

Charting the Course Toward Improved Patient Outcomes in Psoriatic Arthritis (PsA) and Axial Spondyloarthritis (axSpA)
In this white paper, leading experts in the treatment of patients with psoriatic arthritis (PsA) and axial spondyloarthritis (axSpA) summarize the educational gaps among health care providers that prevent optimal patient care. Educational pilot programs targeted to specific providers and practice settings are proposed to address these gaps and improve patient outcomes.
Innovative Educational Pilots Proposed by a United States Immunology Panel of Experts:
Drs Afsaneh Alavi, Dhiman Basu, Irene Blanco, Andrew Blauvelt, Jay Chun, Vinicius Costa Diniz Domingues, Firas George Hougeir, Mark Hwang, Vikas Majithia, Fardina Malik, Soumya Reddy, Elliot D. Rosenstein, Elizabeth Schulman, and Evan Siegel
Additional Support Provided by:
Donna Finale, US Health Equity and Sustainability Lead, UCB Biopharma
Peter L. Goldberg, PhD, Senior Field Medical Lead, Director of Medical Affairs, UCB Biopharma
Disclosures:
UCB provided honoraria to the expert roundtable panelists and funded the writing of this paper. Author disclosures and COIs are pending from the panelists.
Psoriatic arthritis (PsA) and axial spondyloarthritis (axSpA) are chronic immune-mediated inflammatory diseases associated with a substantial burden of disease and a reduced quality of life for patients.1 Delayed diagnosis is a key issue for both conditions, with a mean delay of 2.6 years for patients with PsA and 6.7 years for patients with axSpA.2
The shared goal of UCB, the greater rheumatology community, and organizations such as the American College of Rheumatology (ACR), National Psoriasis Foundation (NPF), and the European Alliance of Associations for Rheumatology (EULAR) is to promote consistency and provide a formal structure for the diagnosis and treatment of PsA and axSpA, as well as to improve expectations regarding outcomes for patients.3-5 Experts in these fields, including dermatologists and rheumatologists from various practice settings, met individually and in group roundtable settings to discuss barriers to optimal care for these patients. These sessions were hosted by UCB. These sessions aimed to improve the understanding of the current state of diagnosis and treatment of these conditions and to identify impactful areas for improvement through feasible interventions.
Ultimately, participants determined that an educational effort was the most practical intervention toward affecting change. We will review key insights from expert panelists about creating these pilot programs, along with consideration of the most impactful audiences, the most effective modes of delivery, and the ideal landscape in which to apply these interventions. Expert panelists agree that educational efforts could decrease the time to diagnosis, increase patient and physician disease awareness, and improve outcomes.
Psoriatic Arthritis
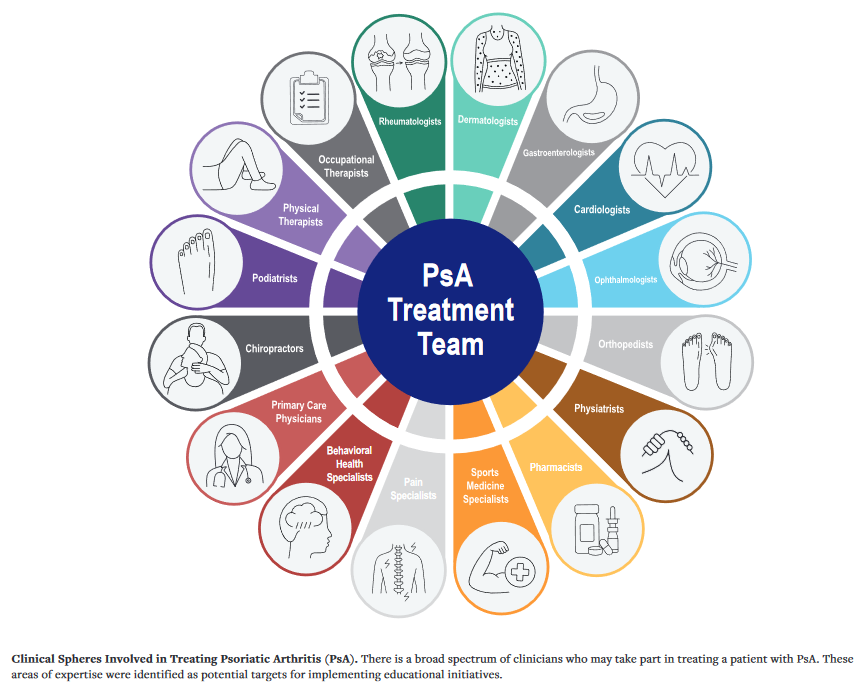
PsA is a chronic immune-mediated inflammatory disease that can lead to progressive joint pain, destruction, and loss of function. Diagnostic and treatment delays of even 6 to 12 months have been associated with irreversible joint damage, poor functional outcomes, and a diminished response to treatment.6 In addition to this reduced quality of life, PsA is associated with considerable economic burden and increased healthcare resource utilization.7 Therefore, the importance of earlier diagnosis, accurate referral, and effective treatment is of significant interest to patients, clinical, payers, and society at large. The expert roundtable considered several key challenges toward optimizing provider and patient education to promote early diagnosis and evidence-based decision-making in treating PsA.
The expert ideation sessions considered this broad array of clinical spheres as targets for feasible, impactful solutions to improve the time to diagnosis and treatment for patients with PsA.
