

Spotlight Interview: The Cleveland Clinic
What is the size of the EP lab facility and number of staff members? What is the mix of credentials in the lab?
 The Cleveland Clinic is composed of 7 EP labs and 1 cardioversion suite. A hybrid operating room is available within the Heart and Vascular Institute for complex procedures. In addition, we have 20 staff physicians, 10 EP fellows, 40 registered nurses (RNs), 1 clinical engineer/RN, 2 office specialists, 1 supply coordinator, and 1 patient care assistant. All technical support is provided by RNs. We do not employ CT or radiology technologists. Radiology technical support is available when needed.
The Cleveland Clinic is composed of 7 EP labs and 1 cardioversion suite. A hybrid operating room is available within the Heart and Vascular Institute for complex procedures. In addition, we have 20 staff physicians, 10 EP fellows, 40 registered nurses (RNs), 1 clinical engineer/RN, 2 office specialists, 1 supply coordinator, and 1 patient care assistant. All technical support is provided by RNs. We do not employ CT or radiology technologists. Radiology technical support is available when needed.
When was the EP lab started at your institution?
The EP laboratory originated in 1980 with 2 electrophysiologists, 2 RNs, and 1 secretary. The procedures were performed in a single, dedicated EP lab or in the cardiothoracic operating room. The EP Section currently has more than 150 personnel comprised of physicians, fellows, clinical nurses, research nurses, secretaries, monitoring technicians, and others who assist in the care we provide.
What types of procedures are performed at your facility? Approximately how many are performed each week?
 On average, we perform 100 procedures per week (over 5,700 cases in 2010). Procedures performed include: pacemakers, defibrillators, biventricular devices, device/lead extractions, loop recorders, and cardioversions. We also perform diagnostic EP procedures and ablations of atrial and ventricular arrhythmias using transvenous or percutaneous epicardial techniques. Procedure duration can range from 1 hour up to 12 hours for patients with exceptionally complex arrhythmias.
On average, we perform 100 procedures per week (over 5,700 cases in 2010). Procedures performed include: pacemakers, defibrillators, biventricular devices, device/lead extractions, loop recorders, and cardioversions. We also perform diagnostic EP procedures and ablations of atrial and ventricular arrhythmias using transvenous or percutaneous epicardial techniques. Procedure duration can range from 1 hour up to 12 hours for patients with exceptionally complex arrhythmias.
The Cleveland Clinic Syncope Center is located near the electrophysiology laboratories, but it is a separate facility staffed by other nurses and physicians. In aggregate, approximately 2,000 diagnostic studies are performed in the Syncope Center each year. These include tilt testing, blood volume studies, and other hemodynamic and neuroregulatory evaluations.
What is the primary goal of your program?
Our mission is to alleviate symptoms related to cardiac arrhythmias and heart failure, thereby reducing the risk of sudden cardiac death. Through world-class care and state-of-the-art technology, we help patients from all over the world who travel to Cleveland because of the expertise we offer. We also accept referrals from other hospitals whose patients have medical problems that are particularly complex or in whom a prior procedure was unsuccessful. This may include extraction of infected leads, or ablation of complex atrial or ventricular arrhythmias.
Who manages your EP lab?
 Patrick Parete, BSN, RN, CNOR, RNFA, is the Nurse Manager of the EP Lab with assistance from Kelly Melgun, BSN, RN and Cheryl Bell, BSN, RN. Dr. Bruce Lindsay heads the Section of Cardiac Pacing and Electrophysiology. Dr. Bruce Wilkoff, Dr. Pat Tchou, and Dr. Walid Saliba serve as Associate Section Heads. Dr. Saliba is the Medical Director of the EP Lab and Dr. Mohamed Kanj is the Associate Director. Dr. Bruce Wilkoff heads the Device Clinic and the Center for Electrical Therapy. Dr. Oussama Wazni directs the Outpatient Department and Dr. Callahan directs the inpatient service. Dr. Dresing is the Fellowship Director. Dr. Jaeger is the director of the syncope clinic.
