



Fluid Therapy in Pediatric Septic Shock: Another Challenge for the 2020 PALS Guidelines

A February 2021 editorial on the 2020 Pediatric Advanced Life Support (PALS) guidelines by Peter Antevy, MD, challenged the applicability of the data behind two of the updates, as well as their physiologic basis.1 Sepsis Awareness Month in September highlighted the need for a critical review of the updated PALS recommendations on fluid resuscitation for sepsis.
The 2020 PALS updates provide helpful guidance for EMS professionals on a variety of time-sensitive interventions for children in prearrest, intra-arrest, and postarrest states.2 While the primary focus of these guidelines is the management of cardiac arrest, septic shock is also included as a condition that may progress to cardiac arrest and therefore requires early recognition and treatment. The 2020 guidelines highlight fluid resuscitation as a foundation of septic shock management, but the new recommendations have become less specific and lack a sense of urgency, potentially missing an important opportunity to improve our response to this life-threatening condition.
A More Hesitant Approach
Severe sepsis remains a leading cause of childhood morbidity, hospitalization, and death worldwide.3–5 Early sepsis recognition and urgent application of simple interventions can prevent its progression to decompensated shock and cardiovascular collapse.
Fluid resuscitation has been considered the cornerstone of early septic shock management and prioritized in many guidelines and educational curricula, including the American Heart Association’s PALS provider course.6–8 As noted in the recent PALS updates, mortality from pediatric sepsis has declined in parallel with the implementation of guidelines stressing early antibiotic and fluid administration. Numerous studies have documented that earlier recognition and intervention improves patient outcomes and that treatment bundles emphasizing fluid delivery have resulted in decreased morbidity,9–11 mortality,9,10,12–16 and hospital length of stay (LOS).4,8,10-13
In recent years, however, the most basic principle of shock reversal through fluid resuscitation has been called into question. The 2020 PALS updates now join a growing list of other guidelines in adopting a more hesitant approach to fluid administration in septic shock.5,17–19
Previous PALS updates communicated a clear sense of urgency about sepsis resuscitation and provided specific guidance on fluid volume and timing, emphasizing that “institution of effective therapy is a high priority before collapse of blood pressure with concomitant increased risks of morbidity and mortality.”20 The PALS provider manual recommends a 20 mL/kg fluid bolus over five minutes for severe shock with hypovolemia or hypotension, noting that “early recognition and rapid intervention are critical to halting the progression from compensated shock to hypotensive shock to cardiopulmonary failure and cardiac arrest,”7 and cautions providers to “avoid the common errors of inadequate or delayed administration of fluid resuscitation.”21
Whereas previous editions of PALS offered specific direction and timing or volume of fluid in septic shock, the new updates now state it is “reasonable” to administer fluid boluses of 10 or 20 mL/kg.22 This is noted to be a weak recommendation based on limited evidence (2a, C-LD). The studies highlighted as the basis for this change suggest harm from fluid overload, higher fluid volumes, and faster administration rates without providing important context on the research cited. The updated 2020 recommendations therefore cast doubt on the safety of fluid resuscitation directed at early shock reversal and potentially lead to a more hesitant approach to resuscitation of children with septic shock.
This presents a dilemma for EMS professionals, who often encounter a more critically ill population of children with septic shock and who may regard PALS guidelines as definitive guidance for the management of these patients. A recent study in one large U.S. metropolitan area showed children with sepsis arriving to the ED by EMS, vs. with family, were twice as likely to have hypotension and had twice the risk of PICU admission and death.23 Despite this, fewer than 3% of these children received any prehospital fluid.23 Clearly an opportunity exists to improve pediatric sepsis outcomes through earlier treatment in the field.
Interpreting the Trials
What influenced the changes in the 2020 PALS updates? The FEAST (Fluid Expansion as Supportive Therapy) trial, a study of fluid bolus therapy conducted in sub-Saharan Africa, has had a major influence on many recent sepsis guidelines. This trial randomized children with “severe febrile illness” to a 20–40-mL/kg fluid bolus vs. no fluid bolus. Children receiving fluid boluses had mortality of 10% compared to 7% in the no-bolus arm, leading the authors to question the safety of fluid bolus therapy. However, a majority of enrolled children had malaria, many had severe anemia or sickle cell disease, few had bacterial sepsis, and none had access to resources such as ICU care or vasopressors. While FEAST was not a sepsis trial and the PALS authors are careful to note that results of the FEAST trial are not generalizable to children with sepsis in higher-resourced settings, three trials are referenced in the PALS “supportive text” section that appear to raise questions about the safety of fluid resuscitation.24–26 Each of these cites FEAST as a basis.