Measuring Disease Activity to Achieve Better Patient Outcomes
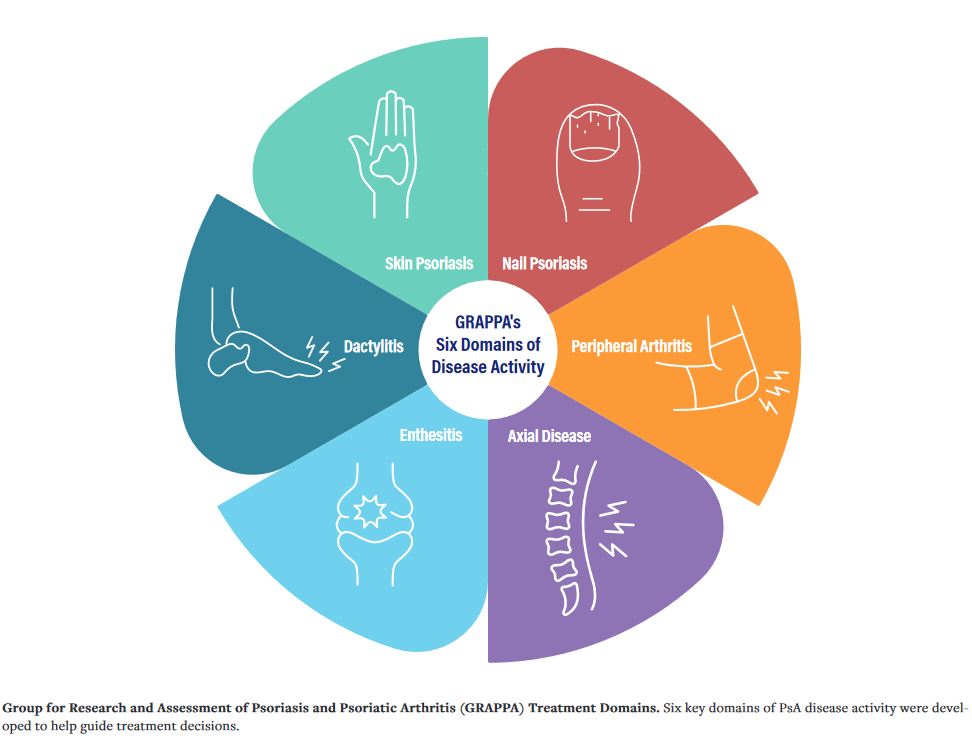
The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) has identified 6 clinical domains of disease activity as part of its treatment schema. Improved clinician and patient education on disease domains in PsA will allow for a more consistent appreciation of symptoms outside of a clinician’s usual focus and may, in turn, offer education and understanding to patients. The core domains are peripheral arthritis, axial disease, enthesitis, dactylitis, skin, and nail psoriasis.8 The updated GRAPPA guidelines recommend consideration of these domains in diagnosis and treatment planning. The expert panel recognized a perceived habit of all rheumatologists to focus on only 1 domain, peripheral joint involvement, limiting their ability to tailor treatment plans to the most active disease area.
Patient-reported outcomes (PROs) incorporate assessments reported directly by individual patients about their symptoms, physical function, and quality of life.9 PRO questionnaires are used to systematically evaluate patients’ symptoms in routine clinical practice. Doing so has improved patient-clinician communication, clinician awareness of symptoms, symptom management, patient satisfaction, quality of life, and overall survival, according to several studies.9
The panel identified failure to recognize all clinical domains involved in a patient’s condition—by both dermatologists and rheumatologists—was identified by the panel as another factor that contributes to delayed diagnosis of PsA. In one real-world cohort study, most patients with PsA were found to have disease across multiple domains. This was associated with higher disease activity and worse quality of life.10 The experts agreed that working with community rheumatologists to increase the consistent use of outcome measures, such as minimal disease activity (MDA), could help monitor patients, once diagnosed, for treatment effectiveness. As is true of other immune-mediated inflammatory diseases, experts now recommend a treat-to-target approach in treating and monitoring patients with PsA.11 In a treat-to-target approach, the healthcare provider chooses an outcome, such as a state of remission or low disease activity (LDA), to objectively follow at each visit. The provider can then adjust therapies to bring the patient to this target.12 This is in line with GRAPPA guidelines, which list the therapeutic goal as the lowest possible level of disease activity, or MDA, in all domains.
Treatment Planning Based on Disease Activity by Domain
Biologic disease-modifying antirheumatic drugs (bDMARDs) may be considered a preferred treatment for patients with more disease activity in certain domains.27 Certainly, the severity of disease in any or all of the domains may impact selection of an appropriate bMARD. Consideration of domains is important in selecting the most effective therapy for an individual patient. The ACR recommends that a chosen therapy for PsA should address all active disease domains.8 The expert panel concluded that education on domains of PsA for rheumatologists could promote informed treatment decisions and elevate outcome expectations.
The panel also considered education on bDMARDs and domains. Education among both patients and providers is lacking regarding when to start bDMARDs and in which patient, what disease domains to consider when deciding treatment, when to switch to another bDMARD, and how to balance benefits and adverse events associated with various bDMARDs. Providing such education can encourage productive communication between the patient and provider to ultimately improve patient outcomes.
