



PCRF 2021 Research Abstracts
Established in 1992, the Prehospital Care Research Forum (PCRF) is dedicated to the promotion, creation, and dissemination of prehospital research. Through our ongoing partnership with EMS World, we are proud to feature selected abstracts from the International Scientific Symposium, to be held during EMS World Expo, October 4–8, 2021, in Atlanta, Ga.
The PCRF is proud to highlight the work of EMS providers who are advancing the profession with science. We believe it is the responsibility of emergency medical professionals worldwide to practice evidence-based medicine and develop a body of evidence that examines prehospital emergency care.
Each year we make research more accessible and understandable through the publication of these abstracts. We hope you will join us in creating a culture of science in EMS by participating in our symposia, workshops, and monthly journal clubs.
On the second Monday of every month, podcasts facilitated by Dr. Remle Crowe focus on the content of Dr. Tony Fernandez’s PCRF Journal Club/Journal Watch column in EMS World Magazine. On the fourth Friday of every month, sponsored by Fisdap, Dr. Megan Corry focuses on educational research. Register for all podcasts at www.prehospitalcare.org.
We would like to thank our volunteer board of advisors and 42 associates. Without the dedication of these volunteers, none of this would be possible. In addition to the hard work of many people, much of our success can be attributed to the commitment of organizations dedicated to research in prehospital care. I would like to acknowledge our various partners, EMS World, ESO Solutions, FirstWatch, Jones & Bartlett Learning, Fisdap, and the RedFlash Group. The generous support of these fine organizations and our affiliation with the National Association of EMTs are what enable the PCRF to fulfill our mission.
The future of EMS depends on the quality and quantity of research we produce. We invite you to take a stand, conduct research in your community, and submit it in 2022 for the greater benefit of EMS. Our PCRF mentors are standing by to assist you.
Sincerely, David Page, MS, NRP
Director, Prehospital Care Research Forum at UCLA
Clinical Abstracts
Mediating Mental Health Stressors for First Responders Using Therapy Dogs in Gaston County, N.C.: A Feasibility Study
Author: Jessica Ross, MHS, NRP
Associate Author: Elizabeth Tait, PhD
Mental health is an important matter in the prehospital setting. The number of suicides and people presenting with mental health disorders is on the rise in emergency medical services (EMS) and other first-responder agencies, and a high number of EMS personnel are being formally diagnosed with PTSD and/or depression. A majority of first responders have experienced mental health issues related to traumatic events, and an alarming number of them abuse alcohol or other drugs as a result. This paper used survey techniques to examine whether therapy dogs can mediate daily stress in first responders. The results indicated the use of therapy dogs can provide a reduction of stress symptoms among first responders reporting high stress.
Objective: To see if therapy dogs can help mediate daily stress among first responders.
Methods: The methodology for this research was a survey among first responders. Pre- and postsurveys were developed and distributed via e-mail to employees of Gaston County EMS. Both surveys were validated by the Institutional Review Board (IRB). A second component of the methodology was having therapy dogs present at Gaston County EMS weekly during shift changes and professional developments. The postsurvey was e-mailed after the therapy sessions. The data from the pre- and postsurveys were reviewed and analyzed.
Results: The survey results indicated therapy dogs provided a reduction of stress symptoms among first responders. Eighty percent of those who participated had high stress that was reduced in a therapy dog session. In addition, a majority of EMS personnel requested for the dogs to be available daily or weekly.
Conclusion: The hypothesis of this study was to see if utilization of therapy dogs is beneficial and could help mediate first responders’ daily stressors. The results showed that 80% of those who participated had high stress that was reduced in a therapy dog session. The majority of the responders stated they would like to see the dogs daily or weekly.
Secondary Traumatic Stress in Emergency Services Systems (STRESS) Project: Quantifying and Predicting Vicarious Trauma in Emergency Medical Services Personnel
Author: Ginny Renkiewicz, PhD, MHS, Paramedic, FAEMS
Associate Author: Michael W. Hubble, PhD, MBA, NRP
Nearly 500 suicides of EMS and fire personnel have been reported since 9/11/01—a number five times higher than in the preceding 120 years. The presence of stress syndromes, such as vicarious trauma (VT), could be a factor; however, there is a dearth of literature describing these syndromes or contributory factors in EMS professionals.
Objective: To identify the prevalence and predictors of VT in EMS professionals.
Methods: This was a survey study of EMS personnel using one-stage area sampling. Service-area data were provided by nine participating agencies. The survey evaluated the relationship between VT and socioeconomic factors and childhood trauma. The Impact of Event Scale-Revised (IES-R) was used to quantify VT. Univariate analyses used chi-square and ANOVA, as appropriate. Factors significant in the univariate analyses were included in a logistic regression to determine predictors of VT while controlling for potential confounders.
Results: A total of 691 respondents participated in the study, of whom 44.4% were female and 12.3% were minorities. Among all participants, 40.8% had VT. Of those, 52.5% scored high enough to potentially elicit immune responses. Compared to those without VT, more than four times as many EMS professionals with VT self-reported as currently in counseling (9.2% vs. 2.2%; p<0.01). One in four EMS professionals (24.0%) had considered suicide, while nearly half (45.0%) knew an EMS provider who had committed suicide. There were multiple predictors of VT, including female sex (OR=1.55; p=0.02) and childhood exposure to emotional neglect (OR=2.31; p<0.01) or domestic violence (OR=1.91; p=0.05). EMS professionals earning $40,000 to $60,000 annually were five times more likely to have VT (>$100,000=referent). Those with other stress syndromes, such as burnout or compassion fatigue, were 2.1 and 4.3 times more likely to have VT, respectively.
Conclusion: Among study participants, 41% suffered from VT, and 24% had considered suicide. Female sex, income level of $40,000–$60,000, childhood emotional neglect or exposure to domestic violence, and having burnout or compassion fatigue were all predictive of VT. As a largely understudied phenomenon in EMS professionals, additional research on VT should focus on causality and the mitigation of critical stress events experienced by EMS providers in the workplace.
Secondary Traumatic Stress in Emergency Services Systems (STRESS) Project: Quantifying the Effect of Personal Trauma Profiles on Lifetime Prevalence of Suicidality in Emergency Medical Services Personnel
Author: Ginny Renkiewicz, PhD, MHS, Paramedic, FAEMS
Associate Author: Michael W. Hubble, PhD, MBA, NRP
Since the terrorist attacks of September 11, 2001, there have been over 400 suicides of public safety personnel—a 500% increase from preceding years. The cause of this phenomenon is unknown, but it is possible there is a confluence of factors that contribute to suicidality in emergency medical services personnel.
Objective: To identify personal trauma histories and predictors of suicidality in EMS personnel.
Methods: This was a prospective cross-sectional survey study of EMS personnel with IRB approval. Nine EMS agencies were selected to participate based on geographic area and population; they then provided data about their annual call volume and mix. Respondents completed a survey during monthly training that included sociodemographic, employment, and military factors. Additionally, adversity in childhood and potentially traumatic experiences (PTEs) were evaluated using the Adverse Childhood Experience (ACE) questionnaire and the Life Events Checklist DSM-V (LEC-5), respectively. Categorical and continuous variables were analyzed with parametric or nonparametric testing as appropriate. Using factors significant in the univariate analyses, a logistic regression was conducted to determine predictors of suicidality while controlling for potential confounders.
Results: A total of 768 EMS providers participated in this study: 56.1% were male, 12.6% were minorities, 72.8% were paramedics, and 80.4% worked full-time. Nearly 1 in 4 EMS providers (24.4%) had considered suicide. Approximately two times as many had a prior history of counseling for a stress-related event, and 1.5 times as many identified as currently in counseling. Suicidality was two times more likely in EMS providers with prior military service (OR=2.15, p=0.011) and five times more likely in EMS providers who identified as sexual minorities (i.e., nonheterosexual; OR=5.00, p=0.008). Childhood trauma predictive of suicidality included emotional abuse (OR=3.31, p<0.001); emotional neglect (OR=2.19, p=0.015); physical neglect (OR=2.77, p=0.025); and exposure to depression, suicide, or other mental illness (OR=2.15, p=0.010). The presence of burnout was also predictive of suicidality (OR=2.74, p<0.001).
Conclusion: Suicidality is an indisputable concern for the EMS profession and represents a multifaceted issue that needs to be addressed. These findings may prove useful for EMS leaders tasked with interventional strategies for employee wellness and resilience.
An Analysis of Emotional Intelligence in Relation to Turnover Intention Among United States EMTs and Paramedics
Author: Emily Kaplan, MPA, EMTP, CIC, DrPH
Associate Authors: Kenneth A. Knapp, PhD; Peter Ondish, PhD; Celia Sporer, PhD
The demand for emergency medical service professionals is increasing in the face of an unprecedented labor shortage and increasing voluntary turnover. Few studies have explored affective factors, including the trait of emotional intelligence, relating to turnover intention among EMTs and paramedics. Key questions concern 1) the degree to which the trait (EI) is predictive of turnover intention while controlling for other established predictors and 2) the extent to which the impact of EI is mediated by other well-known predictors of turnover intention, including stress and mental and physical health.
Objective: To examine whether emotional intelligence is related to turnover intention among EMTs and paramedics.
Methods: A convenience sample (n=446) was obtained through an online survey based on validated EI, turnover, stress, and other instruments that was created and distributed to EMS providers via agencies and online forums. Analytic methods included t-tests, Pearson correlations, linear regression, mediation, and moderation analysis.
Results: Higher EI was found to result in decreased turnover intention both at the global (r=[−0.31], p<0.001) and factor levels (well-being: r=[−0.22], p <0.001; self-control: r=[−0.19], p<0.001; emotionality, r=[−0.35], p<0.001; sociability, r=[−0.17], p<0.001). Findings from linear regression suggest that although EI has a relationship with turnover intention, variables other than EI may be better predictors of turnover intention. The relationship between EI and turnover intention was found, in mediation analysis, to occur both through perceived stress, (−0.69)(0.26)=(−0.18), and the emotional exhaustion component of occupational burnout (−0.49)(0.57)=(−0.28). EI was not found to buffer the relationship between perceived stress and turnover intention.
