing methods to prevent communication breakdowns during nurse hand-off can promote compliance with established procedures and prevent negative patient outcomes. Using a standardized checklist and visual verification of assessment parameters promotes consistency and completeness in communication during the nurse hand-off process.
Acknowledgements: The authors thank Lisa Marie Bernardo, PhD, MPH, RN, for her thoughtful review of the manuscript, and Helen Burns, PhD, RN, NEA-BC, FAAN, and Mary Mantese, DNP, RN, CENP, for their support and oversight of the project.
Disclosures: The authors report no conflicts of interest regarding the content herein.
The authors can be contacted via Melissa Anderson, MSN, RN, CCRN, at manderson@excelahealth.org
References
1. The Joint Commission Center for Transforming Healthcare. Hand-off communications. Accessed April 14, 2022. https://www.centerfortransforminghealthcare.org/improvement-topics/hand-off-communications/
2. Galatzan B, Carrington J. Exploring the state of the science of the nursing hand-off communication. CIN: Computers, Informatics, Nursing. 2018; 36(10): 484-493.
3. O’Rourke J, Abraham J, Riesenberg LA, et al. A Delphi study to identify the core components of nurse to nurse handoff. J Adv Nurs. 2018; 74(7): 1659-1671. https://doi.org/10.1111/jan.13565
4. White-Trevino K, Dearmon V. Transitioning nurse handoff to the bedside: engaging staff and patients. Nurs Adm Q. 2018;42(3):261-268. https://doi.org/10.1097/NAQ.0000000000000298
5. Prasad A, Cios T, Staub-Juergens W, et al. Standardization improves postoperative patient handoff experience for junior clinicians. Am J Manag Care. 2020; 26(6): e184-e190. doi: 10.37765/ajmc.2020.43494.
6. Ayaad O, Haroun A, Yaseen R, et al. Improving nurses’ hand off process on oncology setting using lean management principles. Asian Pac J Cancer Prev. 2019; 20(5): 1563-1570. https://doi.org/10.31557/APJCP.2019.20.5.1563
7. Sharp L, Dahlen C, Bergenmar M. Observations of nursing staff compliance to a checklist for person-centred handovers-a quality improvement project. Scand J Caring Sci. 2019; 33: 892-901.
8. Joint Commission Center for Transforming Healthcare releases targeted solutions tool for hand-off communications. Jt Comm Perspect. 2012 Aug; 32(8): 1,3.
9. Kaufman J, Twite M, Barrett C, et al. A handoff protocol from the cardiovascular operating room to cardiac ICU is associated with improvements in care beyond the immediate postoperative period. J Comm J Qual Patient Saf. 2013; 39(7): 306-311.
10. Dixon J, Stagg H, Wehbe-Janek H, et al. A standard handoff improves cardiac surgical patient transfer. J Healthc Qual. 2015; 37(1): 22-32. doi:10.1097/01.JHQ.0000460123.91061.b3
11. McGrath A. CRNA to CVICU RN: Implementation of a standardized patient handoff checklist for post-surgical heart patients. Doctor of Nursing Practice Projects. 2020:94. Accessed April 14, 2022. https://spark.siue.edu/dnpprojects/94
12. Peters DH, Adam T, Alonge O, et al. Implementation research: What it is and how to do it. BMJ. 2013; 347: f6753. doi:10.1136/bmj.f6753.
13. Al-Momani M, AbuRuz M. Incidence and predictors of groin complications early after coronary artery intervention: a prospective observational study. BMC Nurs. 2019 Jun 28; 18: 24. doi: 10.1186/s12912-019-0349-8
14. Kim S, Behnes M, Baron S, et al. Differences of bleedings after percutaneous coronary intervention using femoral closure and radial compression devices. Medicine. 2019; 98(20): e15501. https://doi.org/10.1097/MD.0000000000015501


