



Managing Newborns in the Field

EMS field delivery of an infant can be a scary situation for even the most skilled and veteran provider. While most of the time things go as nature intends, there are instances with a need for resuscitation of the freshly birthed neonate.
Every year there are approximately 3.9 million births in the U.S. Approximately 3,500 of these are prehospital births, and even fewer are in the presence of EMS clinicians.1,2 Fortunately most prehospital births are uncomplicated (90%), and the neonate requires minimal intervention to survive and adapt to their new environment.
Delivery of a Newborn
During most regular deliveries there will be minimal need for paramedic intervention. The two most important steps in a normal vaginal delivery are controlling the fetal head as it crowns and stimulating the infant after it has been born.2 But there are approximately 350 prehospital births a year that do not go as planned, with the newborn requiring some degree of resuscitation.1
In 1987 the American Heart Association (AHA) and American Academy of Pediatrics (AAP) collaborated on a program to provide clinicians with guidelines for resuscitation of the neonate, the Neonatal Resuscitation Program (NRP).3 These guidelines have been refined over the years but to this day remain the gold standard for neonatal care.
Many EMS providers feel unfamiliar with immediate newborn or neonatal care. In one study 66% of providers surveyed said they’d never received specific neonatal resuscitation training or had received it more than two years ago.4 In the same survey, only 16% of providers felt comfortable taking care of a patient less than 30 days old. While the overall incidence of high-risk EMS neonatal calls is low, they often have a high risk of life-threatening safety events.5 These include medication administration; resuscitation; clinical procedures; fluid administration; clinical assessment and decision-making; airway management; equipment use; and systems processes.
Each of these can be life-threatening for any patient. It is important that EMS clinicians are well versed in neonatal resuscitation and how it pertains to the EMS environment.
Prehospital Resuscitation
The NRP was originally designed for in-hospital emergencies, with minimal guidance for EMS crews delivering babies outside hospital walls. Thankfully there have been many adaptations over the years that make the guidelines more conducive to the EMS environment. As always, it is important to follow local protocols, and these guidelines often represent well-accepted alternatives to the standard NRP guidelines.
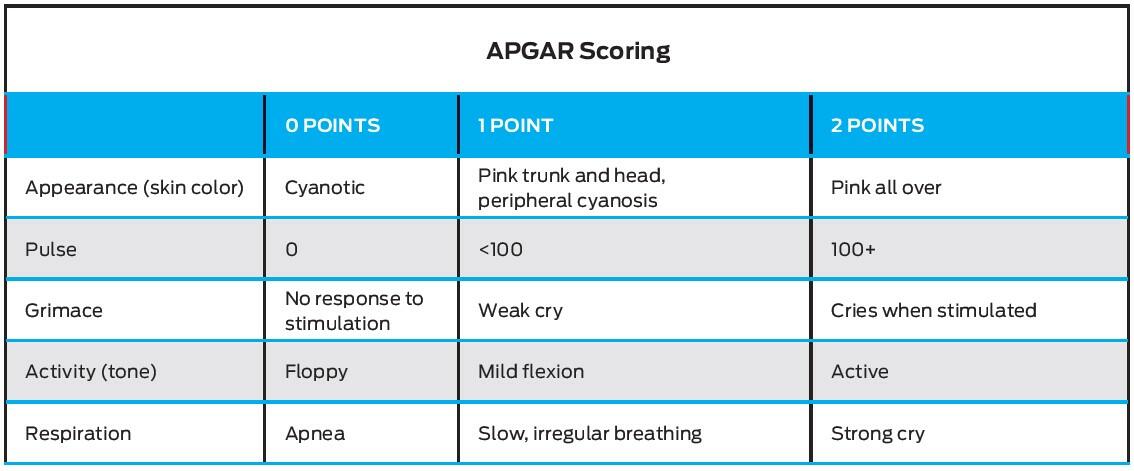
The APGAR score will also provide the EMS clinician with a valuable tool for evaluating neonatal risk.
APGAR scores are taken at one and five minutes of life and are on a 10-point scale based on the infant’s appearance, pulses, grimace, activity (tone), and respiration.6 Infants with one-minute APGAR scores of less than 7 require immediate resuscitation and repeat APGAR scores every five minutes.