Greater Engagement with Dermatologists in the Coordination of Care
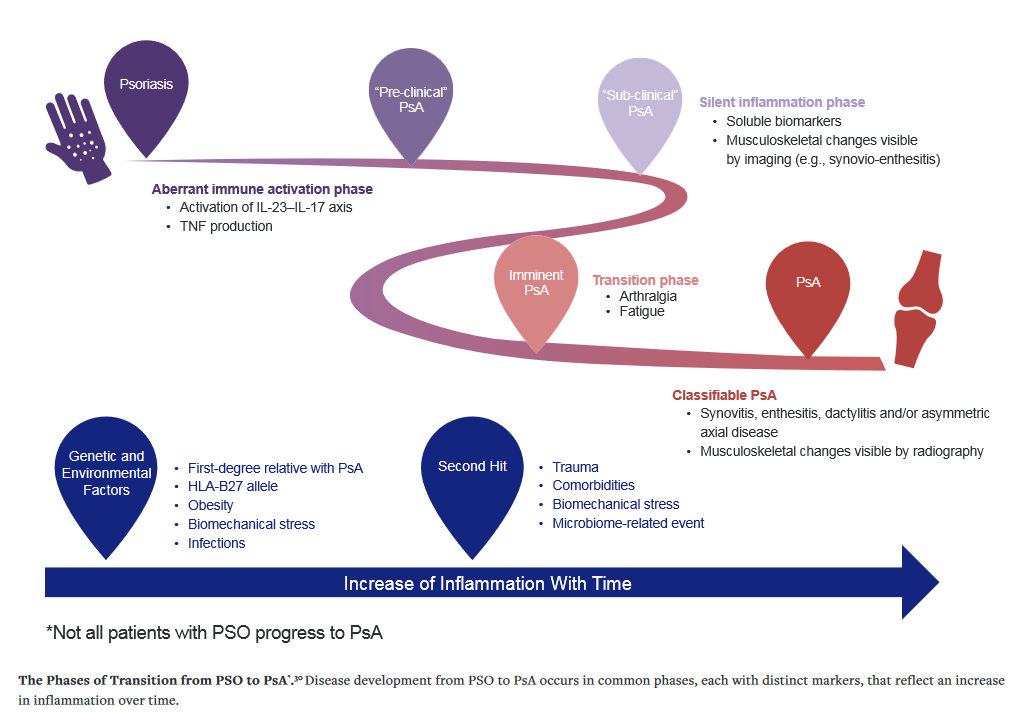
Dermatologists play an important role in the early identification of PsA, as up to 40% of patients with psoriasis (PSO) may progress to PsA.28 Delayed diagnosis and treatment can lead to significant long-term progression.28 Dermatologic complaints generally precede joint involvement by several years, making dermatology providers an ideal group to focus educational interventions. The guidelines of the American Academy of Dermatology(AAD) and the NPF both call for screening patients with PSO for PsA “essential at each visit.”29 Our expert panel identified the failure of some dermatologists to recognize inflammatory joint complaints among patients with PSO as a significant and modifiable issue. They concluded that a simple patient interview assessing for inflammatory joint pain (e.g., pain worse in the morning, better with activity) may be sufficient in reducing diagnostic delays.29
The panel also identified that communication between and coordination among dermatologists and rheumatologists is suboptimal and may play a role in delayed diagnosis and effective treatment for patients with PsA. One potential consideration discussed was leveraging technology to improve access to timely rheumatologic care. The panel proposed telemedicine as one potential mode of a patient-physician interface that could overcome some of the barriers to care (e.g., distance to a rheumatologist) that patients face. Telemedicine can allow access to medical care for patients who live in remote or rural areas and for patients with severe disabilities who cannot travel for an in-person visit.31
Care coordination is the organization of information and sharing of care plans among various providers to achieve safe and effective care for patients. Patients with chronic, complex conditions, including PsA, may benefit from the support offered through coordinated care frameworks. Several health systems use coordination of care between dermatology and rheumatology to improve results for their patients with PSO and PsA.32 For example, the Cleveland Clinic developed a dermatology–rheumatology clinic, which they note has led to improved patient outcomes.32 The Brigham and Women’s Hospital has similarly developed a Center for Skin and Related Musculoskeletal Diseases, which offers multidisciplinary care to patients with psoriatic disease by attending rheumatologists and dermatologists.33 In this way, the clinic offers coordinated care while contributing to the cross-specialty education of future dermatologists and rheumatologists. However, the expert panel noted that there may be real-world impediments to establishing such clinics. In the absence of a designated care center or clinic, opportunities for coordinated care also exist within referral and/or telemedicine networks.
Patient-Provider Trust
Likewise, communication between patient and provider offers benefits to patients. Shared decision-making is a process through which patients and clinicians work collaboratively to review outcome goals and create treatment plans. Shared decision-making can result in treatment plans that better reflect patient goals, increase both patient and physician satisfaction, and have a positive effect on patient outcomes.34 The expert panel agreed that encouraging shared decision making and prioritizing patients’ needs to align on goals of care is essential.
Charting the Course Toward Improved Patient Outcomes in PsA
The expert panel proposed an educational pilot program structured to support improved care in the management of PsA. Educational efforts would be aimed at primary care physicians, dermatologists, rheumatologists, and advanced practice providers (APPs) within dermatology and rheumatology practices.