The first of these trials, conducted by the Alberta Sepsis Network, is provided as evidence that fluid overload can increase morbidity.24 This retrospective study evaluated 44 children with septic shock and found patients who received more than 20 mL/kg during the first two hours of care had increased LOS and ventilator days.
These results should be interpreted with caution based on multiple potential confounders. No propensity matching was used, and patients who received more fluid were sicker and likely received more aggressive intervention. No details were presented on timing and volume of fluid infusion at the outside hospital or prior to diagnosis in the hospital. Fewer than half of patients with septic shock received 20 mL/kg in less than two hours, potentially obscuring the effects of a few patients receiving very large volumes. Last and perhaps most important, no information was included on children who may have responded to fluid resuscitation alone and therefore did not require PICU admission, invasive monitoring, or vasopressors. This study therefore provides little information useful for guiding care in the early minutes of septic shock care and should not be cited as evidence of the harms of excess fluid. It is also important to note that most of the published data on the harms of fluid overload implicate total crystalloid volume delivered over the course of ICU care and not volume received during the initial resuscitation.27–29
A second trial referenced in the supportive text section suggests a larger initial fluid bolus may lead to clinically significant volume overload. The Fluids in Shock (FiSh) pilot trial randomized children with clinical suspicion of infection and signs of shock to receive 10-mL/kg or 20-mL/kg fluid boluses after an initial dose of 20 mL/kg.25 A total of 73 patients were randomized, and of these fewer than 10% had hypotension. Patients in the 20-mL/kg group received more fluid than the 10-mL/kg group over the four-hour study period (27.5 vs. 14.5 mL/kg). There was no difference in mortality, PICU LOS, or hospital LOS. Two patients in the 20-mL/kg group were noted to have clinical signs of fluid overload, but the specific findings were not described. Patients randomized to the 20-mL/kg group were younger and smaller (median age 2 vs. 11 months, median weight 5 vs. 9 kg) and more likely to have bacterial sepsis (50% vs. 31%).
Most interesting, more than 50% of screened children received their first 20 mL/kg of fluid for clinical signs of shock, subsequently improved, and then did not meet enrollment criteria. This study may therefore add helpful guidance regarding fluid bolus size, since 10-mL/kg doses require more frequent patient reassessment, but it does not provide evidence that higher initial volumes of fluid lead to clinically significant fluid overload. This study in fact suggests that most children with signs of shock benefited from early resuscitation with 20 mL/kg of fluid and as a result did not require additional therapy.
Lastly, the PALS guidelines cite as evidence a trial by Indian pediatrician Jhuma Sankar, et al., suggesting faster resuscitation may lead to fluid overload and worse outcomes.26 In this study of children in India presenting with suspected septic shock, resident physicians were assigned to deliver 40–60 mL/kg given in 20-mL/kg doses over 5–10 minutes vs. 15–20 minutes. More children in the faster bolus arm met the primary endpoint of “need for mechanical ventilation,” an intervention for which the authors admitted having a low threshold and the application of which was likely highly subjective. In addition, high-flow nasal cannula or other forms of noninvasive ventilation were apparently not considered as alternatives to endotracheal intubation. The authors said they “used similar volumes (up to 60 mL/kg) in both groups to adhere to the guidelines, as well as to ensure similar volumes in both groups so the results were comparable.” This suggests that clinical markers of response after each bolus were not used to guide therapy. Lastly, this study actually demonstrated a trend toward decreased mortality in children who received fluids more rapidly. A helpful editorial on this study outlines other methodologic problems.30
These references remind us that patients presenting with shock require constant reassessment after each bolus of fluid. However, none of these studies provides evidence that the possible harms of fluid resuscitation outweigh the benefits of 10–20-mL/kg doses of fluid for septic shock. The softening of the language on fluid delivery in the updated guidelines, combined with subsequent text suggesting potential harm, may lead prehospital professionals treating children with shock to question whether delivering a fluid bolus is the right approach. This is further complicated by the absence of specific language on the urgency of treating decompensated shock.
