

Cardiac Resynchronization Therapy in a Patient With Coronary Sinus Ostial Stenosis
A persistent left superior vena cava (PLSVC) is a common congenital malformation that may present difficulties when implanting cardiac devices. In a recent case, we identified a coronary sinus (CS) ostial stenosis with retrograde venous flow via the vein of Marshall and PLSVC following standard placement of the right-sided leads. In the rare patient with concomitant CS ostial obstruction and PLSVC, the presence of a PLSVC can provide an alternative access for lead implantation. In this article, we present a case involving left ventricular coronary sinus lead placement utilizing a previously unrecognized PLSVC in the setting of CS ostial stenosis.
Case Presentation
An 82-year-old male with history significant for multi-vessel coronary artery disease, mitral stenosis post coronary artery bypass grafting, and mitral valve repair, was referred for CRT-D implantation due to a persistent ejection fraction (EF) of 25% despite 90 days of optimal medical therapy with New York Heart Association (NYHA) class III heart failure symptoms and a left bundle branch block.
Left axillary vascular access was obtained with a left upper extremity venogram. A DF-4 lead (Boston Scientific) was successfully placed in the right ventricular apex followed by placement of the right atrial lead within the right atrial appendage. Both leads passed easily along the innominate vein and the superior vena cava (SVC). Appropriate sensing and pacing characteristics were exhibited and at this juncture there was no evidence of venous anomalies.
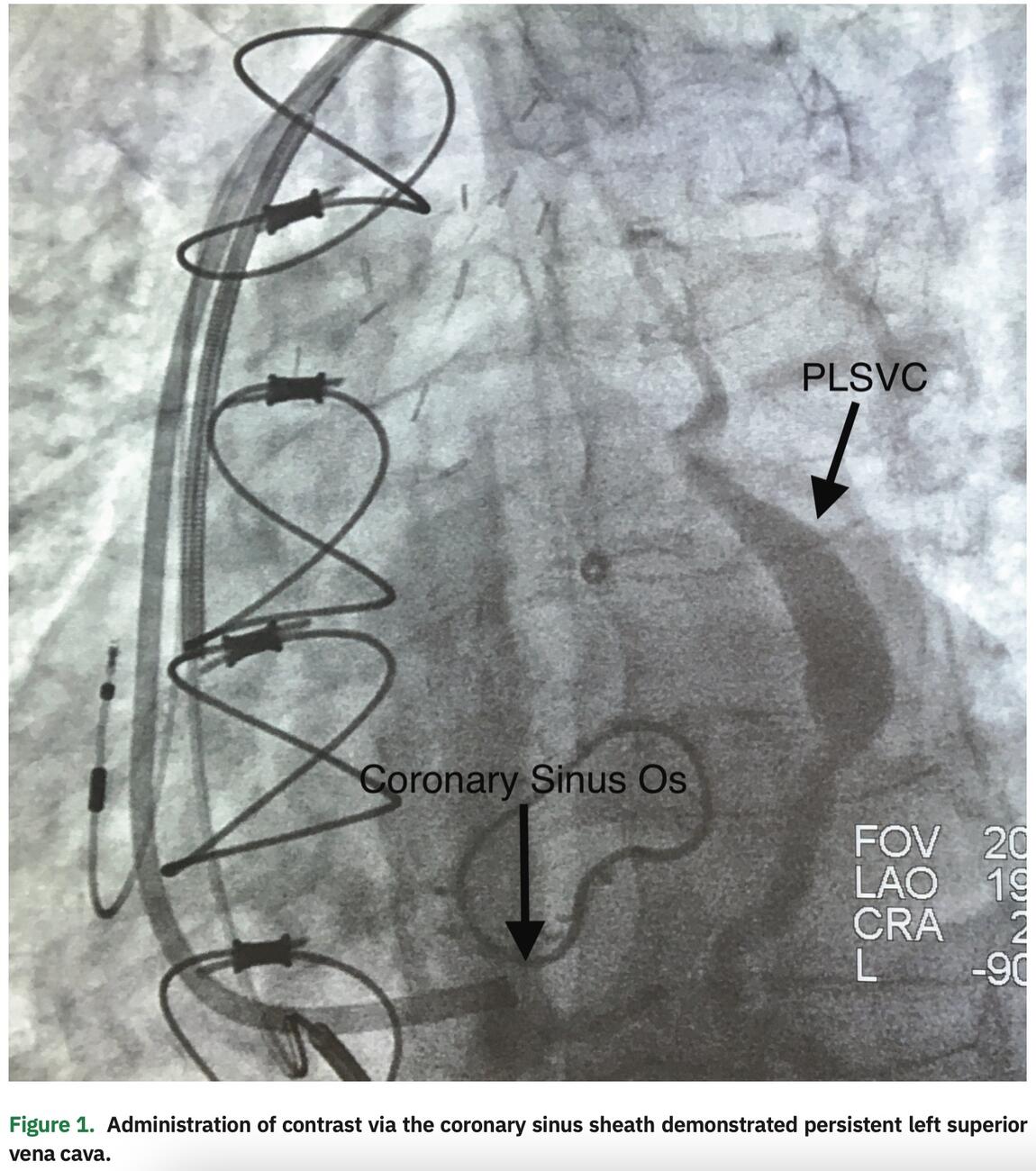
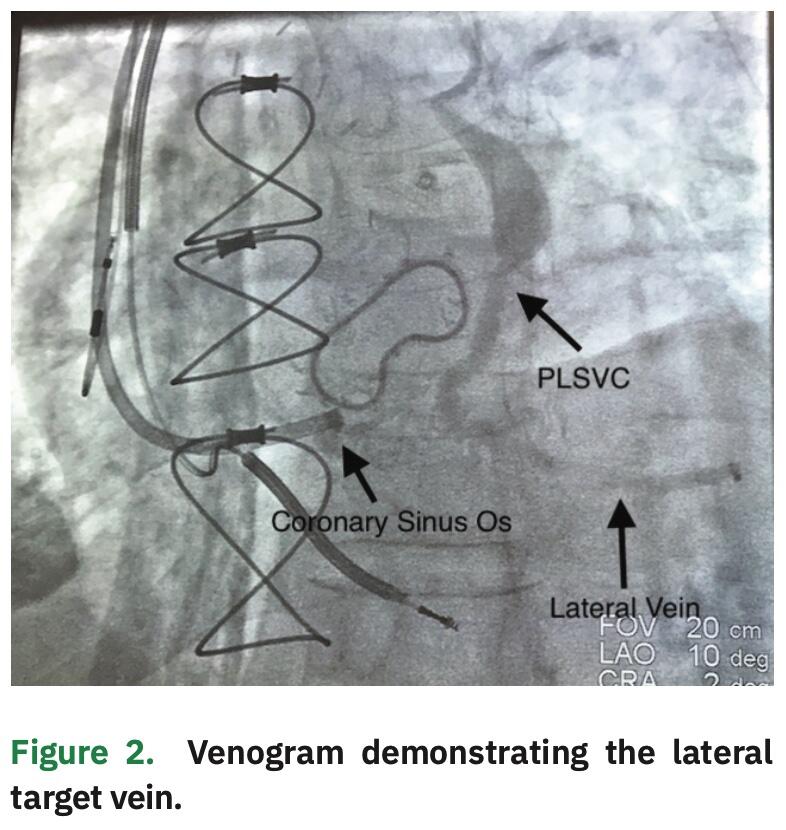
Subsequently, we attempted to selectively engage the CS ostium; however, an obstruction was encountered. An inner catheter was then used to partially engage the coronary sinus ostium, although the CS sheath could not be advanced. Angiography, via the CS sheath, revealed a subtotal occlusion and retrograde flow through what appeared to be a remnant vein of Marshall, but with a connection to the left innominate vein, consistent with a small PLSVC (Figure 2). Due to the CS ostial stenosis, the vein of Marshall or PLSVC provided venous return of the heart via its connection to the left innominate vein.