1. Educate on the Domain
The expert panel agreed that community rheumatologists are generally not utilizing domains when diagnosing or assessing patients with PsA. Educational materials could use the GRAPPA-identified six clinical domains as a scaffold on which to build a comprehensive and impactful program
The panel identified rheumatology fellows as a potentially high-yield population for the above interventions. Rheumatology APPs would also be a focus for educational interventions. The program would leverage regional networking opportunities for the dissemination of educational materials to both physicians and APPs, and it could explore opportunities to partner with the NPF and Psoriasis & Psoriatic Arthritis Clinics Multicenter Advancement Network (PPACMAN).
2. Increase the Use of Formal Measures of Disease Activity
The panel recommends the creation and implementation of an electronic medical record (EMR) to increase the use of outcome measures in clinical practice. This may include the use of PROs to assess patient symptoms such as pain and fatigue. The creation of a PsA-specific EMR template could prompt rheumatologists and dermatologists to consider the domains and track treatment response (e.g., MDA or psoriatic arthritis impact of disease, PSAID) more consistently and efficiently.
3. Educate on the Use of Domains in Treatment Planning
Consideration of domains is important in diagnosing and creating treatment plans for patients with PsA, in particular, in a treat-to-target approach. The expert panel recommended education on how to choose therapy to best address active domains, on assessing treatment response by domain, and when deciding whether to continue or switch medications. Education should include information on the components of MDA and its simplicity. The goal is to increase rheumatologists’ use and knowledge of MDA, as well as the importance of treating all domains. Additionally, the creation of a clinician reference with up-to-date educational materials on bDMARDs and their mechanisms of action could allow for more frequent achievement of MDA.
4. Provide Updated Education on bDMARDs
The panel also recommended educational materials on initiating, switching, adding, or removing bDMARDs in patients with PsA. It also recommended to provide materials on benefits and adverse events associated with various bDMARDs for patients and providers.
5. Educate Other Practitioners Caring for Patients With PsO
The expert panel recommended educating community dermatologists on the progression of disease from PSO to PsA to facilitate timelier referral of appropriate patients to rheumatology. Creating and implementing specialized EMR templates to prompt dermatologists to screen for PsA in their patients with PSO was recommended as a part of this effort. Educational materials or programs could be disseminated using regional networking opportunities. The expert panel identified dermatology residents as a potentially high-yield group. An APP could teach separate educational programs for dermatology APPs, so that each type of practitioner learns from a peer expert. The expert panel noted that a focus on APPs may, in areas where medical dermatology is performed largely by APPs, have a significant impact on earlier referrals to rheumatology.
Establishing expedited referral pathways for patients with signs or symptoms of PsA between dermatology and rheumatology may allow for quicker evaluation and, thus, treatment. The educational pilot program could enhance communication between specialties and improve the coordination of multispecialty care across provider networks.
Primary care providers (PCPs) may also be involved in the diagnosis and initial management of PSO, and the expert panel indicated that they could benefit from their own tailored and updated education on signs of progression from PSO to PsA.35 The proposed educational pilot program would emphasize the importance of assessing PSO patients for joint symptoms in order to intervene early and prevent irreversible joint damage. This pilot program would also include education on appropriate referrals and initial work-up for patients with suspected PsA to facilitate the appropriate care once a patient has transferred care to rheumatology. Because PSO is associated with an increased risk of several chronic conditions (e.g., cardiovascular disease, diabetes, depression), developing targeted educational materials for PCPs could help ensure routine screenings for these co-morbidities and appropriate follow-up for treatment.35 HCPs could leverage regional networking opportunities to connect and provide education on disease state, domains, treatment guidelines, and associated co-morbidities. Primary care APPs could also take advantage of educational opportunities.
6. Educate Patients With PsO About PsA
Educating patients with PSO on the signs and symptoms of PsA may promote earlier diagnosis and treatment.36 UCB is proud to have supported patient education efforts with the International Federation of Psoriasis Associations (IFPA). Educational materials for patients may include digital educational displays in primary care and dermatology practices, alerting patients with PSO to the signs and symptoms associated with PsA. Direct-to-patient educational materials and simplified self-administered screening tools in addition to those used by providers, such as the Psoriasis Epidemiology Screening Tool (PEST), may also be impactful.37 UCB is proud to have partnered with IFPA and rheumatologists to present Good Care, which raises awareness about new treatment guidelines and can help improve the quality of life for those living with PsA.3
Axial Spondyloarthritis (axSpA)
axSpA is a chronic immune-mediated inflammatory disease that affects more than 1% of adults in the United States and is associated with decreased quality of life, increased mortality, and substantial healthcare-related costs.39 The term axSpA encompasses both ankylosing spondylitis (AS/r-axSpA) and non-radiographic axSpA (nr-axSpA), which are distinguished by the presence or absence of sacroiliitis on x-ray.40 axSpA is challenging to diagnose, in part, because chronic back pain is highly prevalent in the general population, and axSpA only accounts for about 5% of cases of those suffering from back pain.40 As such, axSpA is associated with delays in diagnosis as well as proper intervention, increasing the risk of functional impairment for patients.2
Experts identified 5 key challenges to axSpA patients reaching optimal care outcomes: 1) increased use of outcome measures; 2) understanding the true burden of disease; 3) diagnostic delays; 4) care coordination between specialties; and 5) educational gaps for clinicians. The panel suggested that an educational pilot program would be a feasible intervention that could effect change in these areas, with the goal of optimizing provider education to promote evidence-based therapeutic decision-making.