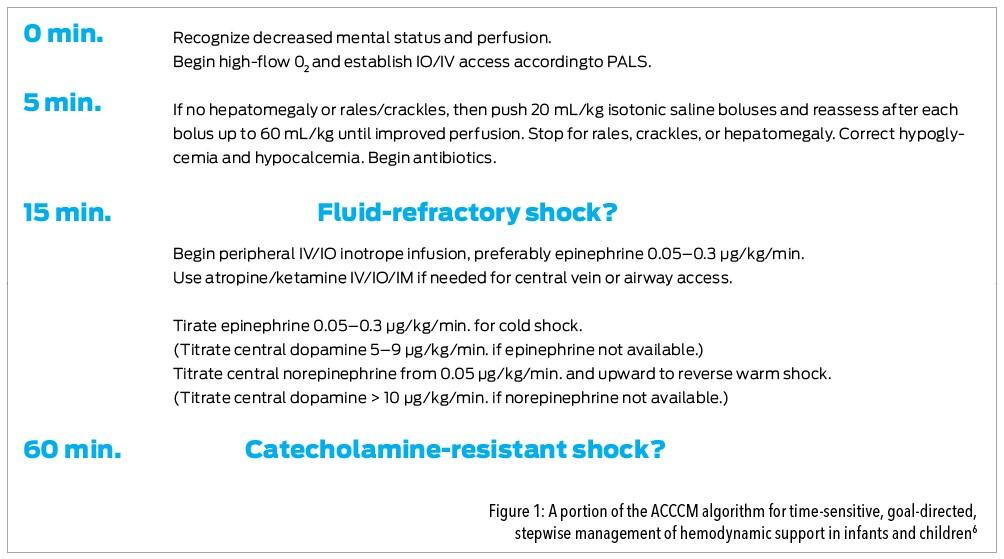
Thankfully the 2020 PALS provider manual continues to communicate urgency, advocating 20-mL/kg boluses given over 5–10 minutes and titrated to shock reversal.21 This is also consistent with the European Resuscitation Council and American College of Critical Care Medicine guidelines, which suggest 20-mL/kg fluid boluses, up to 40–60 mL/kg for children with signs of inadequate perfusion (Figure 1).6,31 The new Surviving Sepsis Campaign (SSC) guidelines similarly recommend 10–20-mL/kg boluses of fluid up to 40–60 mL/kg, with attentive reassessment after each bolus.
Unfortunately, based largely on the FEAST trial, the SSC authors also suggest that in clinical settings without access to intensive care, a fluid bolus only be given to children with hypotension.5 Adding to the uncertainly created by the PALS updates, the SCC guidelines do not address whether EMS professionals are considered to have access to intensive care.
Conclusion
As one of the most recognized and respected authorities on the early management of critical illness in children, the American Heart Association, through the PALS guidelines and PALS provider course, has the opportunity to provide clear and actionable advice for clinicians. On the important topic of septic shock resuscitation, the PALS authors could provide more-specific suggestions on the timing, speed, and volume of resuscitation, while acknowledging these will all vary depending on patient condition and that precise guidance will likely remain a matter of controversy for some time.
None of the available literature appears to provide sufficient basis for changing recommendations on fluid resuscitation.
References
1. Antevy P. Two Issues With the New PALS Guidelines. EMS World, 2021 Feb; www.hmpgloballearningnetwork.com/site/emsworld/article/1225297/resident-eagle-two-issues-new-pals-guidelines.
2. Topjian AA, Raymond TT, Atkins D, et al. Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 2020 Oct 20; 142(16_suppl_2): S469–S523.
3. Weiss SL, Balamuth F, Hensley J, et al. The epidemiology of hospital death following pediatric severe sepsis: when, why, and how children with sepsis die. Pediatr Crit Care Med, 2017; 18(9): 823–30.
4. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet, 2020; 395(10,219): 200–11.
5. Weiss SL, Peters MJ, Alhazzani W, et al. Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Intensive Care Med, 2020; 46(Suppl 1): 10–67.
6. Davis AL, Carcillo JA, Aneja RK, et al. The American College of Critical Care Medicine Clinical Practice Parameters for Hemodynamic Support of Pediatric and Neonatal Septic Shock: Executive Summary. Pediatr Crit Care Med, 2017; 18(9): 884–90.
7. American Heart Association. Pediatric Advanced Life Support (PALS) Provider Manual. Dallas, Tex.: American Heart Association, 2016.
8. American Academy of Pediatrics. APLS: The Pediatric Emergency Medicine Resource, 5th ed. Jones & Bartlett Learning, 2011.
9. Carcillo JA, Kuch BA, Han YY, et al. Mortality and functional morbidity after use of PALS/APLS by community physicians. Pediatrics, 2009; 124(2): 500–8.
10. Balamuth F, Weiss SL, Fitzgerald JC, et al. Protocolized treatment is associated with decreased organ dysfunction in pediatric severe sepsis. Pediatr Crit Care Med, 2016; 17(9): 817–22.
11. Akcan Arikan A, Williams EA, Graf JM, Kennedy CE, Patel B, Cruz AT. Resuscitation bundle in pediatric shock decreases acute kidney injury and improves outcomes. J Pediatr, 2015; 167(6): 1,301–5.