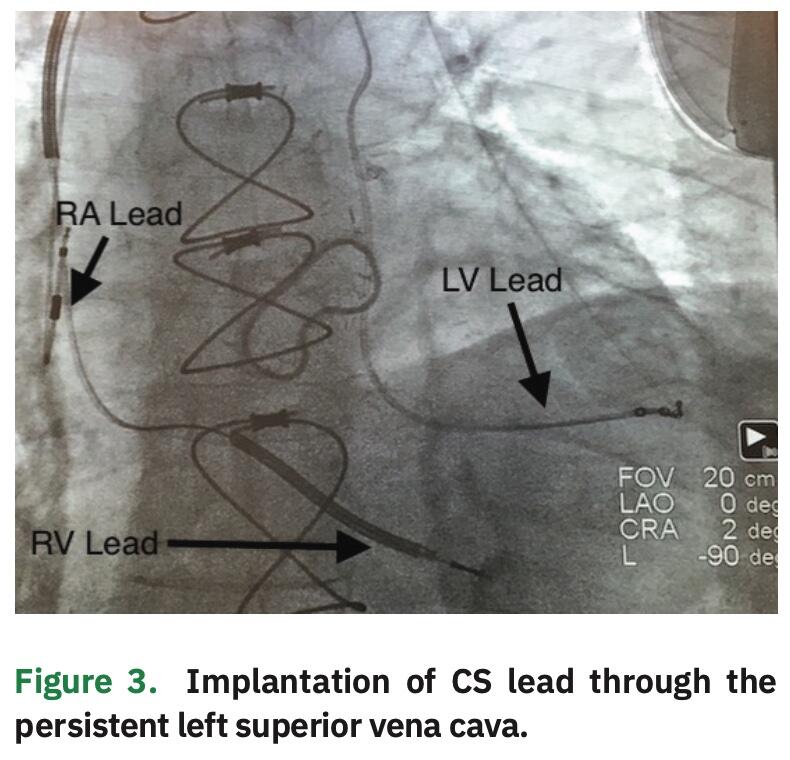
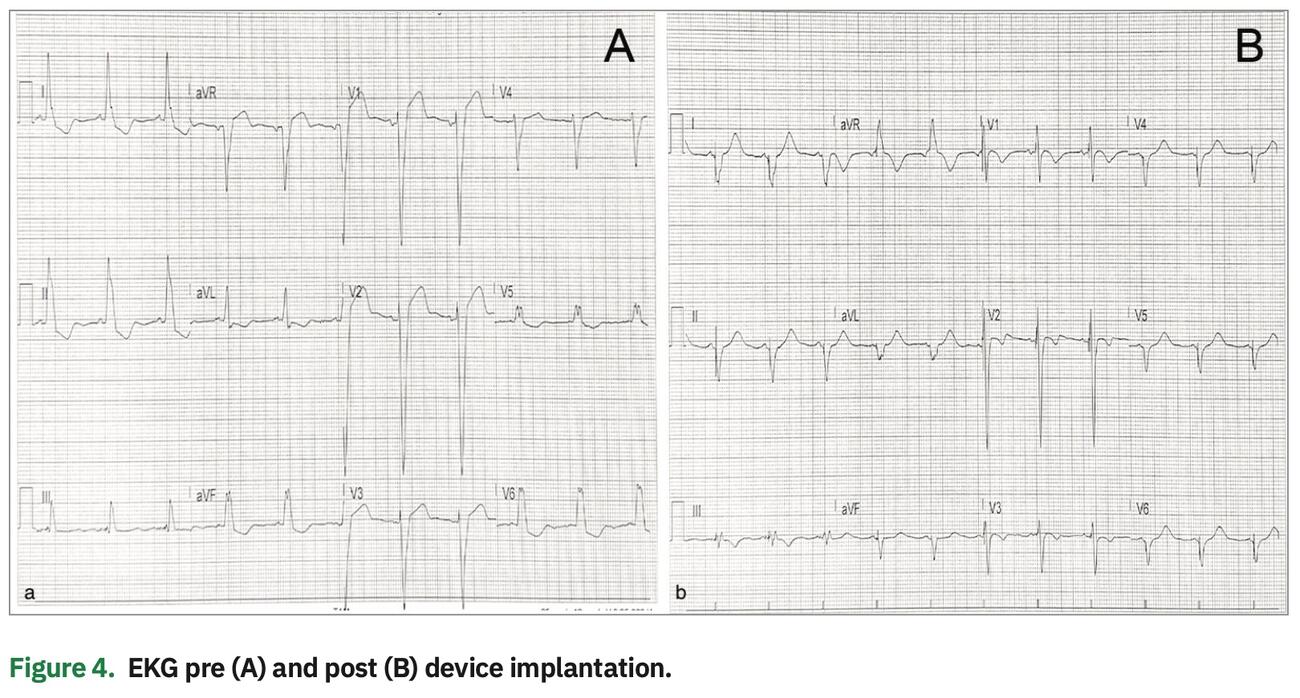
Given the subtotal occlusion, it was decided to abandon any further attempts of placement of the CS lead through the ostium. Rather, we proceeded with placement of the CS lead using the PLSVC. The previous venogram (Figure 1) demonstrated a medium to large caliber lateral vein without significant branching, which could be targeted with a quadripolar LV pacing lead. The inner catheter was utilized to subselect the PLSVC and deliver the lead into the lateral vein, which resulted in a stable lead position with adequate pacing and sensing characteristics. The greatest stability was achieved with the distal lead location within this vein. This site also provided an excellent pacing complex without diaphragmatic stimulation (Figure 4).