Outcome Measures
The expert panel agreed that the diagnosis of axSpA is challenged by the lack of clear diagnostic criteria and confusion regarding the differences in the classification and diagnosis of axSpA. Classification criteria are designed for the purpose of clinical studies, whereas diagnostic criteria are used for individual patients in clinical practice.41 Because current practice guidelines for spondyloarthritis are based on classification criteria (e.g., Assessment of Spondyloarthritis International Society [ASAS]), conservative treatment practices may dictate that if a patient does not meet these criteria, then the patient does not have the disease and therefore, cannot be treated with a biologic. The patient may indeed have the disease but simply does not satisfy the stringent classification criteria. A validated diagnostic paradigm for axSpA that is designed for clinical practice may allow earlier treatment of this condition by rheumatologists in a variety of practice settings.
Classic measures of disease activity are important, not only in diagnosis, but also in assessing treatment response. Currently, disease activity for patients diagnosed with axSpA can be assessed using the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) or the Ankylosing Spondylitis Disease Activity Score (ASDAS). The expert panel discussed these outcome measures, and the consensus was that facilitating their use by the wider rheumatology community would be beneficial. A simplified tool such as the Routine Assessment of Patient Index Data 3 (RAPID3), which is already widely used, may be helpful. One panel member felt that if rheumatologists better understood the impact of axSpA on patient quality of life, the use of formal measures (e.g., BASDAI, ASDAS) may be more commonly utilized in clinical practice.
Burden of Disease
Disease activity, function, mobility, quality of life, and work productivity all contribute to the burden of disease in axSpA. The true disease burden in axSpA, particularly without the use of classic measures, may be difficult to appreciate. Educating rheumatologists and other health care providers on axSpA and the associated disease burden could increase the consistent use of outcome measures and the urgency to initiate appropriate treatment.
Diagnostic Delay
The delay to diagnosis for axSpA is longer than many rheumatologic conditions, with a reported range of 2 to 10 years.2,42 This diagnostic delay is multifactorial, and it can result in functional impairment, poor quality of life, reduced response to treatment, and a significant burden to patients and society.2 Part of the diagnostic delay for patients with spondyloarthritis is due to physician unfamiliarity with the heterogeneous clinical presentation of the condition and lack of proper screening.43
We have come a long way since the 1950s. Diagnostic delays experienced by patients with axSpA have decreased. However, studies from the past several decades suggest that this decrease in delay until diagnosis may be plateauing.42 Thus, there is a need for continued development in this area toward optimizing the health of affected populations. Increasing disease awareness and improving accurate and timely referrals could improve diagnostic delays in patients with axSpA.44 The consensus from the expert panel was a goal to reach the aims of the treat-to-target approach by 6 months.
Care Coordination and Referral
Inflammatory back pain (IBP) criteria are useful in screening for axSpA. However, studies evaluating strategies for referral to a rheumatologist showed that only 17% to 33% of at-risk patients with IBP were diagnosed with axSpA, indicating that these criteria alone are not sufficient.39
The expert panel reviewed challenges related to care coordination and referrals and determined that both contribute to delayed diagnosis and treatment. Improved diagnosis and screening tools, as well as increasing recognition of IBP and referring patients who screen positive, could have a significant impact on the time to diagnosis and appropriate treatment. The expert panel identified specialties that would be important to target in interventions aimed at timelier referral to rheumatology.

Educational Gaps
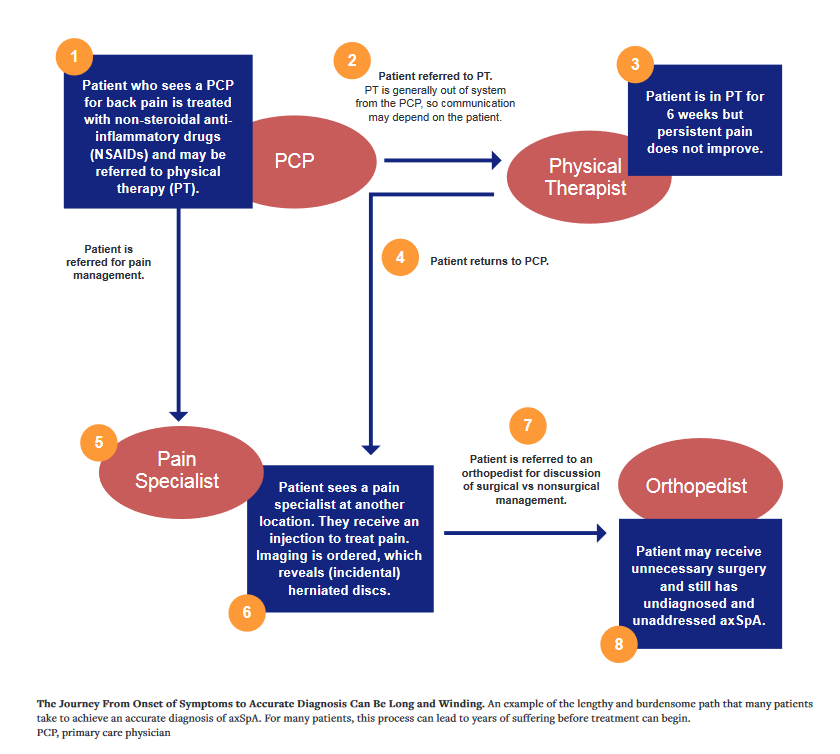
Only 37% of patients with ankylosing spondylitis in the United States are diagnosed by rheumatologists. The remainder of patients are diagnosed by practitioners in primary care (26%), chiropractic medicine/PT (7%), orthopedic surgery (4%), pain clinics (4%), and other settings (19%).40 This underscores the importance of directing educational interventions at a variety of specialties for improved referrals and diagnosis.