12. Carcillo JA, Davis AL, Zaritsky A. Role of early fluid resuscitation in pediatric septic shock. JAMA, 1991; 266(9): 1,242–5.
13. Han YY, Carcillo JA, Dragotta MA, et al. Early reversal of pediatric-neonatal septic shock by community physicians is associated with improved outcome. Pediatrics, 2003; 112(4): 793–9.
14. Oliveira CF, Nogueira de Sá FR, Oliveira DSF, et al. Time- and fluid-sensitive resuscitation for hemodynamic support of children in septic shock: barriers to the implementation of the American College of Critical Care Medicine/Pediatric Advanced Life Support Guidelines in a pediatric intensive care unit in a developing world. Pediatr Emerg Care, 2008; 24(12): 810–5.
15. Lane RD, Funai T, Reeder R, Larsen GY. High reliability pediatric septic shock quality improvement initiative and decreasing mortality. Pediatrics, 2016; 138(4).
16. Evans IVR, Phillips GS, Alpern ER, et al. Association Between the New York Sepsis Care Mandate and In-Hospital Mortality for Pediatric Sepsis. JAMA, 2018;3 20(4): 358–67.
17. Maitland K. Emergency fluid bolus therapy studies: first do no harm. Arch Dis Child, 2019; 104(5): 409–10.
18. NICE. National Institute for Health and Care Excellence: Sepsis: Recognition, Diagnosis and Early Management (NICE Guideline 51); www.nice.org.uk/guidance/ng51.
19. World Health Organization. Guideline: Updates on Paediatric Emergency Triage, Assessment and Treatment: Care of Critically-Ill Children. Geneva: World Health Organization, 2016.
20. de Caen AR, Maconochie IK, Aickin R, et al. Part 6: Pediatric Basic Life Support and Pediatric Advanced Life Support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation, 2015; 132(16 Suppl 1): S177–S203.
21. Op. cit., American Heart Association. Pediatric Advanced Life Support (PALS) Provider Manual.
22. de Caen AR, Berg MD, Chameides L, et al. Part 12: Pediatric Advanced Life Support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 2015; 132(18 Suppl 2): S526–S542.
23. Depinet HE, Eckerle M, Semenova O, Meinzen-Derr J, Babcock L. Characterization of Children with Septic Shock Cared for by Emergency Medical Services. Prehosp Emerg Care, 2019; 23(4): 491–500.
24. van Paridon BM, Sheppard C, G GG, Joffe AR, Alberta Sepsis Network. Timing of antibiotics, volume, and vasoactive infusions in children with sepsis admitted to intensive care. Crit Care, 2015; 19: 293.
25. Inwald DP, Canter R, Woolfall K, et al. Restricted fluid bolus volume in early septic shock: results of the Fluids in Shock pilot trial. Arch Dis Child, 2019; 104(5): 426–31.
26. Sankar J, Ismail J, Sankar MJ, C P S, Meena RS. Fluid Bolus Over 15–20 Versus 5–10 Minutes Each in the First Hour of Resuscitation in Children With Septic Shock: A Randomized Controlled Trial. Pediatr Crit Care Med, 2017; 18(10): e435–e445.
27. Abulebda K, Cvijanovich NZ, Thomas NJ, et al. Post-ICU admission fluid balance and pediatric septic shock outcomes: a risk-stratified analysis. Crit Care Med, 2014; 42(2): 397–403.
28. Alobaidi R, Morgan C, Basu RK, et al. Association Between Fluid Balance and Outcomes in Critically Ill Children: A Systematic Review and Meta-analysis. JAMA Pediatr, 2018; 172(3): 257–68.
29. Al-Lawati ZH, Sur M, Kennedy CE, Akcan Arikan A. Profile of fluid exposure and recognition of fluid overload in critically ill children. Pediatr Crit Care Med, 2020; 21(8): 760–6.
30. Russell MJ, Kanthimathinathan HK. Is There an Optimum Duration of Fluid Bolus in Pediatric Septic Shock? A Critical Appraisal of “Fluid Bolus Over 15–20 Versus 5–10 Minutes Each in the First Hour of Resuscitation in Children With Septic Shock: A Randomized Controlled Trial” by Sankar et al (Pediatr Crit Care Med, 2017; 18: e435–e445). Pediatr Crit Care Med, 2018; 19(4): 369–71.
31. Maconochie IK, Bingham R, Eich C, et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 6. Paediatric life support. Resuscitation, 2015; 95: 223–48.
Mark Piehl, MD, MPH, is a pediatric intensivist and critical care transport medical director with WakeMed Health and Hospitals in Raleigh, N.C. He is co-founder and chief medical officer of 410 Medical in Durham, N.C.