Patrick Parete, BSN, RN, CNOR, RNFA, is the Nurse Manager of the EP Lab with assistance from Kelly Melgun, BSN, RN and Cheryl Bell, BSN, RN. Dr. Bruce Lindsay heads the Section of Cardiac Pacing and Electrophysiology. Dr. Bruce Wilkoff, Dr. Pat Tchou, and Dr. Walid Saliba serve as Associate Section Heads. Dr. Saliba is the Medical Director of the EP Lab and Dr. Mohamed Kanj is the Associate Director. Dr. Bruce Wilkoff heads the Device Clinic and the Center for Electrical Therapy. Dr. Oussama Wazni directs the Outpatient Department and Dr. Callahan directs the inpatient service. Dr. Dresing is the Fellowship Director. Dr. Jaeger is the director of the syncope clinic.
Is the EP lab separate from the cath lab? How long has this been? Are employees cross trained?
The Cleveland Clinic’s EP and cath labs have separate managers, nurses, and facilities. We have found that the degree of expertise required to function at a high level is best achieved by nurses who focus on electrophysiology, so we do not cross train nurses to work in both laboratories. Lisa Keene, RN serves as the education coordinator for the EP lab.
Do you have cross training inside the EP lab? What are the regulations in your state?
The RNs provide world-class care to our diverse and complex patient population by managing conscious sedation and monitoring hemodynamic status; they are also qualified to operate all mapping systems, ablation generators, device analyzers, EP recording systems, and programmable EP stimulators. We take pride in having our nurses develop these skills. Ohio does not permit nurses to administer deep sedation; however, the laboratory is staffed by a team of anesthesiologists and nurse anesthetists, directed by Dr. Sam Irefin, who administer deep sedation or general anesthesia if needed. Each patient is evaluated by our anesthesia team prior to the procedure. We will have an anesthesia machine in each room by the end of this year in order to reduce delays when patients are converted from conscious to deep sedation.
What new equipment, devices and/or products have been introduced at your lab lately?
 We strive to improve the quality of care through assessment of outcomes and introduction of new technologies related to ablation of cardiac arrhythmias, cardiac resynchronization, and novel devices for stroke prevention, lead extraction, pacing and defibrillation. We were the first in the United States to implant an MRI-safe permanent pacemaker. We have been involved in many trials for innovative technologies such as magnetic and robotic navigation, left atrial pressure monitoring devices, subcutaneous defibrillator trials, and the left atrial appendage closure device trial. We will begin to evaluate new technologies to assess contact force for ablation catheters later this month.
We strive to improve the quality of care through assessment of outcomes and introduction of new technologies related to ablation of cardiac arrhythmias, cardiac resynchronization, and novel devices for stroke prevention, lead extraction, pacing and defibrillation. We were the first in the United States to implant an MRI-safe permanent pacemaker. We have been involved in many trials for innovative technologies such as magnetic and robotic navigation, left atrial pressure monitoring devices, subcutaneous defibrillator trials, and the left atrial appendage closure device trial. We will begin to evaluate new technologies to assess contact force for ablation catheters later this month.
Have you recently upgraded your imaging technology?
Yes. We utilize state-of-the-art systems manufactured by Philips and Siemens. We also help in the co-development of new imaging features and trial some of their future technology before it becomes available for official release. We track the age and repair costs of all equipment and develop a schedule for maintenance and replacement as the equipment ages.
Who handles your procedure scheduling? Do you use particular software?
EP lab procedures are scheduled by either the Center for Atrial Fibrillation for PVI ablations or by one of the EP lab schedulers for all other types of procedures. Currently, the EP lab schedulers utilize Outlook Software; however, we will transition to OP-Time later in the year.
What type of quality control/quality assurance measures are practiced in your EP lab?
 Dr. Brian Baranowski and Ruth Madden, RN, lead the section’s program to monitor quality outcomes, which are reported to the HVI oversight committee. We have a comprehensive database, developed at the Cleveland Clinic, which is used for reports and to track outcomes of all procedures. We are in the process of revising the database to improve our ability to search it for quality measures and outcomes research in accordance with IRB-approved studies. A Database Committee chaired by Dr. Mina Chung reviews our data fields and makes changes as needed to improve functionality. We follow the Centers for Medicare & Medicaid Services (CMS) and the Joint Commission for standards and frequently perform quality audits from hand washing to documentation of procedural outcomes. We also abide by the College of American Pathologists (CAP) for standards of practice and are an accredited laboratory. All ICD implant data is entered into the National Cardiovascular Database Registry (NCDR®).
