

A 58-Year Follow-up of Complete Surgical Correction of Tetralogy of Fallot: A Marvel of Modern Medicine
See EP Lab Digest's 2023 update on this article here!
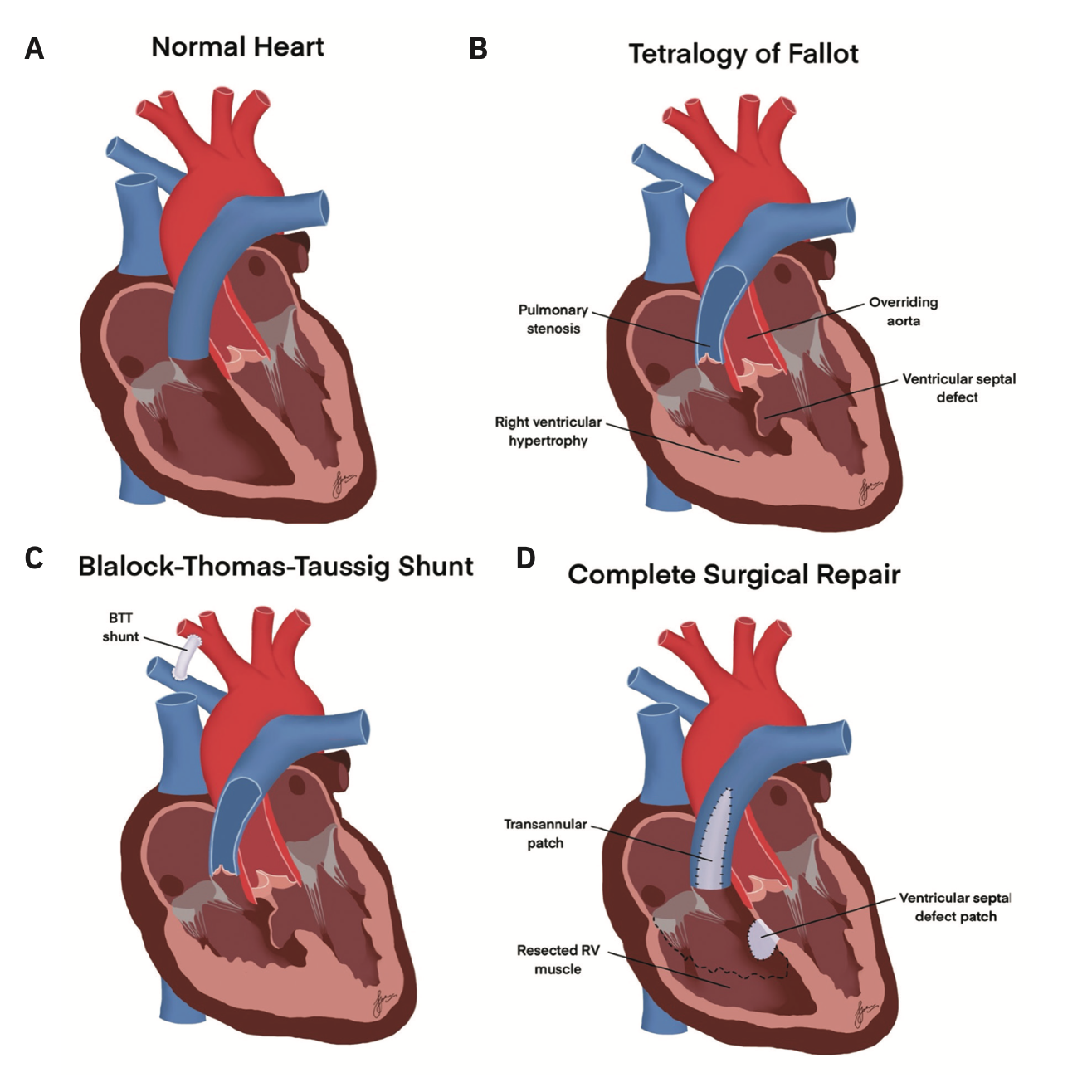
Tetralogy of Fallot (ToF) is a congenital cardiac malformation that affects 3 in every 10,000 live births.1 Newborns with ToF may have visibly blue lips or nail beds2 due to the clinical presentation of cyanosis arising from a tetrad of anatomical variations: ventricular septal defect, pulmonary infundibular stenosis, right ventricular hypertrophy, and overriding aorta (Figure 1A-B).1 ToF typically presents at 2-4 months of age, with symptoms of cyanosis, tachypnea, failure to thrive, and periods of hypercyanosis known as “tet spells.” Suspected ToF requires immediate screening that includes a transthoracic echocardiogram (TTE), electrocardiogram, and chest x-ray, followed by surgical intervention.2
Advancements in the treatment of ToF were spearheaded by the success of the Blalock-Thomas-Taussig (BTT) shunt at Johns Hopkins in 1944 (Figure 1C).3 Ten years later, the first successful complete surgical repair of ToF was performed by C. Walton Lillehei at the University of Minnesota.3 This achievement sparked an interest in alternative procedures for ToF surgical repair during the era of open-heart surgery.3 Surgical correction of ToF involves repair of the 4 anomalies (Figure 1D). Although surgical correction leads to decreased mortality rates, the procedure does not result in a fully functional heart.4 Sequelae of the repair include pulmonary regurgitation and long-term cardiac complications, thus requiring lifelong specialized medical care.1,2
This case report describes the follow-up and long-term care of a 68-year-old woman who participated in the original series at Columbia-Presbyterian Medical Center (1960-1965) and underwent a novel surgical procedure for complete correction of ToF.5
Case Presentation
