



Discipline in EMS: Set Up for Success

In your office one morning, you receive an e-mail from the local hospital with a complaint about one of your field personnel. The e-mail alleges a serious infraction—one that needs to be addressed. You look to your organization’s policy manual for disciplinary guidance, but there is no policy that determines the severity or lays out a process. You have no policy that allows for progressive discipline. This leaves you no choice but to administer discipline with no plan or process for consistency.
Unfortunately, this is the case for many EMS services.
The first question you should ask for any discipline is simple: Did we set the employee up for failure? The second: Did we fail to explain the policies and discipline well enough for the employees to understand? If you answer yes to either question at any point enforcing your discipline policy, it may be time for an update.
What does discipline really mean? Well, it’s the expectation of the organization—not the punishment. You set policies to create a disciplined organization. The policy is the process by which you get to that type of department you want to be. Most policies can be described in a page or two with general terms and statements, but all should be detailed and clearly laid out. When building a discipline policy, you have to be clear about expectations and the process for progressive discipline.
Clarifying Statements
We created a discipline policy for our organization, Nevada’s Humboldt General Hospital EMS, that consists of several parts. The first is the clarifying page. It lays out many specific topics, including when and how the policy will be enforced:
This disciplinary policy is to be used as a guide to discipline an employee and is to be applied while in the stations, on calls, in the hospital or community setting, or any other time the employee is under the auspices of the EMS department.
This statement allows for a far-reaching policy focused on any time the employee is fulfilling job requirements as an official employee.
A major component of any disciplinary policy is the expectations you set for employees and why a discipline policy is required. This can be laid out in a simple statement. Our way of accomplishing this is the following:
An employee failing to adhere to the polices set forth by the department violates the community’s trust. For EMS professionals this violates the standards of moral and ethical conduct established by our profession. More importantly, it violates the trust developed between patients, our partners, and us.
This statement clearly lays out that professional behavior is required by the department and the profession. It is our belief that to be successful in this career, staff members with integrity and who hold themselves to a higher standard is a must.
We also have the ability to elevate discipline based on investigation and evidence it obtains. This allows some flexibility on the part of the EMS chief/director to increase the punishment if multiple infractions occur or there is a patient safety issue. That is achieved with a simple statement in the first section of the policy:
In case of serious misconduct, the EMS chief/director may bypass the verbal and/or written warning process and suspend the individual from the EMS system immediately or terminate if deemed necessary.
Discipline Matrix
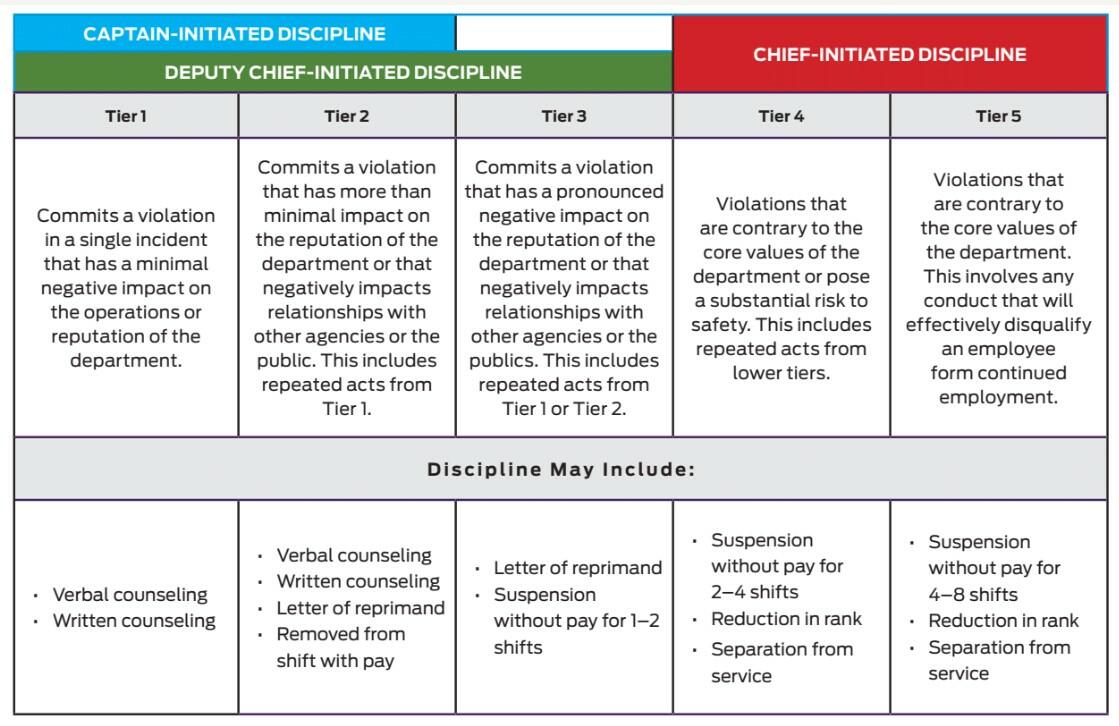
The purpose of the policy is to serve as a resource to help guide discipline decisions. But its overall goal is to communicate expected behavior and the consequences for not following it, with a large focus on training, leading, coaching, and encouraging. This focus allows for small infractions to be corrected before larger ones become an issue. We achieve this by use of a discipline matrix (Table 1).
