Case of the Quarter: Asthma’s Deadly Triad

EMS World’s new Case of the Quarter feature is developed by Texas’ Montgomery County Hospital District EMS to share lessons learned with the wider EMS community. For further discussion of this case, visit www.emsworld.com/podcasts.
Pediatric asthma currently affects 7% of children living in the United States and is the third-most common cause of childhood hospitalization. Given advances in the recognition and treatment of asthma, yearly childhood asthma deaths in our country have been reduced by more than half.1 First responders must stay vigilant, as their next call may place them in the face of asthma’s deadly triad.
Staffed by 250 paramedics and supported by 12 regional first responder organizations, Montgomery County Hospital District (MCHD) EMS is a publicly funded 9-1-1 provider from Montgomery County, Texas. MCHD provides 9-1-1 EMS service to 1100 square miles just north of Houston and answers more than 75,000 calls a year. This article follows an MCHD crew as it responds to the cardiac arrest of an asthmatic pediatric patient.
The Call
An 8-year-old female, unresponsive, in cardiac arrest. CPR by caller, assisted by an alarm medic.
En route paramedics gather pertinent information and review differential diagnoses for pediatric cardiac arrest. They also utilize the Handtevy pediatric resuscitation app to review equipment sizes and drug dosages.
Initial Differential
Pneumothorax, pneumonia, anaphylaxis, foreign body, trauma/nonaccidental trauma, acute decompensated heart failure, near-drowning, seizure/CNS disorder, toxic ingestion leading to depressed ventilation.
On Scene
The patient is an 8-year-old child with a history of severe asthma (previous ICU admissions and intubation) found unresponsive, with a family member now performing operator-assisted CPR. Per the family the patient had respiratory distress for 1 day and collapsed at home a few hours after returning from school. She was found to have a femoral pulse on initial check, and CPR was halted.
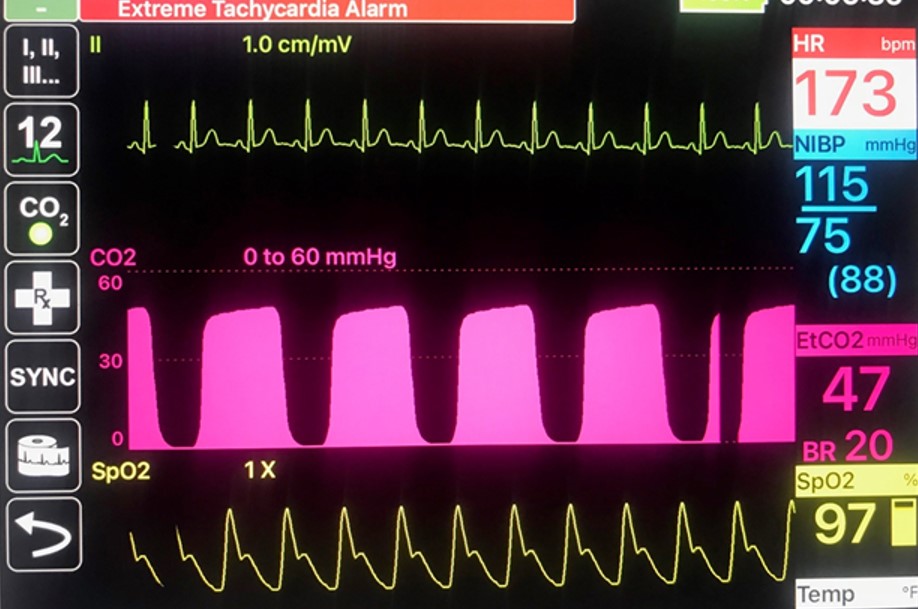
A primary survey revealed an unresponsive young girl with agonal respirations and no obvious signs of injury. A lung exam revealed diminished breath sounds with diffuse wheezing bilaterally. Retractions of the chest wall were also observed. Figure 1 reflects her monitor display.
Pathophysiology
Respiratory compromise and cardiac arrest in the asthmatic patient occur through a cascade of events. These can be separated into two types: bronchoconstriction of the conducting airways and inflammatory changes in the conducting airways. Both mechanisms can impair oxygenation and ventilation. Inflammatory changes cause inflammation of the airways, along with excess mucus production. Bronchoconstriction can result in breath stacking, where the tidal volume of a breath can get in but not be exhaled completely due to the constriction of the airways. This extra volume of air in the chest increases with each incompletely exhaled breath, causing increased intrathoracic pressure, decreased venous return to the heart, and therefore compromising circulation. This deadly triad of respiratory exhaustion, respiratory acidosis, and impaired venous return can lead to cardiac arrest and is most likely the cause of this child’s cardiorespiratory arrest.
Load and Go or Stay and Play?