The expert panel agreed that one of the most important initial steps in accurate diagnosis for patients with axSpA is to differentiate between IBP and mechanical back pain (MBP). Clinicians who often see and manage patients with back pain or other typical axSpA features are not consistently aware of the concept of IBP or extra-spinal manifestations.45 One study of PCPs found that only 60% were aware of differences between MBP and IBP.45 This can lead to misdiagnosis and missed referrals. Patients can be referred to the wrong type of specialist based on inaccurate diagnosis of back pain, which costs both the patient and provider time. Specific spondyloarthritis-aimed training has been shown to improve appropriate PCP referrals of patients with symptoms of axSpA by more than 40%,43 indicating that educational interventions have a proven ability to improve referral and diagnosis for these patients.
The panel also identified improving patient education in axSpA as an important goal. Patient education in this area has been shown to contribute to improved treatment goals.46
Charting the Course Toward Improved Patient Outcomes in axSpA
A potential educational pilot program proposed by the expert panel would be aimed at primary care physicians, chiropractors, physical therapists, orthopedists, spine surgeons, rheumatologists, and APPs and/or nurses within these practices, with the goal of increasing timely diagnosis of axSpA. A partnership with an integrated delivery network (IDN) could focus on clinician education to improve patient journeys to effective treatment.
1. Increase the Use of Formal Measures
This educational pilot program would promote the use of ASDAS as a treatment target for patients with axSpA. Integration of ASDAS LDA into the EMR may facilitate its increased use in daily clinical practice. Furthermore, PRO assessments can provide a systematic evaluation to monitor a patient’s symptoms. Integration of these measures into the EMR would likely increase consistency in utilizing these tools and obtaining valuable data. However, effective design and workflow must be considered to reach full potential use.47
2. Understand the Burden of Disease
Improved awareness of axSpA among PCPs and increased understanding of the burden of disease may encourage timely referrals to rheumatologists, allowing earlier diagnosis and effective management, which could improve long-term outcomes.48-49
3. Address Diagnostic Delays
Most patients with back pain present to non-rheumatologists for evaluation. One of the most significant barriers to timely and appropriate referral to rheumatology, as identified by our expert panel, is a poor understanding of MBP vs IBP. Thus, increasing education to improve knowledge on IBP would be a focus of the proposed educational pilot. Development or modification of an IBP questionnaire may allow non-rheumatologists to identify IBP and thus refer to rheumatology more quickly from chronic back pain populations seeking medical care. For patients and practices using online intake forms electronically sent to patients, an IBP questionnaire could even allow appropriate triage before the patient has seen the frontline clinician.
4. Improve Care Coordination
This pilot program would aim to improve care coordination and care facilitation to help expedite diagnosis and treatment. The expert panel recommended educational interventions, which may improve timely and accurate referrals to rheumatology. An important consideration is the volume of referrals that could be generated and the bottleneck that may result because of the possible misdiagnosis of MBP.
5. Address Disease State Educational Gaps
Education of non-rheumatologists should focus on the identification of IBP and the irreversible damage that a delayed axSpA diagnosis could cause, underscoring the urgency for referral. Educational targets could include national and regional meetings for internal medicine, family practice, orthopedics, podiatry, or physical therapy. The expert panel believed that education during training would be preferred. Residents and fellows could participate in learning initiatives together, with programs being taught by a physician (e.g., junior faculty). Modules could be created for chiropractic programs as well. If modules are not able to be integrated into training, one-time presentations could be made available and be delivered around the time of graduation.
Education of APPs in relevant fields should also be a focus. The expert panel believed that this population was eager to learn. APP conferences could be a focus for educational efforts (the American Academy of Physicians Assistants, the American Association of Nurse Practitioners, and the Rheumatology Advanced Practice Providers all have annual meetings).
Education for nurses is also an important focus. The expert panel pointed out that nurses are important in clinical settings, as they are active in initial intake, follow-up, and patient education. Nursing congresses could be a target to reach this important audience.
Education for community rheumatologists will aim to improve understanding and use of available tools and treatments. One expert panel member suggested that Spondyloarthritis Research and Treatment Network (SPARTAN)-associated rheumatologists could teach community rheumatologists at national meetings. Education for residents and fellows in this pilot program could consist of modules specifically tailored to signs or symptoms by specialty (e.g., rheumatology [enthesitis, peripheral arthritis, and dactylitis]; gastroenterology [inflammatory bowel disease]; ophthalmology [uveitis], dermatology [psoriasis], and primary care/chiropractic medicine/physiatry [IBP]).
Direct-to-patient questionnaires could help patients identify IBP even before they have sought medical evaluation. Involving patient advocacy organizations, such as the Spondylitis Association of America (SAA), may facilitate reaching appropriate patients. One expert panel member suggested direct-to-patient web-based questionnaires, with recommendations for follow-up care by a rheumatologist if the patient submits positive answers to key questions regarding IBP.