In 1962, at the age of 9, the patient underwent a novel procedure for complete surgical correction of ToF at Columbia-Presbyterian Medical. The patient described being severely disabled preoperatively, appearing cyanotic with labored breathing. Following complete correction, she appeared asymptomatic, pink, and was able to begin living a normal life, participating in physical activities such as dancing.
In 2003, at the age of 50, the patient presented at New York University (NYU) Winthrop with refractory atrial tachyarrhythmias and near-syncope. An electrophysiology (EP) study revealed alternating rhythms of atrial fibrillation (AF), atrial flutter (AFL), and atrial tachycardia, with moderate His-Purkinje disease. The decision was made to perform an atrioventricular junction ablation, which resulted in complete heart block and led to the implantation of a permanent pacemaker.
In 2008, the patient presented at NYU Winthrop with symptomatic AFL and ablation was successfully performed. The EP study also revealed inducible sustained monomorphic ventricular tachycardia (VT), a common postsurgical arrhythmia of ToF repair.3 Despite a normal ejection fraction (EF) greater than 55%, she required a dual-chamber implantable cardioverter-defibrillator (ICD). This was performed in accordance with the 2008 American College of Cardiology/American Heart Association /Heart Rhythm Society guidelines for device-based therapy of cardiac rhythm abnormalities6 for secondary prevention, as a result of the patient’s structural heart disease, spontaneous sustained VT, and VT induced during her EP study. The patient later developed mild cardiomyopathy and symptomatic congestive heart failure (CHF). This was initially treated with ramipril, which alleviated her CHF symptoms. In December 2018, the patient was taken off of ramipril because of suspected drug-induced liver injury and put on sacubitril/valsartan and metoprolol shortly after due to symptomatic CHF.
In 2019, a TTE revealed mild impairment of left ventricular (LV) function, with an EF of 45% and moderate tricuspid regurgitation. ICD monitoring data also reported events of nonsustained VT with a maximal heart rate of 205 bpm. In 2020, fluid accumulation and elevated right atrial thresholds were also detected. A subsequent follow-up TTE revealed an EF of 35%.