Conclusion: The most important implication of this study is that EI should be included in discussions of job turnover of EMTs and paramedics, such as for human resource planning. In addition, the mental and physical health of EMS providers deserves close attention by researchers, policy-makers, and human resource managers.
Paramedic Perceptions of Health
Author: Nathan Malek, CFRN, CTRN, NRP
Associate Authors: Rich Hardy, EdD, LAT; Jefferson C. Brand, MD; Emily Monroe, JM, MD; Heather Peters, PhD; Engin Sungur, PhD
Little reported research exists that analyzes how perception of health affects the mental well-being of EMT-Ps. We evaluated how EMT-Ps perceive their overall health and how perception of health relates to stress, anxiety, and self-efficacy.
Methods: Ground EMT-Ps who worked a minimum of 35 hours a week and were not dual-credentialed from April 21 to June 29, 2017 completed an online survey. The survey consisted of demographic information, the SF-36 Health Survey, the Perceived Stress Scale, the Beck Anxiety Inventory, and the General Self-Efficacy Scale. We surveyed 100 EMT-Ps (67 male, 33 female). Age ranged between 18 and 64 years.
Results: On the SF-36 Health Survey, EMT-Ps scored higher than normative data (p=0.01), indicating they are better able to perform physical activities without limitations due to health. EMT-Ps scored lower on subscales suggesting greater amounts of pain (p=0.04), poorer health (p<0.00), feelings of being more worn out (p<0.00), having more physical or emotional problems that interfere with social activities (p=0.00), experiencing more problems with work or other daily activities because of emotional problems (p>0.00), and having more feelings of nervousness and depression (p=0.00). Our sample reported moderate stress, low anxiety, and high perceptions of self-efficacy. Higher perceptions of health were related to lower perceptions of stress and anxiety and higher perceptions of self-efficacy.
Conclusion: EMT-Ps have low perceptions of overall health, moderate stress perceptions, low anxiety perceptions, and high perceptions of self-efficacy. Higher perceptions of overall health were related to lower perceptions of stress, lower perceptions of anxiety, and higher perceptions of self-efficacy.
A Cross-Sectional Analysis of Organizational Structural Predictors of Ambulance Crashes
Author: Justin Sleffel DHA, Paramedic
The purpose of this study was to investigate the association between three organizational structural factors—organizational type, organizational status (staffing model), and level of service—and ambulance crash rates. The null hypothesis was that there would be no difference in the rate of ambulance crashes during response or transport by any of the three factors studied.
Objective: To investigate the association between three organizational structural factors—organizational type, organizational status (staffing model), and level of service—and ambulance crash rates.
Methods: This study used a cross-sectional design with a sample drawn from the 2019 National EMS Information System (NEMSIS) data set to examine the relationship between these systems-level factors and ambulance crashes. After applying inclusion criteria, a sample of 2,207 cases was drawn and analyzed using the chi-square test of association and multiple logistic regression.
Results: There was a statistically significant but small association between level of service and ambulance crashes during transport, using the chi-square test of association (p<0.05). Emergency medical technician (EMT)-level services had higher crash rates, whereas paramedic-level services had lower rates than expected. There was no statistically significant association between organizational type or organizational staffing model and ambulance crashes during either the response or transport phase of an EMS call, using the chi-square test of association (p>0.05). Likewise, there was no statistically significant relationship between any of the covariates in either of the logistic models performed (p>0.05).
Conclusion: The organizational structural factors examined in this study failed to explain most of the variance in ambulance crash rates. Ambulance crashes are not more or less prevalent in agencies of any particular structure. EMS healthcare administrators and researchers should continue to explore potentially modifiable factors to reduce the incidence of these events and therefore the risk of injury to patients, EMS workers, and the public at large.
Prehospital Trauma Care for Older Patients and Its Association with Patient Outcomes: Aging Challenges and Barriers
Author: Naif Harthi
Associate Authors: Steve Goodacre, MB, ChB, MRCP, DipIMC, FRCEM, MSc, PhD; Fiona Sampson, BA, MSc, PhD; Rayan Alharbi, Dip, BSc, MSc
The use of ambulance services by older patients with injuries is increasing due to impacts of progressive aging changes, leading to adverse patient outcomes. Paramedics end up providing suboptimal care due to these impacts.
Objective: To determine what the published evidence tells us about prehospital trauma care for older patients by examining the extent, range, and nature of this research area and identifying research gaps in the literature.
Methods: A scoping review was conducted guided by the Arksey and O’Malley framework, in line with the PRISMA-ScR checklist. A systematic search was conducted of the Scopus, CINAHL, MEDLINE, PubMed, and Cochrane Library databases to identify articles published between 2001 and 2021. Inclusion and exclusion criteria were applied independently by two reviewers. Data were extracted, charted, and summarized from eligible articles.
Results: A total of 25 studies were included. Five categories were identified: 1) field triage, 2) aging impacts, 3) decision-making, 4) paramedic awareness, and 5) paramedic’s behavior. Undertriage and overtriage and sensitivity and specificity are commonly cited as poorly investigated field-triage subthemes. Aging-related physiologic changes, comorbidities, and polypharmacy were the most commonly researched topics. Inaccurate decision-making and poor early identification of major injuries were cited as influencing patient outcomes.
Conclusion: This is the first study investigating the aging-related challenges that impact prehospital trauma care for older patients and their outcomes. Understanding these challenges can improve meeting the older patients’ needs to ensure positive outcomes. More investigations are required regarding the inadequate knowledge of geriatric care and aging changes with the paramedic’s behaviors in providing limited care.
Research Priorities for Prehospital Care of Older Patients With Injuries: Scoping Review
Author: Naif Harthi
Associate Authors: Steve Goodacre, MB, ChB, MRCP, DipIMC, FRCEM, MSc, PhD; Fiona Sampson, BA, MSc, PhD; Rayan Alharbi, Dip, BSc, MSc
The use of ambulance services by older patients with injuries increases within the impacts of aging-related changes, leading to adverse patient outcomes. There is increasing recognition of the importance of prehospital trauma care for older patients but little systematic research to guide practice.
Objective: To review the published evidence on prehospital trauma care for older patients to determine the scope of existing research and identify research gaps in the literature.
Methods: A systematic scoping review guided by the Arksey and O’Malley framework was conducted in line with the PRISMA-ScR checklist. A systematic search was conducted of the Scopus, CINAHL, MEDLINE, PubMed, and Cochrane Library databases to identify articles published between 2001 and 2021. Inclusion and exclusion criteria were applied independently by two reviewers. Data were extracted, charted, and summarized from eligible articles.
Results: A total of 65 studies were identified and reviewed, and 25 were included. Five categories were identified: 1) field triage, 2) aging impacts, 3) decision-making, 4) paramedic awareness, and 5) paramedic’s behavior. Undertriage and overtriage (sensitivity and specificity) were commonly cited as poorly investigated field-triage subthemes. Aging-related physiologic changes, comorbidities, and polypharmacy were the most widely researched. Inaccurate decision-making and poor early identification of major injuries were identified as potentially influencing patient outcomes. More research is required into paramedic knowledge of geriatric care and aging changes and the potential impact of paramedic care.
Conclusion: This is the first study reviewing the published evidence on prehospital trauma care for older patients and identifying priorities for future research. This review identified the prehospital triage for older trauma victims and studies of paramedic knowledge of older trauma care as key priorities. Investigating and understanding these can improve prehospital care of the older patient with injuries for positive patient outcomes. More research is required into paramedic knowledge of geriatric care and aging changes and the potential impact of paramedic care.
Photodegradation Resistance of Tourniquet Webbings
Author: Leila Danishgar, BS
Associate Authors: Carson Henderson, BS; Marco R. Torres, MD, EMT-P; Juan José Pajuel Castro, ORN
Objective: The purpose of this study was to assess photodegradation rates and resistance of emergency tourniquet webbings with lab-controlled UV light exposure and ultimate tensile strength (UTS) pull testing.
Methods: Two commercial non-pneumatic tourniquets were selected: the North American Rescue LLC CAT Tourniquet Gen 7 (CAT) and the OMNA Inc. Marine Tourniquet Gen 2 (OMT). Five webbing samples of each tourniquet were dissected from whole tourniquets, conditioned per ASTM G-155 protocols, separated into three distinct exposure groups, and placed in a Xenon Arc Chamber for exposure. The groups were the following: control (0 hours of UV exposure), three months (250 hours of UV exposure), and six months (500 hours of UV exposure). Once the exposure time limit was complete, the sample groups were removed from the Xenon test chamber and pull tested to failure to determine UTS, which was measured in pounds per square inch.
Results: The average CAT tourniquet UTS for control samples was 8,820 psi; three months, 7,130 psi; and six months, 1,140 psi. The average OMT tourniquet UTS for control samples was 9,260 psi; three months, 9,040 psi; and six months, 7,810 psi. The mean percentage loss of tensile strength for the CAT tourniquet webbing was −19% at three months and −87% at six months. In contrast, the mean percentage loss of tensile strength for the OMT tourniquet webbing was −2% at three months and −16% at six months.
Conclusion: The OMNA Marine Tourniquet Gen 2 webbing demonstrated significantly more photodegradation resistance and maintenance of tensile strength compared to the CAT Tourniquet Gen 7 webbing.
Sensitivity and Specificity of Emergency Medical Dispatching Protocols in the United States
Author: Christopher Gage, MHS, NRP
Associate Authors: Jackson D. Deziel, PhD, NRP; Denise A. Wilfong, PhD, NRP
Emergency medical services require the accuracy of priority dispatching to optimize the match between patients’ medical needs, prehospital resources, and maintaining patient safety. When ambulances travel with lights/sirens rather than traveling with other vehicles’ flow and speed on the road, they are placing themselves and the public at a higher risk. From 1992–2011, 58% of all injuries and fatalities in ambulances occurred when the ambulance was traveling with lights/sirens.