Dr. Brian Baranowski and Ruth Madden, RN, lead the section’s program to monitor quality outcomes, which are reported to the HVI oversight committee. We have a comprehensive database, developed at the Cleveland Clinic, which is used for reports and to track outcomes of all procedures. We are in the process of revising the database to improve our ability to search it for quality measures and outcomes research in accordance with IRB-approved studies. A Database Committee chaired by Dr. Mina Chung reviews our data fields and makes changes as needed to improve functionality. We follow the Centers for Medicare & Medicaid Services (CMS) and the Joint Commission for standards and frequently perform quality audits from hand washing to documentation of procedural outcomes. We also abide by the College of American Pathologists (CAP) for standards of practice and are an accredited laboratory. All ICD implant data is entered into the National Cardiovascular Database Registry (NCDR®).
How is inventory managed at your EP lab? Who handles the purchasing of equipment and supplies?
Our chief supply coordinator, Darlena Fisher, manages our inventory using QSight. Our Supply Chain Management Department handles all contracts related to purchasing of supplies and equipment.
Has your EP lab recently expanded in size and patient volume, or will it be in the near future?
The Sydell and Arnold Miller Family Heart and Vascular Institute is the largest Heart and Vascular Center in the United States. It is located on the main campus of the Cleveland Clinic and has 278 private rooms for patients and 110 ICU beds. After opening of the Heart and Vascular Institute, we expanded to 7 dedicated EP procedural labs in 2009. This allowed us to accommodate a steady increase in procedural volume.
How has managed care affected your EP lab and the care it provides patients?
Managed care has not had a major impact on the care we provide to patients.
Have you developed a referral base?
 Over the past 30 years, the Cleveland Clinic has been recognized as a leading institution for quality outcomes and clinical research, and because of that, we have trained and educated physicians who practice worldwide. Many of these physicians refer patients to the Cleveland Clinic because of the expertise we provide. We have international patients who come through our doors daily and we take care of those who have been turned away from other institutions because of the complexity of their problems. Since the Cleveland Clinic embraces a group practice model, a large number of patients are referred by other Cleveland Clinic physicians. The Cleveland Clinic has been recognized by U.S. News and World Report as the nation’s leading cardiovascular program for 16 consecutive years. Many patients are referred because of our expertise or they chose to come on their own accord.
Over the past 30 years, the Cleveland Clinic has been recognized as a leading institution for quality outcomes and clinical research, and because of that, we have trained and educated physicians who practice worldwide. Many of these physicians refer patients to the Cleveland Clinic because of the expertise we provide. We have international patients who come through our doors daily and we take care of those who have been turned away from other institutions because of the complexity of their problems. Since the Cleveland Clinic embraces a group practice model, a large number of patients are referred by other Cleveland Clinic physicians. The Cleveland Clinic has been recognized by U.S. News and World Report as the nation’s leading cardiovascular program for 16 consecutive years. Many patients are referred because of our expertise or they chose to come on their own accord.
What measures has your EP lab implemented in order to cut or contain costs? In addition, in what ways have you improved efficiencies in patient through-put?
The Cleveland Clinic Cardiac Rhythm Management team works with our Supply Chain Management to negotiate with industry to reduce the cost of all supplies used in the EP lab. We also track our start times and room turnover in order to improve the efficiency of the laboratories.
Does your EP lab compete for patients? Has your institution formed an alliance with others in the area?
We compete at a regional and national level with many other fine institutions. The Cleveland Clinic System includes the main campus and 6 other affiliated hospitals in the metropolitan area.
How are new employees oriented and trained at your facility?
New RNs have a 10–12 week orientation to the EP lab. Through a shared governance initiative, a comprehensive skills checklist was developed to promote growth regarding EP concepts. Further education and training is continued beyond the initial orientation period as well.
What types of continuing education opportunities are provided to staff members?