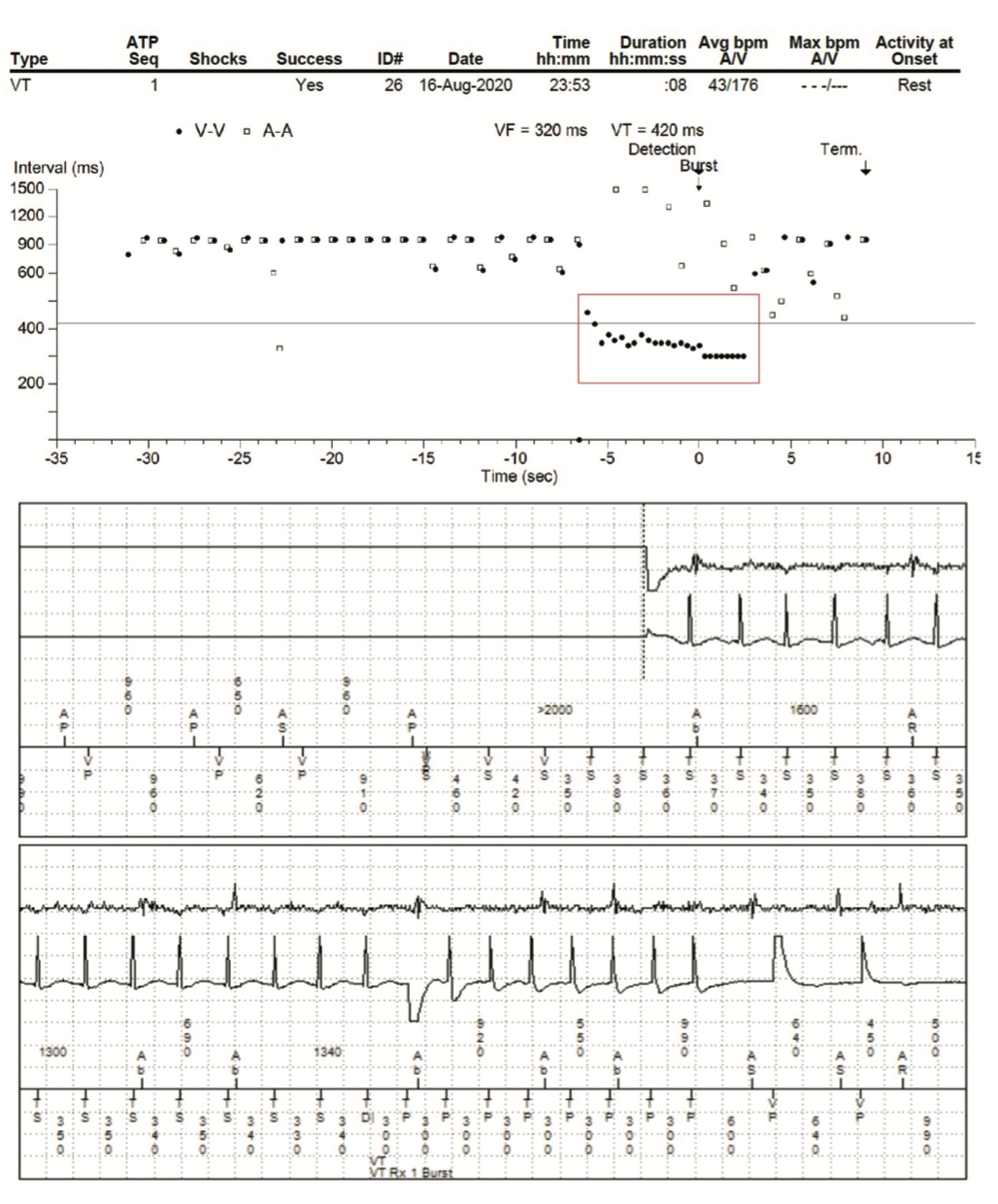
Since initial device implantation, the patient has needed a total of 6 implantable devices—2 pacemakers and 4 ICDs—most recently in 2018. Episodes of AF were detected, with a maximum duration of 40 minutes. OptiVol (Medtronic) threshold was reached in November 2019 and August 2020. A series of TTEs revealed moderate tricuspid regurgitation with mild impairment of LV function—decreased EF from 45% to 35% between 2019 and 2020. Since March 2008, her devices have recorded over 56 episodes of nonsustained VT, with 4 episodes of VT treated with antitachycardia pacing (Figure 2).
Despite optimal medical therapy, the patient was diagnosed with New York Heart Association Class III CHF. As of 2021, the patient is pharmacologically managed with metoprolol, sacubitril/valsartan, and aspirin, and pacemaker-dependent due to complete heart block. Given these factors, implantation of a biventricular pacemaker has been considered but may be challenging due to her anatomical abnormalities.