Not only are they standard of care, but APGAR scores have been shown to correlate to infant deaths. Researchers have found premature babies with five-minute APGAR scores of 0–3 have a mortality rate of around 31.5%, while for those with scores of 4–6, it’s 7.2%, and for those with scores 7 or greater, just 0.5%. This underscores the need for quality assessment and care for all newborns.7
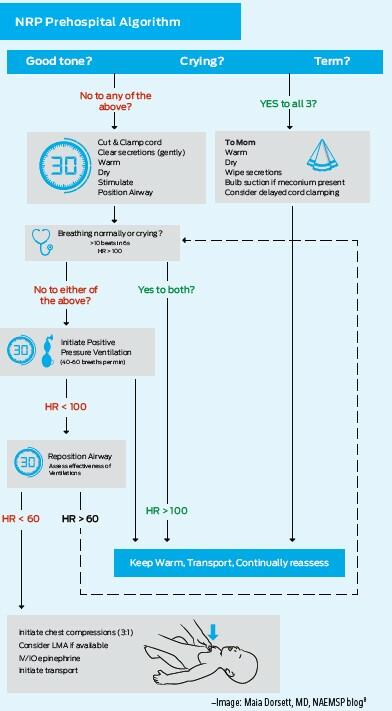
While adaptations exist, NRP is a quality approach.8 At its core it is the rapid assessment and initial treatment algorithm for the neonate. The first few steps are divided into 30-second intervals.
The Evaluation
EMS clinicians should evaluate infants for term birth (more than 37 weeks), their ability to cry, and their overall tone. If these are all good, they should continue standard care, warming, drying, and clearing any secretions that are present. If not, they should clamp and cut the cord, clear secretions, then stimulate, warm, and dry the patient and appropriately position their airway.
Next evaluate breathing and heart rate. The EMS clinician is looking for normal breathing/crying and a heart rate over 100. If these are good, they should continue to monitor, keep the child warm, and transport to an appropriate hospital. If interventions are needed, positive-pressure ventilations are required. Ventilations are performed at a rate of 40–60 per minute for 30 seconds before reevaluation.
If ventilations alone fail to increase the heart rate above 100, reposition the airway and evaluate the effectiveness of ventilations for the next 30 seconds. If this fails and the heart rate drops below 60 bpm, chest compressions are needed. The compression-to-ventilation ratio for NRP is three compressions for every ventilation (3:1). At this point the EMS clinician should evaluate the need for an LMA or ET tube, IV or IO epinephrine, and generally initiate transport.
Be well versed in each of these steps, as the first 90 seconds of care are often crucial in determining the outcome of an infant who requires intervention.
Summary
The need for neonatal resuscitation is generally rare in the field, but if the occasion arises, it can be a high-risk situation. Continue to train and be familiar with these types of situations.
While having certification in NRP is important, it is just as important to understand the adaptations that should be made for EMS field care. Getting help can also require having enough qualified providers for the situation. Remember, there are two patients, as mom still needs care after the baby is born.
It is also important for providers to understand the resources around them, the help they have within their department and surrounding systems, and the capabilities of each hospital in their region. Finally, the provider must decide where to take both patients. Often this is regionalized, but commonly any OB-capable hospital will be able to care for these patients. It is important to transport to a place able to care for both patients, not just one. If resuscitation is required, an OB hospital with a neonatal ICU would be beneficial.
References
1. Huynh T, Bahr N, Harrod T, Guide JM. When Seconds Matter: Neonatal Resuscitation in the Prehospital Setting. Pediatrics, 2020 Jul; 146 (1 Meeting Abstract) 372; https://pediatrics.aappublications.org/content/146/1_MeetingAbstract/372.1.
2. Beaird DT, Ladd M, Kahwaji CI. EMS Prehospital Deliveries. In: StatPearls [Internet]. Treasure Island, Fla.: StatPearls Publishing, 2021.
3. American Academy of Pediatrics. NRP History, https://services.aap.org/en/learning/neonatal-resuscitation-program/nrp-history/.
4. Hlavinka E. EMTs Not Always Familiar With On-Site Newborn Resuscitation. MedPage Today, 2019 Oct 27; www.medpagetoday.com/meetingcoverage/aap/82968.
5. Duby R, Hansen M, Meckler G, et al. Safety Events in High Risk Prehospital Neonatal Calls. Prehosp Emerg Care, 2018; 22(1): 34–40.
6. Simon LV, Hashmi MF, Bragg BN. Apgar Score. In: StatPearls [Internet]. Treasure Island, Fla.: StatPearls Publishing, 2021.
7. Casey BM, McIntire DD, Leveno KJ. The continuing value of the Apgar score for the assessment of newborn infants. New Engl J Med, 2001; 344(7): 467–71.
8. Rayburn D. Here Comes The Baby! Out Of Hospital Principles In Neonatal Resuscitation. NAEMSP Blog, 2020 Jun 24; www.naemsp-blog.com/emsmed/2020/6/24/here-comes-the-baby-out-of-hospital-principles-in-neonatal-resuscitation.
David Wright, MS, PA-C, NRP, is a physician assistant working in the Division of Pediatric Emergency Medicine at Washington University in St. Louis.