The matrix allows us to break down who initiates the discipline and what levels can be implemented. We break down infractions into tiers, which are then further defined by specific offenses. In the Tier 1 and 2 sections, discipline begins with street-level supervision—they can issue a verbal or written warning as soon as an infraction occurs for such offenses. This discipline is designed to be handled immediately and used as a counseling session to alter employee behavior. Tier 2 infractions have more progressive discipline attached, including letters of reprimand and being removed from a shift with pay.
The verbal counseling is a process of notification to the employee that an infraction occurred and needs to be corrected. Written counseling is the process of formally documenting that an infraction occurred and needs to be corrected. The letter of reprimand is a formal document that requires immediate change in behavior/actions to correct infractions.
Tier 3 offenses are immediately elevated to the senior leadership team. These involve more egregious behaviors or actions. This tier allows for suspension of 1–2 shifts or issuing a letter of reprimand. This policy also requires each incident to be handled on a case-by-case basis. Any case can be elevated to a higher tier based on circumstances, severity, and the results of investigation by staff. Each offense will also bring a probationary period lasting 6 months, 12 months, or indefinitely. This is determined by the severity of the infraction and history of the employee.
Tier 4 and 5 offenses are directed to the EMS chief/director, and discipline is initiated within his/her office. The investigation can be coordinated by other senior administrators, but the discipline and final counseling will be handled at the top level. These offenses represent the most serious infractions: ones tied to patient, crew, or personal safety, as well as any behavior that reflects poorly on the EMS system or department.
Each infraction is thoroughly reviewed, and in the case of Tier 4 or 5 offenses, no discipline is administered until all parties are interviewed and an investigation is conducted. These cases are very limited but can cause the most liability or strain on a department. They need to be handled carefully, with proper documentation. Most of these cases will need human resources involvement.
Tier System
These are the categories and specific infractions. They include:
Tier 1 Infractions:
- Nonobservance of the dress code and required personal grooming standards.
- Failure to follow chain of command or a direct order from a superior.
- Failure to act in a professional manner or any conduct deemed unacceptable or inappropriate to good order and discipline.
- Smoking, chewing tobacco, or using a vape device while in the station, unit, hospital, or on any emergency or nonemergency call.
- Disrespectful interaction with any other employees, patients, administrators, and/or staff.
- Failure to abide by the cell phone/camera policy.
- Obtaining or attempting to obtain any benefit to which the employee is not otherwise entitled by duress, coercion, fraud, or misrepresentation.
- Failure to act in a professional, reasonable, prudent, or courteous manner, or otherwise engaging in activities that reflect poorly on the department or EMS profession.
- Conduct that causes distraction to others or behavior that disrupts the department and/or other employees.
- Failure to meet education and training requirements.
- Failure to perform standard or assigned operational duties.
- Damage to property.
Tier 2 Infractions:
- Performing duties and/or skills outside the scope of practice.
- Removal from a shift at the request of a captain due to affective or behavior issues.
- Wearing your uniform while drinking or purchasing alcohol or participating in any other inappropriate behavior.
- Behavior deemed inappropriate by any captain, administrator, or chief.
- Failure to notify administration of any status change in licensure.
- Unauthorized use of department property, unauthorized presence or use of facilities/property, misuse of emergency equipment, and/or illegal use of a computer.
- Performing skills on which the employee has not yet been designated competent and signed off by an administrator.
- Conduct or attributes that cause distraction to others or detract from the effectiveness of the environment.
- Multiple violations of the dress code policy.
- A pattern of excessive absenteeism or tardiness.
- Disregarding safety or security regulations.
- Failure to report damage to department property.
Tier 3 Infractions:
- Abandoning or neglecting a patient requiring emergency care.
- Use of inappropriate, indecent, and/or obscene language; use of any lewd, racial, ethnic, or sexual statement or innuendo; indecent gestures or conduct.