Objective: To evaluate the sensitivity and specificity of emergency medical dispacth (EMD) protocols in the United States.
Methods: Data were collected from ESO Solutions Inc. (Austin, Tex.). The data were analyzed to determine the sensitivity and specificity of multiple variables when the ambulance was dispatched with lights/sirens compared to no lights/sirens.
Results: The results showed that 87% of all 9-1-1 calls were dispatched with an ambulance using lights/sirens when traveling to the patient, and 86% of the patients transported were transported with no lights/sirens. When comparing the use of lights/sirens upon dispatch to their use during transport, EMDs had a positive predictive value of 15.61% and a negative predictive value of 97.86%. The area under the receiver operating characteristic (ROC) curve was 0.7628. This suggests that EMDs are 76% more likely to dispatch every call with lights/sirens. Regarding the vital signs data, the lights/sirens transport results suggest patients are generally sicker than those without lights/sirens transports.
Conclusion: With a negative predictive value of 97.86%, better dispatching of ambulances needs to be implemented to help reduce the number of deaths and injuries to providers and the public. A secondary triaging system could help reduce the overtriage rate suggested by the results and previous studies. Due to the risk-averse mind-set in the medical field, there is a fear of not responding fast enough. More research needs to be conducted on the use of secondary triaging systems to see if having the caller answer more questions about the patient’s condition might lead to a more accurate response.
Acceptance and Motivations of COVID-19 Vaccination Among Emergency Medical Services Professionals
Author: Nate Andrews, MHA, NRP
Associate Author: Jackson D. Déziel, PhD, MPA, NRP
Widespread vaccination against the SARS-CoV-2 virus is an essential public health component for ending the COVID-19 pandemic. The CDC recommends all persons—especially frontline workers, including emergency medical services professionals—receive a COVID-19 vaccine as soon possible. Data show many healthcare workers are likely to receive the COVID-19 vaccine when offered. However, overall acceptance of the vaccine among EMS professionals is largely unknown.
Objective: To identify the acceptance or deference of the COVID-19 vaccine among EMS professionals, as well as the motivations that influence these decisions.
Methods: A cross-sectional survey was distributed to EMS professionals via electronic mailing lists and social media. Participants responded to questions pertaining to their professional and personal experiences with COVID-19, if they had received the COVID-19 vaccine, and personal motivations behind their decision. Descriptive statistics were calculated, and multivariate logistic regression was used to produce adjusted odds ratios.
Results: A total of 1,087 survey responses were collected, with 70 responses removed from analysis for lack of current EMS employment. Among respondents, 64.7% had received a full COVID-19 vaccine dose, 2.4% had received their first dose, and 32.9% had not received a COVID-19 vaccine. Of those participants who had not received a COVID-19 vaccine (n=318), 81% expressed they are unlikely or very unlikely to receive a vaccine. EMTs were 37% less likely than paramedics to have received the vaccine (OR=0.676, p=0.005). Age and education level were also statistically significant factors for vaccine acceptance. Among participants who received at least one dose of the vaccine, a majority reported (agree or strongly agree) a desire to protect family/friends, self, and patients as primary reasons for receiving the vaccine. A majority of participants who did not receive the vaccine reported a lack of information on the long-term effects of the vaccine, belief the vaccine was developed too quickly, and skepticism in vaccine effectiveness as primary reasons for deferring the vaccine.
Conclusion: Age, education, and certification level are statistically significant factors in COVID-19 vaccine acceptance among EMS professionals. Additional research is needed to identify best practices to combat vaccine hesitancy.
Minimum Vital Sign Set Documentation Among 9-1-1 Patients Not Transported by EMS
Author: Antonio Fernandez, PhD, NRP
Associate Authors: Remle P. Crowe, PhD, NREMT; Scott S. Bourn, PhD, RN; J. Brent Myers, MD, MPH
9-1-1 events that do not result in EMS patient transport represent an important area for safety and liability. Complete patient assessment is critical for informing nontransport decisions.
Objective: To describe documentation of a minimum set of vital signs and associated factors among 9-1-1 events in which the patient was not transported by EMS.
Methods: This retrospective analysis used prehospital records from the ESO Data Collaborative for calendar year 2020. We included 9-1-1 responses for adults (age ≥18 years) not transported by EMS. Nontransports were excluded if the EMS disposition indicated the patient refused evaluation or treatment. A minimum set of vital signs was defined as documentation of heart rate, respiratory rate, and systolic blood pressure. Univariable logistic regression was performed to estimate odds ratios and 95% confidence intervals for minimum vital sign set documentation by patients’ age, sex, race/ethnicity, and community size.
Results: Of 8,296,774 total 9-1-1 events, 11.6% (980,199) involved adult patients not transported by EMS. A minimum set of vital signs was documented for 77.0% (754,787). The median patient age was 54 years (interquartile range: 34–72 years), and 52.3% (738,995) were female. Most patients had race/ethnicity documented as white (64.9%; 579,700). Most responses (80.4%; 787,403) occurred in urban areas. Compared to patients ages 18–30 years, patients in every other decade of life had increased odds of minimum vital sign set documentation, with those age ≥90 having the highest odds (OR=1.12; 95% CI: 1.08–1.16). Odds were decreased for males (OR=0.88; 95% CI: 0.88–0.89). Compared to patients with race/ethnicity categorized as white, Black patients (OR =1.58; 95% CI: 1.56–1.60), Hispanic patients (OR=1.17; 95% CI: 1.14–1.19), and patients categorized as other (OR=1.20; 95% CI: 1.15–1.25) had increased odds. EMS encounters in rural areas saw a 44% reduction in the odds of minimum vital sign set documentation (OR=0.56; 95% CI: 0.55–0.56).
Conclusion: Nearly one in four EMS encounters ending in nontransport did not include documentation of a minimum set of vital signs. Vital signs were recorded less frequently for younger patients, males, and those in rural areas. Further research is needed to determine whether the lack of recorded vital signs reflects actual patient evaluations or inaccurate documentation practices.
Benchmarking Prehospital Customer Satisfaction
Author: Glen Keating, Paramedic, RRT
Associate Authors: Chris Kao, MD; Jordan Rhode, MSHA; Robert Farrell; Jeff Fishel, MSHA; Mike Kozlowski, DO; Ashish Panchal, MD, PhD
Patient experience in healthcare drives a multitude of priorities, ranging from clinical decisions to reimbursement. While widely measured in the in-hospital setting via surveys (e.g., Press Ganey), patient satisfaction is not often measured in the prehospital setting. We hypothesize customer satisfaction will be high but decrease with billing and patient care issues.
Objective: To evaluate customer satisfaction assessments at a suburban third-service EMS agency.
Methods: This study is a cross-sectional evaluation of customer satisfaction surveys received from January to July 2020 at Delaware County EMS, Delaware, Ohio, a suburban third-service EMS agency. Standardized five-part questionnaires were distributed and collected by an EMS survey team, excluding patients with primary impressions related to psychiatric/behavioral disorders, substance use, criminal activity, or death. The following topics were addressed: dispatch team, ambulance experience, EMS professionals, billing, and overall rating. Scores were on a five-point scale. Descriptive statistics were calculated: (median [interquartile range]). Composite scores for EMS professional and overall performance were calculated as a percentage and compared to percentile benchmarks from similar-size and overall EMS agencies.
Results: A total of 421 surveys satisfied inclusion criteria (response rate=24.7%). The median respondent age was 72 (range 61–81 years), and 43% identified as male. Scores for each topic were high: dispatch team (5 [5,5]), ambulance experience (5 [4,5]), EMS professional (5 [5,5]), billing (5 [4,5]), and overall (5 [5,5]). Composite scores for EMS professional and overall performance were high at 94% [100,100] and 93% [100,100], respectively. When benchmarked, the customer satisfaction scores were above the 95th percentile compared to other small-size agencies (EMS professionals: 97th; overall: 96th) and all agencies (EMS professionals: 97th; overall: 96th). Finally, with overall high scores for the agency, we were unable to observe a specific impact from billing or patient care issues.
Conclusion: Customer satisfaction scores are overall high in this EMS agency. The response rate for this customer satisfaction survey was higher than those commonly reported for hospital-based surveys. Further evaluation is needed with multiple agencies in different settings and regions to evaluate the association of billing and patient care issues.
Short-Term Outcomes in Air Medical Trauma Patients Treated With Whole Blood Versus Packed Red Blood Cells
Author: Daniel Davis, MD
Associate Authors: David Olvera, BA, NRP; Leslie M. Brown, BS, NRP, FP-C, TP-C; Kaitlyn Price, BSN, RN, CFRN, TCRN; Laura Smith, BSN, RN, CEN, EMT-P
Many air medical agencies carry packed red blood cells (PRBCs) or whole blood (WB) for administration to trauma victims. Although WB may have hypothetical therapeutic advantages, it is more costly with a shorter shelf-life.
Objective: To compare short-term clinical outcomes for PRBC and WB patients.
Methods: This retrospective cohort analysis enrolled trauma patients administered PRBCs or WB by helicopter crews from 146 bases over 2.5 years (January 2019 through May 2021). Demographics, PRBC/WB administration, and initial/final vitals were abstracted for analysis. PRBC and WB patients were compared with regard to the incidence and reversal of arrest, hypotension (SBP<90 mmHg), abnormal HR (<60 or >100 bpm), and abnormal shock index (SI>1.0). Chi-square was used to calculate odds ratios (statistical significance for p<0.05).
Results: Over the 2.5-year study period, a total of 1,561 patients (1,482 PRBC, 79 WB) were included. As anticipated, scene calls were more common in the WB cohort:
- 69 PRBC patients (5%) and 6 WB patients (8%) presented in cardiac arrest (OR=0.59; p=0.357), with measurable final vitals in 9 PRBC arrest patients (13%) and 0 WB arrest patients (0%) (OR: N/A; p=0.601).