Discussion
The patient’s presentation of arrhythmias and CHF may have resulted from scarring of the ventricular septal patch, leading to substrates for VT and damaging the patient’s cardiac conduction system.1,7 These complications increase the risk of sudden cardiac death and encourage the implantation of an ICD in ToF patients.7
In this patient, the decision was made to perform complete ToF correction. The previous palliative standard of care (BTT shunt) was associated with a 2%-9% postoperative mortality rate.4 Comparatively, the original complete surgical correction of ToF, pioneered by Lillehei et al, had a 16%-35% postoperative mortality rate.4 This procedure described a vertical approach to the ventriculotomy, allowing adequate resection and reconstruction of the right ventricular outflow tract (RVOT), carried out at normal body temperature.8 Malm et al set out to refine this technique by placing the patient under induced hypothermia at 28º C and extensively dividing the hypertrophied trabeculae carneae to release the RVOT.4 This protocol decreased postoperative mortality rates to 7%, improved quality of life, and would become the standard of care for treatment of ToF.4,5,9
Although there is a relatively improved quality of life between the BTT shunt and complete correction, ToF patients continue to face the physical and mental burdens of living with this congenital disease.10 At the age of 68, our patient’s quality of life was assessed in March 2022 using the RAND 36-Item Short Form Survey. In comparison to the patients surveyed in Dłużniewska et al, our patient’s age is more than 3 standard deviations above the mean (30.6 years old). She performed better in the categories of physical, emotional, social, and overall general health. However, she received a lower score on her ability to perform more vigorous physical activities, which we speculate is due to her older age. Thus, our patient has exceeded expectations and sets the standard of care for future ToF patients.
Conclusion
To our knowledge, this case report details the most extensive long-term management and follow-up care after complete correction of ToF. We postulate that the series of cardiac events that occurred later in the patient’s life may be late-stage sequelae resulting from her ToF correction at the age of 9. This patient has benefited from cardiac rhythm management and the many scientific advancements made over the past half-century. She is truly a marvel of modern medicine.
Disclosures: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. They have no conflicts of interest to report regarding the content herein.
References
1. Bailliard F, Anderson RH. Tetralogy of Fallot. Orphanet J Rare Dis. 2009;4:2. doi:10.1186/1750-1172-4-2
2. O’Brien P, Marshall AC. Cardiology patient page. Tetralogy of Fallot. Circulation. 2014;130(4):e26-29. doi:10.1161/CIRCULATIONAHA.113.005547
3. Jacobs ML, Jacobs JP. The early history of surgery for patients with tetralogy of Fallot. Cardiol Young. 2008;18(S3):8-11. doi:10.1017/s1047951108003247
4. Malm JR, Bowman F, Jameson A, et al. An evaluation of total correction of tetralogy of Fallot. Circulation. 1963;27(4):805-811. https://doi.org/10.1161/01.cir.27.4.805
5. Malm JR, Blumenthal S, Bowman FO, et al. Factors that modify hemodynamic results in total correction of tetralogy of Fallot. J Thorac Cardiovasc Surg. 1966;52(4):502-513. https://doi.org/10.1016/s0022-5223(19)43394-1
6. Kusumoto FM, Calkins H, Boehmer J, et al. HRS/ACC/AHA expert consensus statement on the use of implantable cardioverter-defibrillator therapy in patients who are not included or not well represented in clinical trials. Circulation. 2014;130(1):94-125. doi:10.1161/cir.0000000000000056
7. Sherwin ED, Triedman JK, Walsh EP. Update on interventional electrophysiology in congenital heart disease. Circ Arrhythm Electrophysiol. 2013;6(5):1032-1040. doi:10.1161/CIRCEP.113.000313
8. Lillehei CW, Cohen M, Warden HE, et al. Direct vision intracardiac surgical correction of the tetralogy of Fallot, pentalogy of Fallot, and pulmonary atresia defects; report of first ten cases. Ann Surg. 1955;142(3):418-445. doi:10.1097/00000658-195509000-00010
9. Argenziano M, Smith C, Spotnitz H, Steinglass K, Bacha E. History of cardiothoracic surgery at Columbia University: a century at the vanguard of clinical care, education, and innovation. Semin Thorac Cardiovasc Surg. 2016;28(3):641-659. doi:10.1053/j.semtcvs.2016.10.014
10. Dłużniewska N, Podolec P, Olszowska M, et al. Quality of life in adults with repaired tetralogy of Fallot. Kardiochir Torakochirurgia Pol. 2018;15(2):107-113. doi:10.5114/kitp.2018.76476
Related Content