N urses have numerous opportunities for continuing education and training. These include weekly educational in-services, off-site training, and national conferences. In April of this year, we held our first EP Educational Conference Day, which was an all-day electrophysiology learning seminar for registered nurses across the Heart and Vascular Institute. In addition, we have nurses who continuously renew the CCRN certification as well as those who will sit for the exam in the coming months. Recently, we had two heart dissection classes where over 50 pig hearts were dissected by our nurses to study cardiac anatomy.
urses have numerous opportunities for continuing education and training. These include weekly educational in-services, off-site training, and national conferences. In April of this year, we held our first EP Educational Conference Day, which was an all-day electrophysiology learning seminar for registered nurses across the Heart and Vascular Institute. In addition, we have nurses who continuously renew the CCRN certification as well as those who will sit for the exam in the coming months. Recently, we had two heart dissection classes where over 50 pig hearts were dissected by our nurses to study cardiac anatomy.
How is staff competency evaluated?
Staff competency is evaluated annually through a computer-based program (COMET) and through hands-on equipment with the education coordinator.
How do you prevent staff burnout? In addition, do you practice any team-building exercises?
To prevent burnout within the EP lab, the management team rotates assignments within the lab and continuously offers learning opportunities. To promote team building, we have initiated multiple community outreach programs including purchasing turkeys for multiple food banks and sponsoring less fortunate families for Christmas. These initiatives have fostered an atmosphere of collegiality and collaboration.
What committees, if any, are staff members asked to serve on in your lab?
The nurses are involved in multiple committees: Ambulatory Practice Council, Conscious Sedation Task Force, Hospital Safety Committee, ITD Steering Committee, Skin Care Team, Professional Development Council, Dimensions in Cardiac Care Nursing Committee, Electronic Medical Records Committee, Shared Governance, and Magnet Accreditation Council. Due to their involvement in these endeavors, the nursing staff feel that they are engaged with the administration in improving the care of our patients and the environment in which we practice.
How do you handle vendor visits to your department? Do you contract with vendors?
Representatives from industry assist with programming during implantation of ICDs and provide additional support for 3D mapping when needed. Each representative is registered with the Cleveland Clinic and wears special attire when they work in the laboratory. They attend by invitation.
Does your lab utilize any alternative therapies to help patients in the EP lab?
Alternative therapies are not employed routinely, but we do accommodate patients who request these measures.
Describe a particularly memorable or bizarre case that has come through the EP lab. What lessons did you learn from it?
 There was an amusing and memorable case involving a patient who was a farmer. He was so focused on harvesting his crops that he ignored the device that eroded through his skin. When the device “popped out” of the pocket, he taped it to his shoulder and completed his work before he chose to come to the hospital. He was admitted and we extracted the device and leads later that day. With this case, we were reminded that every patient has a story to tell, so it is up to us to help them get back to an optimal level of health. We also have performed ablation procedures in patients with a variety of unusual anatomic problems (such as cor triatriatum) or performed transseptal punctures in patients who had undergone prior implantation of an atrial septal occlusion device.
There was an amusing and memorable case involving a patient who was a farmer. He was so focused on harvesting his crops that he ignored the device that eroded through his skin. When the device “popped out” of the pocket, he taped it to his shoulder and completed his work before he chose to come to the hospital. He was admitted and we extracted the device and leads later that day. With this case, we were reminded that every patient has a story to tell, so it is up to us to help them get back to an optimal level of health. We also have performed ablation procedures in patients with a variety of unusual anatomic problems (such as cor triatriatum) or performed transseptal punctures in patients who had undergone prior implantation of an atrial septal occlusion device.
How does your lab handle call time for staff members? How often is each staff member on call?
The EP laboratory has a variety of working hours to meet our patient needs. Nurses work either a 10- or 13-hour shift, enabling staffing to cover any potential emergency.
Does your lab use a third party for reprocessing?
The Cleveland Clinic reprocesses selected products through a commercial entity in accordance with FDA requirements.
Approximately what percentage of your ablation procedures is done with cryo? What percentage is done with radiofrequency?
Radiofrequency ablations greatly outnumber the cryothermal ablations, which comprise of about 5% of our current ablation volume. However, we are interested in some of the new cryoablation technologies and will evaluate them for safety and efficacy.
Do you perform only adult EP procedures or do you also do pediatric cases? Is there cross training for pediatric cases?
We have one pediatric electrophysiologist, Dr. Richard Sterba, who performs ablation procedures. A second pediatric electrophysiologist will join us this year. Pediatric lead extractions are performed by Dr. Wilkoff and others. The same RN staff is utilized for both adult and pediatric cases. Pediatric device implants are performed by the pediatric cardiothoracic surgeons in the operating room.