- 543 PRBC patients (38%) and 29 WB patients (37%) had initial hypotension (OR=1.08; p=0.841), with correction in 351 PRBC patients (65%) and 19 WB patients (66%) (OR=0.96; p=0.920).
- 870 PRBC patients (62%) and 50 WB patients (63%) had initial SBP≤90 mmHg (OR=0.93; p=0.841), with 150 PRBC patients (17%) and 10 WB patients (20%) (OR=0.83; p=0.752) having final hypotension. This included arrest in 5 PRBC patients (1%) and 1 WB patient (2%).
- 952 PRBC patients (67%) and 49 WB patients (62%) had initial abnormal HR (OR=1.26; p=0.390), with correction in 243 PRBC patients (26%) and 11 WB patients (22%) (OR=1.18; p=0.752).
- 808 PRBC patients (57%) and 45 WB patients (57%) had initial SI>1.0 (OR=1.01; p=0.920), with correction in 440 PRBC patients (54%) and 22 WB patients (49%) (OR=1.25; p=0.566).
Conclusion: Improvements in vital signs were observed for PRBC and WB. No signal was detected to indicate improved short-term outcomes with WB administration over PRBC. Potential differences may be detected with use of longer-term outcomes.
Prehospital Firearms-Related Injury Descriptives: National Trends
Author: Morgan Anderson, MPH
Associate Authors: Douglas G. Butler Jr., EMT-P; Michael Patoc
Firearm-related injuries are among the five leading causes of death for individuals under the age of 65. Understanding the population most at risk for firearm-related injuries can help aid public health in targeting specific populations with prevention efforts.
Objective: To evaluate the rate of firearm-related prehospital incidents over the last three years among age groups and regions across the United States.
Methods: Retrospective prehospital 9-1-1 responses to firearm-related incidents from 2018 to 2020 were analyzed from the ImageTrend Collaborate database. National EMS Information System Version 3.4 Cause of Injury (eInjury.01), Provider Primary Impression (eSituation.11), and Provider Secondary Impression (eSitutation.12) fields were searched for terms gun or firearm. U.S. regions were identified utilizing the U.S. Census region groups. Chi-square analysis was performed to measure differences from 2018 to 2020.
Results: From 2018 to 2020, a total of 36,454 firearm-related incidents out of 13,259,280 overall incidents involved a 9-1-1 response with patient contact. Most of the firearm-related incidents involved males (90%), Black/African Americans (42%), and the 16–35 age group (57%). Almost 20% of incidents had a fatal pronouncement by EMS services, accounting for 3.8% of all prehospital pronouncements. There was a significant change from 2018 to 2020 (chi-square p<0.01) across all age groups and all regions except the West. There was an overall 37% increase in firearm-related injuries in 2020 compared to 2018. The pediatric age group (0–15 years) saw the largest increase (84%), followed by young adults (16–25 years; 54%). The Midwest saw the largest increase in firearm-related incidents (88%), and the Northeast saw a decrease (26%).
Conclusion: Firearm-related incidents continue to be a major public health problem and have increased drastically over the last three years. Continued evaluation and promotion of firearm prevention policies and strategies across the highest risk age groups and regions is needed. Further research is needed to understand if these injuries are unintentional, self-harm, or assault-related.
Wellness Program Availability and Self-Perceived Support for First Responders in the Rural vs. Urban Work Setting
Author: Morgan Anderson, MPH
Associate Authors: Douglas G. Butler Jr., EMT-P; Michael R. Wilcox, MD
Access to wellness and support programs, including mental health support, may be limited for first responders working in rural communities. Support from coworkers and supervisors has been shown to be protective against work-related stressors.
Objective: To compare access to agency-provided wellness services, self-perceived support from coworkers and supervisors, and stress based on work location (rural vs. urban) for first responders.
Methods: A volunteer-based survey was made available to first responders (EMS and fire) within the United States from 2018 to 2020. Data were analyzed using descriptive statistics to compare first responders working in urban and rural locations. Individuals were asked if they worked in urban, suburban, rural, or wilderness areas. Suburban and urban were combined to create the urban category, and rural was combined with wilderness to create the rural category, based on Census Bureau classification. Pearson chi-square p-values were calculated to identify significant differences in descriptives by work location. Odds ratios and 95% confidence intervals were calculated to describe the association between work location, wellness program availability, and self-perceived support.
Results: There were a total of 649 respondents, with 238 (37%) in the rural setting and 411 (63%) in the urban setting. Reponses indicated a higher proportion of female first responders in rural settings (38%) compared to urban settings (24%). There was no significant difference in job-related stress between urban and rural. Individuals working in rural settings had lower odds of having wellness services provided by their agency (OR=0.61; 95% CI: 1.19–3.82) but had higher odds of feeling fully supported by their supervisor (OR=1.78; 95% CI: 1.11–2.86) and coworkers (OR=2.21; 95% CI: 1.19–3.82).
Conclusion: Within rural locations, agency-provided wellness programs appear to be limited, but coworker and supervisor support networks seem to be robust compared to urban settings. Further research is needed to evaluate education and remote wellness resource opportunities in rural settings.
Prehospital O+ Whole Blood to Enhance Resuscitation (POWER): Are We Targeting the Right Patients?
Author: David Wampler, PhD, LP, FAEMS
Associate Authors: Julien Mapp, MD; Manuel Rayas; Mark Dieterle; David Miramontes, MD; William Bullock; Donald Jenkins, MD; Christopher Winckler, MD
Hemorrhage is a leading cause of potentially preventable death in trauma. Low-titer O+ whole blood (WB) may prevent patients from progressing to hemorrhagic shock. Patients receiving hemostatic resuscitation at the point of injury may prevent irreversible shock. One large urban EMS system has deployed WB to treat patients at risk for needing massive transfusion. Due to clinical, systematic, and logistical complexities, not all eligible patients receive WB therapy.
Objective: To determine if the EMS system’s transfusion criteria are targeting the most severely injured trauma patients.
Methods: This was a retrospective review of all EMS trauma patients transported to a Level 1 trauma center from January 1 to December 31, 2020. Patient EMS electronic medical records were matched with the hospital’s trauma registry (six-element probabilistic matching). Patients were dichotomized to WB or no WB and compared on the following variables: scene time, systolic pressure, heart rate, shock index (SI), injury severity score (ISS), trauma and injury severity score (TRISS), and demographics. Patients with an Abbreviated Injury Score of 6 for the head (fatal head injury) were excluded (n=14). Descriptive statistics and t-test were used for continuous data, and chi-square for categorical data. The significance was p<0.05.
Results: The review included 9,911 trauma patients, and 4,979 (50%) patients were matched to outcomes. The WB group included 265 (5%) patients. WB patients were younger (37+/-15 vs. 46+/-21 years, p=.01) and predominantly male (81% vs. 65%) with a shorter scene time (807+/-463 vs, 1,045+/-502 seconds). All vital signs for patients receiving WB indicated a more critical patient: systolic pressure, 103+/-31 vs. 137+/-29 mmHg; heart rate, 100+/-28 vs. 96+/-23 bpm; SI, 1.08+/-.53 vs. .94+/-.16; TRISS, .718+/-.39 vs. .947+/-.16, and ISS 20.1+/-18.2 vs. 8.9+/-9.3. The mortality rate was 29% on the WB group vs. 4% in the no-WB group. There was an insignificant left-shift of the WB mortality inflection point (sigmoidal curve) when mortality rate was plotted against ISS.
Conclusion: Our transfusion criteria successfully identified a critically ill subset of our regional trauma activations. Further study is needed to determine if prehospital WB transfusion provides clinical benefit to critically ill trauma patients.
Trends in Student Airway Device Placement
Author: Christina M. Keatley, MHS, NRP
Associate Authors: Ron R. Lawler, BUS, NRP; Zachary S. Finn, MD; Robert Gurliacci, BPS, EMT-P; Antonio R. Fernandez, PhD, NRP; Jonathan L. Epstein, MEMS, NRP; Paul Vogt, BAAS; Madison Johnson, BA; Abdulaziz S. Alrubayyi, EMT-P
Objective: To determine whether the frequency, type, and setting of advanced airway placement for adult patients has changed for paramedic students from 2012–2020.
Hypothesis: Over the eight-year study period, it was anticipated that placement frequency of endotracheal intubation (ET) decreased with a rise in placement of supraglottic airway (SGA) devices in all settings (e.g., laboratory, clinical, field).
Methods: This was a retrospective review of student records from Fisdap. Student data were included from all paramedic student accounts from the Core Consortium for Research schools (49 programs) with graduations between January 1, 2012, and December 31, 2020. Records were further limited to those where one of the following airway procedures was recorded: Combitube, digital ETI, EOA/EGTA, ET confirmation of CO2, King LT, LMA, nasotracheal intubation, orotracheal intubation, or where airway management was checked. Descriptive statistics were calculated.
Results: A total of 115,443 paramedic student records were reviewed from 3,606 paramedic students. Throughout the study period there were a total of 2,284 (24.7%) SGA attempts and 6,975 (75.3%) entotracheal intubation (ETI) attempts. From 2015 to 2018 the number of SGAs placed was greater in the clinical setting (2015: 2, 66.7%; 2016: 39, 61.3%; 2017: 176, 61.3%; 2018: 171, 56.3%). The number of SGAs was greater in the lab setting in 2014 (4, 66.7%), 2019 (328, 63.9%), and 2020 (979, 88.1%). There were no ETIs documented in 2012. From 2013 to 2018, the number of ETIs was greater in the clinical setting (2013: 2, 66.7%; 2014: 3, 50.0%; 2015: 11, 57.9%; 2016: 178, 64.0%; 2017: 863, 64.1%; 2018: 720, 59.8%). The number of ETIs was greater in the lab setting in 2019 (1,038, 55.2%) and 2020 (1,880, 84.0%). From 2017 to 2020 the number of ETI attempts increased 66.2%, while the number of SGA attempts increased 287.1%.