- Violating any rule or standard that may jeopardize or create a negative effect on the health or safety of a patient or crew member.
- Behavior with intent to detract, disrupt, endanger, or harass another employee and/or failure to report an employee who knowingly helps or is present when another employee violates behavior standards.
- Lying, cheating, or other acts of dishonesty.
- Hazing and/or bullying.
- Being charged with a crime while employed or failure to notify the chief with in 72 hours of any arrest.
- Failure to maintain confidentiality of information regarding patient care or other events; failure to comply with the Health Information Portability and Accountability Act (HIPAA).
- Misuse of department property to include intentional damage or destruction of property.
- Insubordination.
- Failure to comply with lawful instructions, orders, or directions given by administration.
- Behavior deemed inappropriate by any captain, administrator, or chief.
Tier 4 Infractions:
- Unauthorized use or removal of narcotics, drugs, supplies, or equipment from any ambulance, healthcare facility, or other workplace location.
- Possession of any guns or other lethal weapons while in the auspices of the department, unless authorized by the chief.
- Any intentional falsification or invention of data or information in a clinical setting. Examples include inventing, altering, or falsifying patient data for a run report; submitting information as your own when someone else completed or created the information; communicating false, altered, or incomplete information around clinical care and/or documentation.
- Conduct that threatens or endangers the health or safety of others, assault, threat, extortion, and physical altercation (fighting).
- Violation of the laws of the state or its rules and regulations pertaining to EMS personnel.
- Sexual misconduct, including sexual harassment, sexual assault, obscene or offensive jokes or gestures, or inappropriate touching.
- Using or being under the influence of, possessing, or distributing alcohol or illegal drugs during any phase of employment.
- Stealing, including appropriating or possessing without authorization medications, supplies, equipment, or personal items from HGH, the EMS department or affiliate, or any employee or patient.
- Behavior and/or actions deemed unprofessional or that detract from the ability to perform duties.
- Behavior deemed inappropriate by any captain, administrator, or chief.
- Discrimination on the basis of national origin, race, color, creed, religion, gender, gender orientation, age, disability, or economic status while engaging in activities related to the department.
- Abandonment of a patient and/or committing gross negligence.
Tier 5 Infractions:
- Multiple violations of lesser tiers or policies.
- Any violation of the lower tiers that results a safety issue that affects patients, crew members, hospital staff, or the public.
- Any violation of the lower tiers that results in a trust issue within the organization.
- Any violation deemed detrimental to the organization.
- Behavior deemed inappropriate by an administrator and/or chief.
Documentation
No discipline policy is complete without a thorough process of documentation. We release all documentation to the employee, except statements from other employees, patients, or witnesses. This is to protect the reporting parties and witnesses. Sharing other documentation is necessary so the employee knows they were treated fairly and a thorough investigation was performed.
The process starts with filling out a discipline packet that includes a checklist (to verify everything is completed), a timeline of the incident, the outcome form, a copy of the policy or protocol violated, recommendation from street-level supervision, any documentation (e-mails, mail, etc.), employee/witness statements, any minutes from meetings, and verification that the chief/director was notified. There is a lot to document, but this can be completed in less than an hour and is vital to performing a thorough investigation.
The counseling form is a simple document that allows for a description of the infraction, its nature, and a follow-up plan. This is signed by all parties. The timeline lays out the time and date of the event. It also allows for a description of the events leading up to the infraction, following the infraction, and notes from the reporting party. The final outcome form lays out the discipline received and probationary period attached. These forms are used with each infraction, no matter how big or small. This allows for consistency and fairness to all employees.
Conclusion
Discipline is the hardest task administrators handle. It also comes with the most scrutiny. Having a clear and decisive plan laid out in advance makes the difficult task of disciplining your employees more manageable.
Our plan fits our experiences and employees. Each department has to determine what discipline levels or tiers it requires to successfully achieve a disciplined organization. The goal is to train, lead, coach, encourage, and communicate behavior and the consequences. This allows for employees to receive progressive discipline and have a clear process to avoid discipline altogether.
Drew Hooker, MPA, CEMSO, CCPM, NRP, PD, IC, is a 20-year veteran of EMS and has focused on progressive medicine, quality EMS education, and elevating EMS nationally. He has background in operations, education, and administration and is a national and regional speaker on a variety of topics in EMS.
Kevin Grannis, AAS, CCEMT-P, NRP, has been in the emergency services for 14 years in roles from an entry-level first responder and volunteer firefighter in Northern California to his current role as a paramedic supervisor with Humboldt General Hospital EMS in Winnemucca, Nev.