What measures has your lab taken to minimize radiation exposure to physicians and staff?
 All fluoroscopy systems are set to “low” exposure with appropriate collimation of the beam, frame rate, limitation of steep angulations, and selection of appropriate table height. We track the gray units for each patient and monitor exposure for the EP staff. The use of intracardiac echo and 3D mapping systems assist in reducing radiation usage. Lead aprons, thyroid collars, and eye protection are utilized among all staff members and are checked annually for integrity. The medical staff and fellows undergo annual training for radiation safety and use of our specific imaging systems.
All fluoroscopy systems are set to “low” exposure with appropriate collimation of the beam, frame rate, limitation of steep angulations, and selection of appropriate table height. We track the gray units for each patient and monitor exposure for the EP staff. The use of intracardiac echo and 3D mapping systems assist in reducing radiation usage. Lead aprons, thyroid collars, and eye protection are utilized among all staff members and are checked annually for integrity. The medical staff and fellows undergo annual training for radiation safety and use of our specific imaging systems.
Do your nurses/techs participate in the follow up of pacemakers and ICDs? If so, how many device visits per week do they handle? Do you use any particular software for follow up?
All of our implant data is transferred from the EP lab database to the Pacemaker and ICD Outpatient Clinic. Moreover, data from the Paceart system is transferred to the electronic medical record (EPIC). Patients with pacemakers, ICDs, and implantable loop recorders are followed in the Outpatient Department Device Clinic. In 2010, more than 25,000 pacemaker and ICD evaluations were performed in the clinic or through remote monitoring.
What innovative EP techniques are being utilized in your lab?
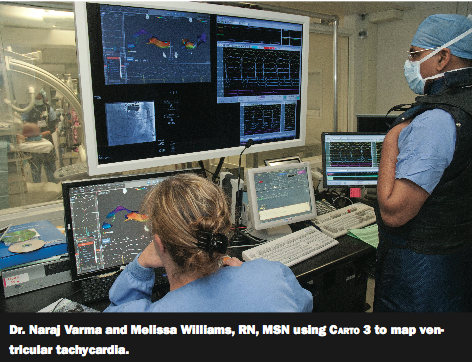
During implantation of pacemakers and ICDs, we record intracardiac electrograms to evaluate injury current at the lead implant site. Our laboratory extensively uses intracardiac echo (ICE) for ease and safety of intra-atrial transseptal punctures as well as vascular imaging for femoral access. This has decreased the likelihood of vascular complications in anticoagulated patients. We also track esophageal temperatures with all PVAI procedures to reduce the risk of thermal injury to the esophagus, and have selectively used endoscopy capsules to determine whether patients have developed any sign of ulceration. Magnetic and robotic navigation are used for selected ablation procedures. Electrocardiographic imaging is under study for noninvasive assessment of complex arrhythmias.
What are some of the dominant trends you see emerging in the practice of electrophysiology? How is your lab preparing for these future changes?
 The field of electrophysiology continues to evolve with new methods and technologies to improve outcomes. Since the inception of our laboratory, we have witnessed the development of nonthorocotomy lead systems for ICDs, endocardial and percutaneous epicardial ablation of arrhythmias, and extraction of leads. We anticipate that these procedures will continue to evolve with innovative catheter ablation and lead technologies. The challenge will be to control costs with the introduction of sophisticated technologies that improve patient care.
The field of electrophysiology continues to evolve with new methods and technologies to improve outcomes. Since the inception of our laboratory, we have witnessed the development of nonthorocotomy lead systems for ICDs, endocardial and percutaneous epicardial ablation of arrhythmias, and extraction of leads. We anticipate that these procedures will continue to evolve with innovative catheter ablation and lead technologies. The challenge will be to control costs with the introduction of sophisticated technologies that improve patient care.
What are your thoughts about non-EPs implanting ICDs? Do you train such individuals?
ICD implantations should be performed by physicians who meet training criteria as stipulated by the COCATS document or who underwent training and certification specified by the HRS-approved alternative pathway which was closed 3 years ago. Currently, we do not train physicians who are not enrolled in our fellowship program.