Conclusion: Although ETI and SGA placement both increased over the study period, SGA placement increased at a greater rate. Both ETI and SGA transitioned from a majority of attempts in a clinical setting to a majority in a lab setting throughout the study period.
Evaluating Prehospital Point of Care Ultrasound Interpretation Accuracy
Author: Kevin Collopy, MHL, FP-C, NR-P, CMTE
Associate Author: William F. Powers IV, MD, FACS
The Focused Assessment with Sonography for Trauma (FAST) is a rapid bedside examination used to identify patients requiring surgical management for significant bleeding leading to shock.
Objective: To use FAST in the prehospital setting to evaluate its accuracy and potential for patient triage.
Methods: This prospective, observational study analyzed prehospital use of the FAST exam. Airlink and Vitalink providers were equipped with U-lite ultrasound, and paramedics underwent six hours of training prior to use. FAST was performed by paramedics on all eligible patients as part of their secondary assessment. This was compared to FAST performed by the trauma team. The primary outcome was the accuracy of FAST performance by prehospital personnel compared to the trauma team.
Results: A total of 180 patients who underwent prehospital FAST were enrolled in the study. The positive predictive value of the prehospital FAST was 5% (95% CI: 0.02–0.12), and the negative predictive value was 99% (95% CI: 0.94–1.00) for the identification of free abdominal fluid and pericardial tamponade.
Conclusion: Early recognition of life-threatening traumatic injuries utilizing the FAST exam can lead to expedited treatment with massive transfusion protocol and surgical intervention. Although this initial study showed a low positive predictive value for prehospital FAST exam accuracy, further training and practice with the prehospital team could lead to better triage of trauma patients.
The Hemodynamic Impact of Induction with Ketamine vs. Etomidate During Prehospital Rapid Sequence Intubation
Author: Kevin Collopy, MHL, FP-C, NR-P, CMTE
Associate Authors: Carrie Fales, MD; Steven H. Nakajima, PharmD, BCCCP; William F. Powers IV, MD, FACS
When managing critically ill prehospital patients, rapid sequence intubation (RSI) is an essential skill. Ketamine and etomidate are common prehospital induction agents; however, induction agent selection is largely based on provider choice or protocol-driven. The few studies comparing the two drugs have shown no difference in mortality or ICU days. Retrospective studies suggest ketamine may be linked with peri-intubation hypotension and cardiac arrest; however, no studies have prospectively evaluated the hemodynamics of these drugs.
Methods: A prospective study evaluated adult RSI patients between January 1, 2018 and August 31, 2019. Patients were randomized by calendar date and induced for RSI with 0.3 mg/kg IV etomidate on even days and 2 mg/kg IV ketamine on odd days. The primary outcome was the incidence of postintubation hypotension, defined as a 20% decline in systolic blood pressure (SBP). Vital signs were evaluated up to 15 minutes postinduction or until additional sedatives were administered. Secondary outcomes included the absolute change in hemodynamic values, number of intubation attempts, use of vasopressors, time to additional sedatives, and IV fluid (IVF) or blood product administration. Data were analyzed via SPSS.
Results: During the study period, 293 patients underwent prehospital airway management; 98 were excluded because no sedative was used (n=57), age less than 18 years, incorrect drug selection, or missing data. Thus, 195 patients were included in the final analysis (ketamine n=103, etomidate n=92). The study groups had similar age, gender, weight, Glasgow Coma Scale (GCS), initial SBP, and shock index (SI). Indication for RSI was also similar, as were airway problems and complications (p=1.0, p=0.923). First-pass intubation success was 89.2%.
Hypotension occurred in both groups (ketamine, 25.2%; etomidate, 22.8%; p=0.821). Resuscitation with blood or IVF occurred more frequently following ketamine inductions, though neither reached statistical significance (p=0.307, p=0.775). Patients with a high SI (>0.9) who received ketamine had lower SBP 8–15 minutes postintubation (p=0.007). Although ketamine was associated with more hypotension in this subset (26.28% vs. 21.4%), it was not statistically different (p=0.821).
Conclusion: In this trial both ketamine and etomidate were associated with similar rates of postintubation hypotension. Postintubation hypotension was lower following ketamine administration when patients had a high shock index.
A Comparison of Cardiopulmonary Resuscitation (CPR) Outcomes Between Traditional and Endomorphic Manikins With and Without Protective Athletic Equipment
Author: Jennifer Longo, PhD, ATC, NREMT
Associate Authors: Katie J. Lyman, PhD, ATC, NREMT; Thomas A. Hanson, PhD; Gianluca Del Rossi, PhD, ATC; Bryan Christensen, PhD
It is imperative that emergency responders are equipped with the skills and knowledge to determine the best way to care for an equipment-laden athlete suffering from out-of-hospital cardiac arrest (OHCA). Athletes, specifically football players, vary in body composition depending on the demands of their specific position. Furthermore, these athletes utilize protective equipment, which poses an additional barrier to the chest, potentially reducing the quality of chest compressions.
Objective: 1) To investigate emergency responders’ administration of chest compressions on traditional and endomorphic manikins following 2020 AHA CPR Guidelines; 2) to examine emergency responders’ CPR performance over football shoulder pads (FSP).
Methods: Fifty emergency responders completed four two-minute bouts of compression-only CPR. Scenarios included 1) removal of FSP before initiating chest compressions on both traditional and endomorphic manikins and 2) initiating chest compressions over the shoulder pads on both traditional and endomorphic manikins.
Results: There was a statistically significant effect at the 10% level for rate (p=.098) and depth (p=.090) with the presence of FSP. For chest recoil, there was a statistically significant effect due to manikin type (p=.017) and presence of FSP (p=.003). Overall, our findings indicate compression depth is decreased on the endomorphic manikin compared to the traditional manikin, as well as over shoulder pads compared to directly on the chest. It should also be noted that in all conditions compression depth was well below the minimum recommended depth published by the AHA. The average depth on the traditional manikin with no equipment barrier fell nearly 10 mm short of the minimum recommended compression depth.
Conclusion: Providing emergency responders with formal education that includes a variety of external factors, including size of chest and the presence of equipment, is recommended based on the results of this study. Although the LUCAS device has often been cited as a possible mitigation tool for compression issues, the expense of this medical equipment has deterred some services from purchasing. Therefore, it is imperative to consider alternative CPR algorithms based on the circumstance of the OHCA.
Educational Abstracts
These abstracts are presented in partnership with the National Association of EMS Educators.
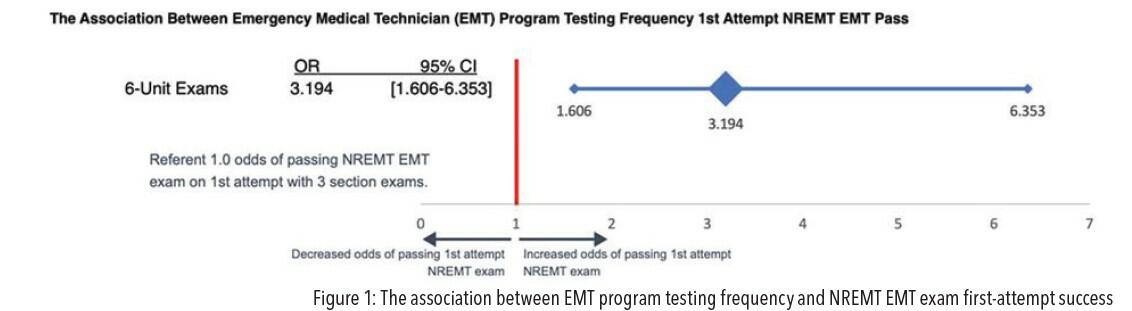
Association Between Emergency Medical Technician (EMT) Program Testing Frequency and NREMT Success
Author: Charles Foat, PhD, NRP
There is wide variation in cognitive testing during EMT programs. Programs should test with adequate frequency to provide students and instructors with indications of the students’ progress. However, it is not known what “sufficient frequency” is.
Objective: To explore the impact of testing frequency (three unit exams and final or six unit exams and final) and first attempt (FA) results on the NREMT exam.
Methods: This study was a retrospective review of prospectively collected EMT program data. Participants were included if they completed an FA NREMT examination for sections ending between January 1, 2018 and May 31, 2021 and were assigned to a class with three or six unit exams. The outcome variable was passing the NREMT exam on the FA. The independent variable was testing frequency. The same instructors taught sections with both three- and six-section exams during the study. The exams had equivalent validity and reliability; however, the three-section exams contained 800 total items, and the six-section exams contained 650 total items.
Results: A total of 296 students met the inclusion criteria. The mean FA pass rate was 82.43% overall. The mean FA pass rate was 75% for classes with three unit exams and 90.55% for classes with six unit exams. Thus, the likelihood of passing the NREMT exam was 3.194 (95% CI: 1.606–6.353) times greater for classes with six unit exams compared to classes with three unit exams.
Conclusion: There was a statistically and practically significant increase in the likelihood of passing the NREMT exam on the FA for EMT classes with six unit exams (see Figure 1).