Conclusion
Compiled learnings from the roundtables with the expert panel have facilitated the identification of educational interventions that have the potential to advance the standard of care for patients with PsA and axSpA. The aim of the proposed pilot programs is to reach key participants and directly affect inter-specialty communication and patient care, which would facilitate the timely and accurate diagnosis of PsA and axSpA, expand the number of patients receiving appropriate treatment for these potentially debilitating conditions, and improve overall patient outcomes and quality of life. Mark Kaufmann, MD, FAAD, states, “Last year we integrated the PEST tool into our Advanced Dermatology’s electronic health record in an effort to capture the earliest signs of systemic disease. Building on the success of this we would like to continue to strive for better coordination of care especially between Dermatology & Rheumatology. We are excited to be partnering in our headquartered state of Florida with one of the largest Rheumatology groups to implement education, resources, and share best practices as part of a pilot launching in 2024.” The pilot phase of the proposed educational programs would explore different specialties, practice settings, education levels, and geographic regions toward achieving earlier referral, better diagnosis, and optimal treatment for patients with PsA and axSpA. Andrew Ripps adds, “It is crucial that we work closely with and form relationships between rheumatology and dermatology at the national and local level to accomplish these goals. Perhaps most importantly, the advanced practice providers who integrate into the coordinated care team for these patients need disease, diagnostic and therapeutic education to accurately identify the first signs and earliest symptoms of joint involvement. Leveraging AARA powered by Bendcare Illumination Healths technology platform including provider and patient engagement visualization to monitor progress and digitized resources in early detection will be essential to improve the speed and accuracy of referrals while improving the patient journey and outcomes.” UCB is strategizing methods with a wider group of stakeholders to operationalize this educational initiative. Through a partnership with Advanced Dermatology and Bendcare, a pilot educational module program is in development to facilitate the implementation of these insights and lead to meaningful practice change.
References:
1. Garrido-Cumbrera M, Hillmann O, Mahapatra R, et al. Improving the management of psoriatic arthritis and axial spondyloarthritis: roundtable discussions with healthcare professionals and patients. Rheumatol Ther. 2017;4(2):219-231.
2. Zhao SS, Pittam B, Harrison NL, Ahmed AE, Goodson NJ, Hughes DM. Diagnostic delay in axial spondyloarthritis: a systematic review and meta-analysis. Rheumatology (Oxford). 2021;60(4):1620-1628.
3. Tran G. American College of Rheumatology (ACR) - Advocating for Better Care and Treatment. American EHR. Published April 18, 2023. Accessed September 18, 2023. https://www.americanehr.com/american-college-of-rheumatology/
4. Strategic Plan. www.psoriasis.org. Accessed September 18, 2023. https://www.psoriasis.org/strategic-plan/
5. About EULAR Advocacy. EULAR. Accessed September 14, 2023. https://www.eular.org/about-eular-advocacy
6. Karmacharya P, Wright K, Achenbach SJ, et al. Diagnostic delay in psoriatic arthritis: a population-based study. J Rheumatol. 2021;48(9):1410-1416.
7. Ogdie A, Hwang M, Veeranki P, et al. Health care utilization and costs associated with functional status in patients with psoriatic arthritis. J Manag Care Spec Pharm. 2022;28(9):997-1007.
8. Coates LC, Soriano ER, Corp N, et al. Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA): updated treatment recommendations for psoriatic arthritis 2021 [published correction appears in Nat Rev Rheumatol. 2022 Dec;18(12):734]. Nat Rev Rheumatol. 2022;18(8):465-479. doi:10.1038/s41584-022-00798-0
9. Basch E, Barbera L, Kerrigan CL, Velikova G. Implementation of patient-reported outcomes in routine medical care. Am Soc Clin Oncol Educ Book. 2018;38:122-134. doi:10.1200/EDBK_200383.
10. Ogdie A, Hur P, Liu M, et al. Effect of multidomain disease presentations on patients with psoriatic arthritis in the corrona psoriatic arthritis/spondyloarthritis registry. J Rheumatol. 2021;48(5):698-706.
11. Gossec L, McGonagle D, Korotaeva T, et al. Minimal disease activity as a treatment target in psoriatic arthritis: a review of the literature. J Rheumatol. 2018;45(1):6-13.
12. Ogdie A, Coates LC, Gladman DD. Treatment guidelines in psoriatic arthritis. Rheumatology (Oxford). 2020;59(Suppl 1):i37-i46. doi:10.1093/rheumatology/kez383.
13. Lindenmann J, Burke DC, Issacs A. Studies on the production, mode of action and properties of interferon. Br J Exp Patho. 1957;38(5):551-562.
14. Liu X, Sun S, Liu D. IL-17D: a less studied cytokine of IL-17 family. Int Arch Allergy Immunol. 2020;181(8):618-623.
15. Johansen C, Usher PA, Kjellerup RB, Lundsgaard D, Iversen L, Kragballe K. Characterization of the interleukin-17 isoforms and receptors in lesional psoriatic skin. Br J Dermatol. 2009;160(2):319-324. doi:10.1111/j.1365-2133.2008.08902.x.
16. Menter A, Korman NJ, Elmets CA, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 4. Guidelines of care for the management and treatment of psoriasis with traditional systemic agents. J Am Acad Dermatol. 2009;61(3):451-485. doi:10.1016/j.jaad.2009.03.027.