What about device recalls? How has your lab handled these?
The Pacemaker and ICD Device Clinic works in collaboration with industry to identify those patients who need to return for appropriate evaluation and treatment when the FDA issues a warning or recall.
Is your lab doing web-based/transtelephonic device follow-up?
The Device Clinic area follows the device patients with remote follow-up. An average of 50–60 remote follow-ups are performed daily.
Is your EP lab currently involved in any clinical research studies or special projects? Which ones?
 We are currently engaged in 19 clinical trials. These include the evaluation of new technologies for lead extraction, ablation of atrial fibrillation, innovative pacemakers and ICDs, and post-market trials. We have a team of research nurses, directed by Denise Kosty Sweeny, RN, who educate patients about the trials, collect data, and coordinate follow-up. Through the combined efforts of our nurses and physicians, these efforts have resulted in more than 100 publications in peer-reviewed manuscripts over the past 3 years.
We are currently engaged in 19 clinical trials. These include the evaluation of new technologies for lead extraction, ablation of atrial fibrillation, innovative pacemakers and ICDs, and post-market trials. We have a team of research nurses, directed by Denise Kosty Sweeny, RN, who educate patients about the trials, collect data, and coordinate follow-up. Through the combined efforts of our nurses and physicians, these efforts have resulted in more than 100 publications in peer-reviewed manuscripts over the past 3 years.
Are you ACGME-approved for EP training? What do you think about 2-year EP programs?
We offer 8 ACGME-approved fellowships and 2 international fellowships each year. As recognized in the COCATS document, most programs require 1.5 to 2 years of clinical training. Our program requires 2 years of training in cardiac electrophysiology and pacing after completion of a general cardiology fellowship.
Does your staff provide any educational materials for patients about their condition/procedure? In addition, does your hospital have a device support group for pacemaker or ICD patients?
The patients are given educational materials at the time of their appointment in the Outpatient Department, and they receive additional information in the mail prior to the procedure. They are given written pre-discharge instructions and educational pamphlets that cover our recommendations for care. Patients are also given a “contract” that explains our plan of action and their responsibilities during long-term follow-up of implantable devices.
Give an example of a difficult problem or challenge your lab has faced. How it was addressed?
 We felt that the number of nurses required to staff the laboratory was insufficient. An analysis by Kelly Hancock, MSN, RN, CNA-BC, Director of Nursing for the Heart and Vascular Institute, determined that we did not have enough nurses to cover the expansion of laboratories or time lost by vacations or illness. We established a target for recruitment and have steadily increased the number of nurses who staff our laboratory to accommodate the increase in procedural volume.
We felt that the number of nurses required to staff the laboratory was insufficient. An analysis by Kelly Hancock, MSN, RN, CNA-BC, Director of Nursing for the Heart and Vascular Institute, determined that we did not have enough nurses to cover the expansion of laboratories or time lost by vacations or illness. We established a target for recruitment and have steadily increased the number of nurses who staff our laboratory to accommodate the increase in procedural volume.
Describe your city or general regional area. How does it differ from the rest of the U.S.?
We are located in metropolitan Cleveland, Ohio, where there are several prestigious medical institutions. There are hotels adjacent to the medical center for patients and families who come from a distance, and the Cleveland Clinic offers shuttle services to several hotels in the area. The city has many world-class cultural attributes such as the symphony, playhouse square, and highly regarded museums.
Please tell our readers what you consider unique or innovative about your EP lab and staff.
Within the last 6 months, our EP lab has recently been awarded several special distinctions which included: “Certificate of Excellence” for outstanding performance and commitment to patient safety and quality care through accreditation; the “Patient Safety Champions” honor for being instrumental in facilitating collaboration between nursing, anesthesia, and physicians in order to implement the safety checklist in the EP lab; and “Ambulatory Nursing Unit of the Year,” Cleveland Clinic’s nursing excellence award. All of these merits were based upon the teamwork, dedication, and alliance among the nurses, ancillary staff, and physicians. This group effort also goes beyond the walls of the EP lab. Our cohesiveness comes together from multiple off-campus festivities, seasonal celebrations, a Christmas present-wrapping party for adopted families, and a combined total of 475 years nursing experience. That is what is truly unique about the Cleveland Clinic EP Lab.