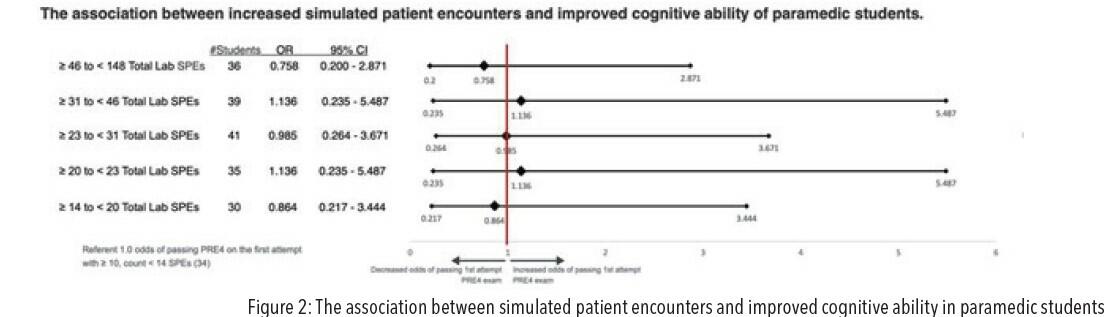
The Association Between Increased Simulated Patient Encounters and Improved Cognitive Ability of Paramedic Students
Author: Charles Foat, PhD, NRP
Associate Authors: Andrea LaLumia, MEd, NRP; David Page, MS, NRP
Previous research has shown that paramedic students (PS) completing more field patient encounters demonstrate improved cognitive ability and first-attempt national exam pass rates (FANEPR). Opportunities for field encounters are variable and challenging to obtain. Simulated patient encounters (SPEs) in the laboratory may be more reliably attainable and produce similar educational outcomes.
Hypothesis: Increased SPEs during PS labs is associated with improved cognitive ability and FANEPR.
Methods: A retrospective analysis of prospectively collected quality assurance data entered by consenting paramedic students in a lab who graduated from programs participating in the Core Consortium for Research in the 2019 calendar year was conducted. Fisdap Paramedic Readiness Exam first-attempt pass rates (FAPR-PRE3/4) were used as a surrogate for first-attempt NREMT pass rates (97% positive predictive value). Only students who documented SPEs in lab using the Fisdap Skills Tracker and attempted the PRE3/4 were included. The outcome variable was FAPR-PRE3/4 performance. The independent variable was the number of SPEs. Chi-square association was used to establish SPE frequency groups.
Results: A total of 148 PS met the inclusion criteria and completed 4,790 SPEs (median=23; IQR 16–36). The mean FAPR-PRE3/4 was 78.4% overall. FAPR-PRE3/4 for PS documenting 46–148 SPEs was 76.9%, vs. 81.5% for PS documenting 10–13 SPEs. PS with more than 46 SPEs showed no significant difference in FAPR-PRE3/4 (OR=0.758; 95% CI: 0.200–2.871). See Figure 2 for complete odds ratios.
Conclusion: Increased PSEs in lab are not associated with improved cognitive ability of PS. Further investigation into the effect of encounter types and leadership roles will improve paramedic education outcomes.
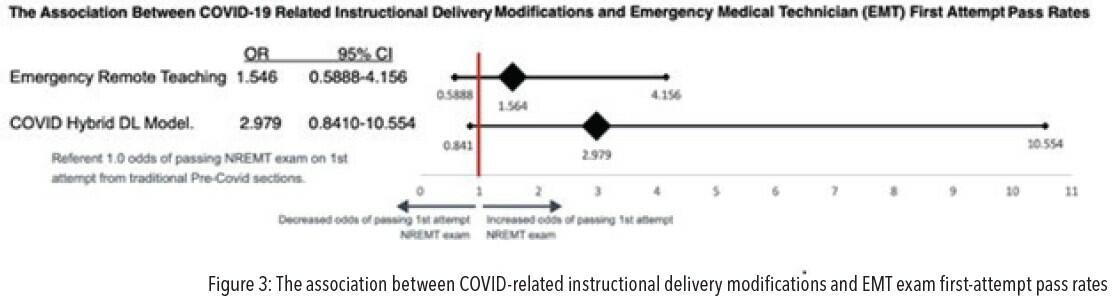
The Association Between COVID-19-Related Instructional Delivery Modifications and Emergency Medical Technician (EMT) First-Attempt Pass Rates
Author: Nicole Hansen, EMT-P, CIC, MEd
Associate Authors: Charles Foat, PhD, NRP; Scott Gann, MS, NRP; Danielle Pettry, PhD, NREMT; Alison Lozeau, MS, NREMT; Robert Rajsky, MSEd, NRP; Andrea Gressens, MHS, NRP; Zeling Yu, BS
When the COVID-19 pandemic caused mandatory shutdowns, many EMS programs were forced to transition from traditional, in-person formats to virtual learning formats. This sentinel event has unearthed concerns regarding the potential adverse effects new learning methods would have on EMT learning outcomes.
Objective: To explore the impact of two instructional models—emergency remote (ER) and COVID distance learning hybrid (DL)—on NREMT certification exam performance.
Methods: A retrospective review of prospectively collected data for a single EMT program. Inclusion criteria included students who completed a first attempt of the NREMT examination for sections ending between July 1, 2019 and December 31, 2020. The outcome variable was passing the NREMT exam on the first attempt. The independent variable was the instructional method: ER or DL. Traditional pre-COVID (TR) was used as the control.
Results: A total of 206 students met the inclusion criteria. The mean first-attempt pass rate was 85.43% overall. The mean first-attempt pass rate TR pre-COVID was 81.73%, 87.5% for ER and 93.02% for DL hybrid. The likelihood of passing the NREMT exam was 1.564 (95% CI: 0.5888–4.156) times greater for students in the ER sections and 2.979 (95% CI: 0.841–10.554) times greater for students in the DL classes compared to the TR sections.
Conclusion: No statistically significant association was found between instructional method and NREMT FA pass rate (see Figure 3). We recommend further investigation into remote learning for EMS education.
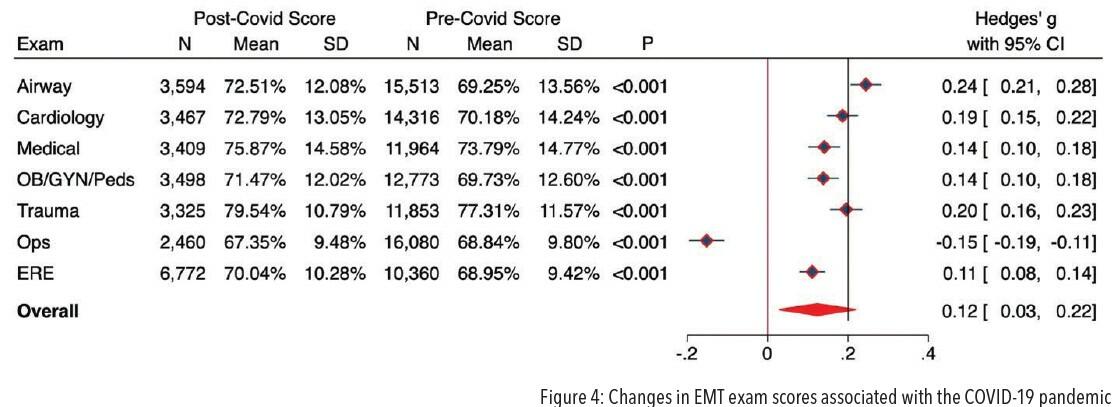
Changes in EMT Exam Scores Associated With the COVID-19 Pandemic
Author: Andrea Gresens, MS, NRP
Associate Authors: Charles Foat, PhD, NRP; Nicole Hansen, MEd, EMT-P; Scott Gann, MS, NRP; Danielle Pettry, PhD, NREMT; Alison Lozeau, MS, NRP; Robert Rajsky, MSEd, NRP; Zeling Yu, BS
The COVID-19 pandemic resulted in changes to methods of instruction and exam proctoring standards in Emergency Medical Technician education programs. Rapid modifications posed increased stress for both instructors and students.
Objective: To explore changes in EMT exam scores that occurred during the COVID-19 pandemic.
Methods: The study was a retrospective review of prospectively collected Fisdap EMT student data. Participants were included if they attempted any Fisdap EMT exams during the study period. EMT Airway, Cardiology, Medical, OB/GYN/Pediatric, Trauma, Operations, and ERE4 exam scores for the pre-COVID period (January 1, 2019 to March 31, 2020) were compared with the during-COVID period (April 1 to December 31, 2020) using inferential statistics to calculate statistical and practical significance.
Results: A total of 19,107 students from 258 programs students met the inclusion criteria. All exam scores showed a statistically significant score difference during COVID, with higher scores for Airway, Cardiology, Medical, OB/GYN/Pediatric, Trauma, and the ERE4 exams and lower scores for the Operations exam. Effect sizes (ES) were calculated to determine the practical significance of the changes in scores; the improvement on the Airway exam met the criteria to be classified as a small ES. Cardiology, Medical, OB/GYN/Pediatric, Trauma, Operations, and the ERE4 exam differences were classified as trivial in terms of practical significance.
Conclusion: Although significant score differences on all EMT exams were observed during COVID, the effect size met the threshold for practical significance on only one (Airway) of the seven exams evaluated (overall ES, g=0.12; 95% CI: 0.03–0.22) (see Figure 4).
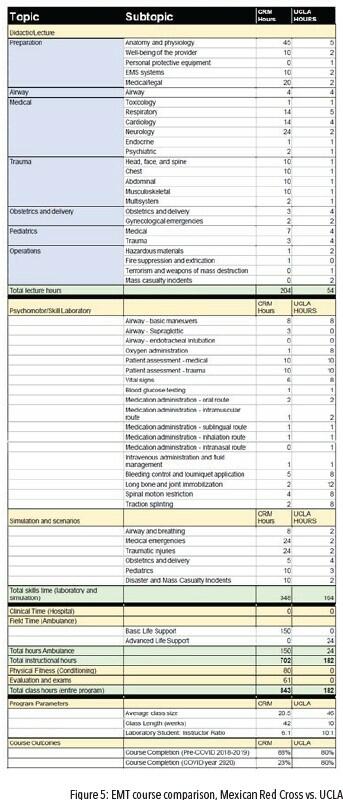
A Comparison of Emergency Changes to Educational Delivery Methods Due to the COVID-19 Pandemic on Emergency Medical Technician (EMT) Student Course Completion Rates
Author: Michael Kaduce, MPS, NRP
Associate Authors: Jeffrey Rollman, MPH, NRP; Em Cyr, BS, EMT; Anthony Keehne, BA, NRP; Ryan Ockey, BS, NRP; Lena Wolter, MA, EMT
The COVID-19 pandemic forced educators to rapidly implement delivery method changes. These changes are marked by many opinions; however, little empirical evidence of student outcomes exists. EMS education programs were similarly affected, with many having to move classes online overnight. It is not known how the shift in delivery method affected EMS student outcomes.