Given the nontraumatic nature of this patient’s arrest, the crew decided to treat and stabilize on scene prior to transport. The decision to stay on the scene of a pediatric cardiac arrest and run the code, rather than choosing early transport, allows for early deployment of oxygenation and ventilation management. This includes placement of an advanced airway and administration of epinephrine and fluid to support or restore circulation. Peer-reviewed data suggests the “stay and play” approach may improve neurologically intact survival. In one study this went from 0% to nearly 25% after the approach was implemented.2
Interventions
- BVM-assisted ventilations with inline nebulized albuterol and ipratropium
- IM epinephrine, methylprednisolone IVP, magnesium sulfate infusion, and fluid bolus
- Plan for sedation-assisted delayed-sequence intubation (DSI)
The crew prepared for DSI knowing it should always be a last resort for asthmatic patients.3 This is because mechanical ventilation opposes the natural pulmonary physiology, changing ventilation from a negative-pressure process to one of positive pressure. Given the patient’s previous cardiac arrest and instability, the crew opted for DSI to manage the airway.
Positive-pressure ventilation in sick asthmatic patients should be reserved for those who fail conventional therapy with supplemental oxygen, bronchodilators, and IM epinephrine. Asthma’s deadly triad already includes an increase in intrathoracic pressure, and mechanical positive-pressure ventilation will further increase that, to a potentially deleterious effect on cardiac output. Monitor severe asthmatic patients for breath stacking. If it is suspected, mitigate it by manually decompressing the chest using two hands to push down on the chest wall, allowing trapped air to escape via the nose and mouth or tracheal tube.
Another potentially deadly complication of intubating asthmatic patients is pneumothorax. The breath stacking and increased pressure inside the lung may damage the lung and allow the leaking of air into the thoracic cavity. Left untreated this can result in a tension pneumothorax with impaired cardiac output and potentially cardiac arrest.
Prep for DSI
MCHD’s “Rule of 15’s”:
- Head of bed at 15 degrees with ear to sternal notch alignment4
- Apneic oxygenation with nasal cannula at 15 lpm
- Bag-valve mask at 15 lpm w/PEEP of up to 15 cm H2O (if patient is apneic) or NRB at 15 lpm
Clinical Course and Outcome
The patient was successfully intubated using sedation-assisted DSI with ketamine. She was admitted to a local children’s hospital for severe asthma with respiratory failure, requiring ICU-level care. She was discharged home after a week, is now well, and has returned to school at her baseline prearrest neurological status.
Take-home Points
- Prepare prior to scene arrival.
- Give early IM epinephrine and oxygen support; bronchodilator nebs are critical in the sick asthmatic patient.
- Avoid positive-pressure ventilation if possible in the asthmatic patient due to increased breath stacking, decreased cardiac output, and risk for tension pneumothorax.
- “Stay and play” in pediatric cardiac arrest improves outcomes.
- Use a structured bundle of care like MCHD’s “Rule of 15's” when preparing for intubation.
- Delayed-sequence intubation trumps the old RSI (check out the MCHD podcast).
References
1. National Center for Environmental Health. Asthma in children. Centers for Disease Control and Prevention. Published May 10, 2018. www.cdc.gov/vitalsigns/childhood-asthma/index.html
2. Banerjee PR, Ganti L, Pepe PE, et al. Early On-Scene Management of Pediatric Out-of-Hospital Cardiac Arrest Can Result in Improved Likelihood for Neurologically-Intact Survival. Resuscitation. 2019; 135: 162–7. doi:10.1016/j.resuscitation.2018.11.002
3. Patrick C, Dickson R, Jarvis J. Delayed Sequence Intubation. MCHD Paramedic Podcast. 2018. https://luminarypodcasts.com/listen/mchd-paramedic-podcast-646/mchd-paramedic-podcast/episode-14-delayed-sequence-intubation-dsi-with-dr-jeff-jarvis/bf811c1b-3b40-4835-8474-5b74662da9b4?country=US
4. Goyal S, Agrawal A. Ketamine in status asthmaticus: A review. Indian J Crit Care Med. 2013; 17(3): 154–61. Doi: 10.4103/0972-5229.117048
Daisy Ryan, MD, is a resident at HCA Houston Healthcare in Kingwood, Texas.
Lillian Trosclair, LP, is licensed paramedic in charge at Montgomery County Hospital District EMS in Conroe, Texas.
James Seek, LP, BAAS, is division chief of Montgomery County Hospital District EMS’s clinical department.
Casey Patrick, MD, is medical director for Harris County ESD 11 Mobile Healthcare and assistant medical director for the Montgomery County Hospital District EMS in Conroe, Texas.
Kevin Crocker, LP, FACPE, is division chief of quality and process improvement for Montgomery County Hospital District EMS.
Robert L. Dickson, MD, FACEP, FAEMS, is EMS medical director at Montgomery County Hospital District (MCHD) EMS and faculty at HCA Houston Healthcare in Kingwood, Texas.