17. Rønholt K, Iversen L. Old and new biological therapies for psoriasis. Int J Mol Sci. 2017;18(11):2297. doi:10.3390/ijms18112297
18. Enbrel. Prescribing information. Amgen Inc; 2021.
19. Taltz. Prescribing information. Eli Lilly and Co; 2021.
20. Siliq. Prescribing information. Bausch Health US LLC; 2020.
21. Tremfya. Prescribing information. Janssen Biotech Inc; 2020.
22. Ilumya. Prescribing information. Sun Pharma; 2020.
23. Skyrizi. Prescribing information. AbbVie Inc; 2021.
24. Stelara. Prescribing information. Janssen Biotech Inc; 2020.
25. Otezla. Prescribing information. Amgen Inc; 2020.
26. Cosentyx. Prescribing information. Novartis Pharmaceuticals Corp; 2021.
27. McInnes IB, Sawyer LM, Markus K, LeReun C, Sabry-Grant C, Helliwell PS. Targeted systemic therapies for psoriatic arthritis: a systematic review and comparative synthesis of short-term articular, dermatological, enthesitis and dactylitis outcomes. RMD Open. 2022;8(1):e002074.
28. Cho HH, Kim BS. Diagnosing psoriatic arthritis from the dermatologist's view. J Lifestyle Med. 2013;3(2):85-90.
29. van Hal TW, Van den Reek JM, Groenewoud HM, et al. Discovery of Arthritis in Psoriasis Patients for Early Rheumatological Referral (DAPPER): protocol for a longitudinal observational study. JMIR Res Protoc. 2021;10(11):e31647.
30. Scher J et al. Preventing psoriatic arthritis: focusing on patients with psoriasis at increased risk of transition. Nat Rev Rheumatol. 2019;15:153-166.
31. Gottlieb AB, Wells AF, Merola JF. Telemedicine and psoriatic arthritis: best practices and considerations for dermatologists and rheumatologists. Clin Rheumatol. 2022;41(5):1271-1283.
32. Profiles in care: importance of a coordinated health care plan in plaque psoriasis and psoriatic arthritis management. American Journal of Managed Care. Published July 20, 2021. Accessed June 19, 2023. https://www.ajmc.com/view/profiles-in-care-importance-of-a-coordinated-health-care-plan-in-plaque-psoriasis-and-psoriatic-arthritis-management
33. Rheumatology-dermatology collaboration enhancing PsA care. Brigham and Women's Hospital. Accessed June 19, 2023. https://www.brighamhealthonamission.org/2021/01/27/rheumatology-dermatology-collaboration-enhancing-psa-care/
34. The consumer benefits of patient shared decision making. Altarum. Published May 2019. Accessed June 19, 2023. https://www.healthcarevaluehub.org/application/files/8115/6367/3510/RB_37_-_Shared_Decision_Making.pdf
35. Kim WB, Jerome D, Yeung J. Diagnosis and management of psoriasis. Can Fam Physician. 2017;63(4):278-285.
36. Armstrong A, Bohannan B, Mburu S, et al. Impact of psoriatic disease on quality of life: interim results of a global survey. Dermatol Ther (Heidelb). 2022;12(4):1055-1064.
37. Ibrahim GH, Buch MH, Lawson C, Waxman R, Helliwell PS. Evaluation of an existing screening tool for psoriatic arthritis in people with psoriasis and the development of a new instrument: the Psoriasis Epidemiology Screening Tool (PEST) questionnaire. Clin Exp Rheumatol. 2009;27(3):469-474.
38. Good care. IFPA. Accessed July 26, 2023. https://ifpa-pso.com/projects/psoriatic-arthritis-awareness
39. Walsh JA, Magrey M. Clinical manifestations and diagnosis of axial spondyloarthritis. J Clin Rheumatol. 2021;27(8):e547-e560.
40. Danve A, Deodhar A. Axial spondyloarthritis in the USA: diagnostic challenges and missed opportunities. Clin Rheumatol. 2019;38:625–634.
41. Braun J, Baraliakos X, Kiltz U, Heldmann F, Sieper J. Classification and diagnosis of axial spondyloarthritis--what is the clinically relevant difference? J Rheumatol. 2015;42(1):31-38.
42. Hay CA, Packham J, Ryan S, Mallen CD, Chatzixenitidis A, Prior JA. Diagnostic delay in axial spondyloarthritis: a systematic review. Clin Rheumatol. 2022;41(7):1939-1950.
43. van Onna M, Gorter S, Maiburg B, Waagenaar G, van Tubergen A. Education improves referral of patients suspected of having spondyloarthritis by general practitioners: a study with unannounced standardised patients in daily practice. RMD Open. 2015;1(1):e000152.
44. Feld J, Elkayam O, Druyan A, et al. Improvement in the diagnostic delay of axial spondyloarthritis, results from real world data. Ann Rheum Dis. 2021;80:753.
45. Kumthekar A, Bittar M, Dubreuil M. Educational needs and challenges in axial spondyloarthritis. Curr Opin Rheumatol. 2021;33(4):313-318.
46. van der Kraan YM, Paap D, Lennips N, et al. Patient’s perspective on patient education in axial spondyloarthritis: a qualitative study. Ann Rheum Dis. 2021;80:1268.
47. Zhang R, Burgess ER, Reddy MC, et al. Provider perspectives on the integration of patient-reported outcomes in an electronic health record. JAMA Open. 2019;2(1):73-80.
48. Magrey MN, Danve AS, Ermann J, Walsh JA. Recognizing axial spondyloarthritis: a guide for primary care. Mayo Clin Proc. 2020;95(11):2499-2508.
49. Kiltz U, Wendling D, Braun J. ASAS health index: the "all in one" for spondyloarthritis evaluation? J Rheumatol. 2020;47(10):1457-1460. doi:10.3899/jrheum.200708