Objective: To compare pre-COVID and during-COVID EMT course completion rates.
Methods: A retrospective analysis was completed of EMT course completion rates in the context of the COVID-19 pandemic, stratified by course delivery method. Both hybrid online and traditional courses were 182 hours, taught by similar educational faculty, and utilized similar policies. The hybrid course was conducted with online, synchronous lectures and on-site skill labs over 10 weeks. The traditional course included on-site lectures and skill labs over four weeks. During the pandemic, all lectures were moved online, and field time was suspended. Pre-COVID courses were from March 2019 to February 2020 and during-COVID courses were from April 2020 to March 2021. Course completion rate was defined as the proportion of students who attempted the first unit exam and subsequently completed all course requirements. Completion rates for each course type were compared using a chi-square test for association between two categorical variables: time (pre-COVID and during COVID) and completion.
Results: In the hybrid course 417 of 558 students (74.7%) successfully completed the course pre-COVID, whereas 322 of 389 students (82.8%) successfully completed the course during COVID, demonstrating a significant increase over time (chi-square=6.50, p=0.01).
In the traditional course, 472 of 574 students (82.2%) successfully completed the course pre-COVID, whereas 276 of 323 students (85.5%) successfully completed the course during COVID, demonstrating a nonsignificant increase over time (chi-square=1.82, p=0.18).
Conclusion: The COVID pandemic’s forced delivery methods did not negatively impact EMT student completion at UCLA. The hybrid course may have been better prepared with technology, instructors familiar with the delivery method, and students expecting the online format to increase completion rates. Study limitations include retrospective data collection limited to UCLA students and inability to collect student demographic factors that could account for outcomes.
A Comparison of Emergency Changes to Educational Delivery Methods Due to the COVID-19 Pandemic on Emergency Medical Technician (EMT) Student Unit Exam Scores
Author: Michael Kaduce, MPS, NRP
Associate Authors: Jeffrey Rollman, MPH, NRP; Em Cyr, BS, EMT; Anthony Keehne, BA, NRP; Ryan Ockey, BS, NRP; Lena Wolter, MA, EMT
The COVID-19 pandemic necessitated rapid changes to educational delivery methods. EMS education programs were also affected and had to move classes online overnight; however, it is unclear how outcomes were impacted.
Objective: To compare pre-COVID and during-COVID unit exam scores.
Methods: A retrospective analysis was completed of EMT unit examination scores in the context of the COVID-19 pandemic, stratified by course delivery method. Both hybrid online and traditional courses were 182 hours, taught by similar faculty, and utilized similar policies. The hybrid course comprised online, synchronous lectures and on-site skill labs over 10 weeks. The traditional course comprised on-site lectures and skill labs. During the pandemic all lectures were moved online, and field time was suspended. Pre-COVID courses were from March 2019 to February 2020, and during-COVID courses were from April 2020 to March 2021. First-attempt exam scores were recorded for EMS operations and airway unit examinations, the first and second exams in the course. Mean test scores for each course type were compared using a Z-score test for two population proportions (pre- and during-COVID populations).
Results: In the hybrid course there was no significant difference between EMS operations pre-COVID (75.4%, n=569) and during COVID (78.6%, n=390; z=[−0.81], p=0.42) or airway score pre-COVID (74.6%, n=532) and during COVID (76.9%, n=384; z=[−1.23], p=0.21).
In the traditional course, there was no significant difference in between EMS operations pre-COVID (79.0%, n=575) and during COVID (80.8%, n=323; z=[−0.63], p=0.53) or airway score pre-COVID (75.4%, n=570) and during COVID (80.3%, n=315; z=[−1.68], p=0.09).
Conclusion: The similar scores on the unit exams support the changes in delivery method. The results suggest health professions students may have been more dedicated to overcoming delivery changes, have similar or more grit, and have similar or greater need to complete the course and join the workforce. Study limitations include retrospective data collection limited to UCLA students and inability to collect student demographic factors that could account for outcomes.
First-Impression Decision-Making Abilities: A Conceptual Model
Author: Jacques Morin, EdD
Orange County Emergency Services (OCES) in North Carolina responds to more than 16,000 9-1-1 calls every year. For each patient OCES EMS providers make first-impression clinical decisions that impact patient outcomes. First-impression clinical decision-making for EMS providers remains an elusive goal. The first-impression process is intended to develop an accurate differential diagnosis, where signs and symptoms of a patient presentation are used to determine an accurate treatment plan.
Objective: To determine how OCES EMS providers make clinical first-impression decisions.
Methods: To understand the decision-making process for EMS providers, four primary research questions were posed for investigation:
- How do providers make a decision?
- What information do providers use to reach a first-impression clinical decision?
- How do providers learn clinical skills?
- How do providers improve their competence?
A convergent mixed-method design was used to collect quantitative survey data using multiple validated instruments. In addition, qualitative data were collected in semistructured interviews to assess decision-making abilities using a framework focused on providers’ instinctual, cognitive, social, and emotional abilities.
Results: Thirty-eight respondents (33 EMS providers and 5 ER physicians) completed the survey. EMS providers reported that they rely on past experiences to decide on first impressions (n=24, 72% agree or strongly agree). EMS providers indicated that the type of call makes a difference in first impression clinical decision making. Studies show shared learning helps clarify the nature of the decision-making problem, but few EMS providers surveyed agreed with this concept (n=12, 36% agree or strongly agree). EMS providers also indicated learning from others is important (n=29, 88% agree or strongly agree) and seeking out clarification when unclear about the information on a call (n=29, 87%, agree or strongly agree).
Conclusion: Conceptual decision-making models should be introduced to EMS providers at OCES during continuing education sessions to support first-impression clinical decision making. Example models include a “hypodeductive reasoning” model when knowledge is sufficient to address a patient presentation or a “rule out worst-case scenario” model when knowledge is lacking.
EMS Clinical First-Impression Impact on Patient Outcomes
Author: Jacques Morin, EdD
Orange County Emergency Services (OCES) in North Carolina responds to more than 16,000 9-1-1 calls every year. For each patient OCES EMS providers make first-impression clinical decisions that impact patient outcomes. This first-impression process is intended to develop an accurate differential diagnosis, where signs and symptoms of a patient presentation are used to determine an accurate treatment plan. Inconsistencies were discovered in how EMS providers use the first-impression codes in patient care records (PCRs). OCES attempted to address the differences and inconsistencies in first impressions with additional training. Repeated training efforts failed to improve the rate of differences and inconsistencies. The assumption was that the paramedics’ competence was responsible for the first-impression inconsistencies.
Objective: To identify reasons for failure of first-impression training efforts.
Methods: OCES’s assessment raised concerns that the training effort was not addressing the root cause of the inconsistencies. In an effort to understand the failure of the training efforts, a clinical decision model that considered a rational multifaceted approach to decision-making was used to develop four primary research questions. A convergent mixed-method design was used to collect quantitative data from more than 12,000 PCRs in 2019 and 2020. First-impression codes were reviewed for agreement using Krippendorf’s alpha reliability coefficient.
Results: Significant differences were found in first-impression coding by providers. OCES has 276 codes for various conditions, symptoms, and events. Fifty-one percent of all first impressions were recorded using 15 of the 276 codes. There was expected agreement in first impressions for conditions such as cardiac arrests (a=1.0, n=23) but a wide range of disagreement for other first impressions, including those noted as “abdominal pain” (a=.1350, n=702) and “no complaint or injury noted” (a=[−.509], n=238), where a reverse relationship was found between providers’ and ER physicians’ clinical impressions.
Conclusion: Providers need a review of the structure and purpose of the coding. Currently, events, symptoms, and diagnoses provide 276 options for providers, creating the opportunity for inaccuracies on first impressions. Incorrect first impressions may lead to improper reference to patient treatment protocols, subsequently impacting patient outcomes.
Building in Bias: Disparities in Paramedic Simulation Training
Author: Sarah Ashton, BS, EMT-B
Associate Authors: Jackson D. Déziel, PhD, MPA, NRP; Kathleen O’Connor, MPP, NRP
Previous research has demonstrated that disparities in care, systemic racism, and gender inequality exist in EMS, education, and the larger healthcare system. Cultural competency and improved training have the potential to reduce these disparities in care. Paramedic education should educate students equitably to care for diverse communities with cultural competence.
Objective: To examine paramedic student educational opportunities and disparities in those opportunities by student race, gender, and ethnicity.
Methods: This was a retrospective analysis of data from paramedic student records from the Fisdap database collected between 2017 and 2019. Descriptive statistics were calculated on 2.8 million student-patient contacts, and multivariate logistic regression was used to produce adjusted odds ratios.
Results: Results of multivariate linear regression models indicated significant differences in the demographics and criticality of patients in simulated vs. clinical settings. Students saw statistically different types of patients depending on their own gender and ethnicity. Students were more than twice as likely to encounter a minority patient in a clinical setting than in simulation. BIPOC (Black, indigenous, and other people of color) and female students were even less likely to encounter a minority patient in simulation. Manikins in simulation were most likely to be critical patients but 77% less likely to represent a minority. Minority students were 42% more likely and females 75% more likely to see a critical patient in the lab compared to their white male counterparts.
Conclusion: Patients presented to paramedic students in laboratory simulation differ significantly from patients they see in the hospital and prehospital setting. There are also disparities between the experiences and opportunities in simulation for minority students. This lack of equity is problematic, especially considering the lack of diversity in EMS. The lack of representation and inequitable experience could potentially build in or exacerbate implicit bias during primary training.
Mental Health Training and Coping Strategies in Paramedic Education: A Narrative Review
Author: Darla Boseman, MHS, NRP, CCEMT-P
Associate Authors: Denise A. Wilfong, PhD, NRP
As part of routine job duties, paramedics are consistently exposed to numerous risk factors that may result in increased incidence of mental health disorders, including post-traumatic stress disorder, depression, and suicidal ideation. As a result, some have demonstrated an inability to maintain their own health and well-being.
Objective: To identify mental health training and coping strategies that could potentially be added to the initial paramedic education curriculum to better prepare graduates for job entry and the stressors they may face in the prehospital setting.
Methods: A search of the literature from 2000 through 2020 was performed utilizing NCBI, Hunter Library Research Guides All-in-One HHS Article Search, and Google Scholar databases. Relevant articles describing mental health and coping strategies were analyzed, exploring opportunities for enhanced initial paramedic education regarding the recognition and reduction of mental health disorders that result from exposures as a part of daily job performance.
Results: Eight publications focusing specifically on the relationship between mental health and coping strategies and prehospital care providers were identified for inclusion. The impact of positive professional and peer support was determined to aid in changing the EMS profession’s culture by normalizing and destigmatizing the expression of emotions and enhancing the recovery process associated with the cumulative effects of distressing and traumatic exposures. Evidence in the articles also highlighted the need for educational change and desire for preventive strategies by both paramedic educators and students.
Conclusion: The stress associated with working in the prehospital setting may have a dramatic impact on the health and well-being of paramedics. By addressing mental health disorders and specific coping strategies not included in initial paramedic education, educators may better prepare new graduates for risk factors associated with the profession and aid in reducing the incidence of these disorders. Further studies are needed to determine specialized educational components that may be added to the paramedic curriculum to prepare students more effectively for recognizing and responding to the risk factors that affect the providers’ mental health and well-being while performing their job duties in the nontraditional prehospital work environment.
Prehospital Provider Attitudes Toward Recognition and Reporting of Child Abuse/Neglect
Author: Makenzie Ferguson, RN
Associate Authors: Shelley Brukman, RN; Kim Zaky, RN; Theodore Heyming, MD
According to the Centers for Disease Control and Prevention, as many as 1 in 7 children are affected by child maltreatment annually. Healthcare providers, including emergency medical service providers, have an ethical and legal obligation to recognize and report abuse. Child abuse screening tools have been successfully adapted for use in the emergency department setting to overcome barriers to recognizing and reporting abuse (Hoft, 2017). Currently there is no known universal tool used by EMS providers to aid in the detection of child abuse.
Objective: To examine EMS attitudes toward child abuse recognition, standard care practices for reporting, and attitudes toward adopting a standardized tool into practice.
Methods: A baseline cross-sectional survey was distributed to 250 EMS providers from three EMS agencies. Elements addressed in the survey included self-reported frequency of the provider caring for abused patients, standard practices when encountering abuse, barriers to recognition/reporting, level of comfort with filing a child abuse report, and provider preferences on having a short screening tool integrated into their electronic patient care report (ePCR). The response rate was 40.4%.
Results: When surveyed most providers indicated that child abuse/neglect occurs in less than 1% of children, grossly underestimating the number of children that experience abuse/neglect. Over 90% of participants reported they did not file a child abuse report or relay suspicion of abuse to the receiving nurse. Only 9% of providers reported that the signs and symptoms of child abuse were clear. The top barriers to recognition/reporting included lack of education, dealing with patients’ family members, confusion regarding regulations, and a fear of being wrong. When asked about adding a short screening tool to the ePCR, 74.5% were in favor; 18.6% were undecided. Years of experience did not have a significant effect on any element of the survey.
Conclusion: This study demonstrates clear barriers to EMS providers recognizing and reporting abuse. Implementation of universal screening tools may be effective in the EMS setting. More research is needed to evaluate screening for child abuse by EMS providers. This study indicates EMS providers are willing to adopt a standardized screening tool into practice.
The Impact of Emergency Remote Teaching on EMS Exam Scores
Author: Kelly Kohler, MS, Paramedic, CHSE, NCEE
Associate Authors: Andrea M. La Lumia, MEd, NRP; Leah M. Tilden, MA, AEMT; J.D. Graziano, MS, NRP; Sarah C. Glass, BS, PMD, ASN; Thomas Fentress, MBA, NRP, PI, CFI; Sara Walker, MS, NRP; Han Gil Jeong, BS; Jose Palma, PhD(c)
The COVID pandemic has caused an unprecedented change in EMS education. Traditionally EMS classes have been held face-to-face (FTF) or in a blend of FTF and online learning. COVID required many EMS programs to move, at least temporarily, to an online format, for which many programs were unprepared. Previous research shows programs already using online learning management systems (LMS) are more prepared to shift to emergency remote teaching (ERT).
Objective: To examine differences in student exam scores post-transition to ERT between FTF, hybrid, and flipped classrooms.
Hypothesis: Null hypothesis: There is no difference in exam scores between hybrid, flipped, and FTF classrooms in ERT. Hypothesis No. 1: There is a difference in exam scores between hybrid, flipped, and FTF classrooms in ERT for EMT students. Hypothesis No. 2: There is a difference in exam scores between hybrid, flipped, and FTF classrooms in ERT for paramedic students.
Methods: Surveys were sent to EMS programs that utilize Fisdap. A total of 21 EMT programs and 27 paramedic programs responded. The survey asked 57 questions centering around adaptations EMS programs made in content delivery due to the pandemic. Data were analyzed by ANOVA, regression analysis, descriptive analyses, and t-tests.
Results: Before the pandemic there was a statistically significant difference in test scores between FTF, hybrid, and flipped classroom methods for EMT and paramedic classes (p<.01 and p<.05, respectively). Due to the pandemic, 86% of EMT programs and 84% of paramedic programs reported switching to ERT. After transitioning to ERT, there was no statistically significant difference in EMT or paramedic exam scores between FTF, hybrid, and flipped classroom methods. However, an increase was noted in exam scores for classrooms that were previously FTF, which is what eliminated any significant difference in scores.
Conclusion: The results reinforced previous research showing flipped classrooms led to increased student learning outcomes on cognitive exam scores pre-COVID. Interestingly, the results do not support research showing that using an LMS (flipped or hybrid classrooms) better prepares classes for emergency remote teaching. These findings suggest future research should focus on which components of online learning most contribute to student learning outcomes.
Emergency Medical Technician Training: A Mexico-USA Comparison
Author: Alfonso Salas, MPS, BSPT, EMT-P
Associate Authors: Gabriel Barrera, MEd, EMT; Andrés Quintero-Leyra, MD, EMT-P; Marisol Roldán, BSPsych, EMT; Michael Kaduce, MPS, NRP; Jessie Castillo, NRP; David Page, MS, NRP
Much of the prehospital care provided in Mexico and the United States of America (USA) is performed by emergency medical technicians (EMTs). Although national education standards establish minimum training requirements, variations exist in how education programs implement curricula despite the scope of practice in both countries being very similar.
Objective: To compare the educational curricula and program delivery models between the Mexican Red Cross, State of Mexico Delegation (MRC), and the University of California, Los Angeles (UCLA) EMT programs.
Methods: Lead instructors from the respective programs provided an hour breakdown of their EMT courses. Lecture topics (didactic), lab skill and simulation (psychomotor), and clinical/field hours were detailed. Class size, student-to-instructor ratio, total program length, and course completion rates were compared.
Results: EMT students completed a total of 843 and 182 hours of training, and of these 204 and 54 were lecture hours; 348 and 104 lab-simulation hours; and 150 and 24 field hours at MRC and UCLA, respectively. Average class sizes were 20.5 and 46 students, and laboratory student-instructor ratios were 6:1 and 10:1 for MRC and UCLA, respectively. Neither program had students complete clinical time in hospitals. See Figure 5 for topics and subtopic results.
Conclusion: EMT students in Mexico receive more education overall but specifically in the didactic areas of anatomy, physiology, simulation, nearly six times more field placement hours, and nearly a year in the classroom. More research is needed to further compare curriculum depth, breadth, teaching methodologies, students profiles for admission, and occupational expectations.
The Effect of COVID-19 on Practical Educational Opportunities for Paramedic Students: A Targeted Retrospective Analysis
Author: Erin Donathan, MPH, FPC, CCEMT-P
Associate Authors: Ryan Ockey, BS, NRP; Nigel Barr, PhD, NRP; Daniel Armstrong, DPT, EMT; Glen Keating, BS, Paramedic, RRT; James Dinsch, MS, NRP, CCEMT-P; Ruby Carlson; Christopher Goehnner, MHS, NRP, NCEE; Scott Lancaster, PhD, MHA, NRP
Performing advanced airway procedures on live patients is necessary for paramedic course completion. As the COVID-19 pandemic progressed, clinical guidance for those procedures was adjusted to reduce provider exposure.
Objective: To explore the effect of the pandemic on paramedic student opportunities to perform advanced airway procedures.
Methods: A retrospective analysis of Fisdap educational data was conducted. A total of 149,678 patient encounters were analyzed. Encounters that occurred from July through December of 2017, 2018, and 2019 were compared to patient encounters during the COVID-19 pandemic (July 2020 through December 2020). These two groups were compared using descriptive and inferential statistical analysis of variables attempted in the field by students and/or preceptors.
Results: Records of paramedic students were analyzed from July through December of 2017–2019 and compared to the same time period in 2020. This study focused solely on clinical shifts performed in the field, excluding lab or simulated shifts. The data were broken down into individual skill performed categories and a Pearson’s chi-square test was completed.
Conclusion: A statistically significant difference in the number of orotracheal intubations, Combitube/King LT insertions, ventilator with PEEP, and ventilatory operations performed by students exists between the prepandemic and pandemic clinical setting. There is also a statistically significant difference in the proportion of those skills performed by the paramedic vs. the preceptor in the field. This study highlights the importance for program directors and EMS educators to increase opportunities for students to perform and observe these skills in the current clinical setting.