Discussion
A PLSVC is the most common thoracic venous malformation and is present in approximately 0.3 to 0.5% of patients in the general population.1 During normal embryonic development, anterior cardinal veins are formed, which drain blood from embryonic cranial structures. As development continues, the left and right cardinal veins are connected through an anastomosis with the brachiocephalic vein. This connection leads to asymmetric venous flow, causing the right anterior vein to develop into the right-sided SVC and regression of the left anterior cardinal vein into the ligament of Marshall.2 When this regression is incomplete, the remnant is identified as the vein of Marshall, which is typically imaged and occasionally cannulated during electrophysiology procedures involving the coronary sinus. When this regression fails to occur, the left anterior cardinal persists to become a PLSVC. In approximately 92% of patients, the PLSVC drains directly into the coronary sinus via the oblique vein of Marshall that drains into the right atrium. In the other 8% of patients, the PLSVC drains directly into the left atrium.3 A PLSVC is rarely the only superior venous return for the upper body. The majority of patients who are found to have a PLSVC typically have a normal right-sided SVC. Many patients with PLSVC will also have a left innominate vein that connects normally to the right-sided SVC, which allows for standard left-sided transvenous lead placement in the right atrium and ventricle.
In the majority of cases, a PLSVC is incidentally found, as patients are typically asymptomatic. Diagnosis of PLSVC can be confirmed via multiple imaging modalities, including transthoracic echocardiography, computed tomography (CT), and magnetic resonance imaging (MRI).
While the presence of a PLSVC adds difficulty to device implant cases, it does not typically prevent device implantation. In our case, the patient had a left innominate vein, which was used for the right atrial and right ventricular lead placement using a standard technique from the left side. This allowed us to place a dual-coil lead with the SVC coil in a standard anatomic position in the right SVC. Following attempts at cannulating the coronary sinus, our patient was found to have CS ostial stenosis, which subsequently led to the incidental diagnosis of a patent vein of Marshall with retrograde flow to the left innominate vein and an unrecognized PLSVC. It is this subpopulation of PLSVC patients with standard venous return via the SVC where the patent vein of Marshall may only be recognized during imaging of the CS if venography of the axillary and subclavian veins is not performed or incomplete. The CS is typically massively dilated if the PLSVC is the only venous drainage for the right upper extremity, and this dilation can make implantation of the right-sided atrial and ventricular leads, as well as the coronary sinus lead, more difficult.
Failure to cannulate the coronary sinus and/or implant the LV lead to a stable and acceptable position occurs in approximately 5 to 10% of cardiac resynchronization procedures.4 In these situations, current options would include placement of a surgical epicardial lead, placement of a His bundle lead, or a deep septal lead (left bundle) insertion to accomplish physiologic pacing to promote cardiac resynchronization.5
During our case, hand injection of contrast was directed into the CS at the level of the ostial stenosis, which allowed us to identify the vein of Marshall with retrograde flow to the left innominate vein or previously unrecognized PLSVC. Typically, the retrograde flow from the PLSVC drains into the right-sided SVC via the left brachiocephalic vein or innominate vein, which directs flow to the right SVC. While the CS ostial stenosis was likely secondary to the patient’s prior mitral valve surgery, we recognize that variants of congenital atresia of the CS ostium are within the differential diagnosis, particularly in the setting of the associated PLSVC. Regardless of the etiology, CS ostial obstructions complicate LV lead implantation when the inner sheath cannot be passed beyond the obstruction, as in our case.
Conclusion
This case illustrates how stenosis of the CS ostium may have led to recruitment of the oftentimes vestigial vein of Marshall and allowed placement of the LV lead through alternative venous approaches. While we were fortunate that we were able to image the vein of Marshall, we propose that prior to considering other options for LV lead placement, one should consider contrast injection in the innominate vein to search for this alternative connection to the vein of Marshall and coronary sinus body.
HCA Disclaimer
This research was supported (in whole or in part) by HCA and/or an HCA-affiliated entity. The views expressed in this publication represent those of the authors do not necessarily represent the official views of HCA or any of its affiliated entities.
- Tyrak KW, Holda J, Holda MK, Koziej M, Piatek K, Klimek-Piotrowska W. Persistent left superior vena cava. Cardiovasc J Afr. 2017;28:e1-e4. doi: 10.5830/CVJA-2016-084
- 2. Jacob M, Sokoll A, Mannherz HG. A case of persistent left and absent right superior caval vein: an anatomical and embryological perspective. Clin Anat. 2010;23:277-286. doi: 10.1002/ca.20945
- Pretorius PM, Gleeson F V. Case 74: Right-sided superior vena cava draining into left atrium in a patient with persistent left-sided superior vena cava. Radiology. 2004;232:730-734. doi: 10.1148/radiol.2323021092
- Lim PCY, Baskaran L, Ho KL, Teo WS, Ching CK. Coronary sinus ostial atresia and persistent left-sided superior vena cava: clinical significance and strategies for cardiac resynchronization therapy. Int J Angiol. 2013;22:199-202. doi: 10.1055/s-0033-1348882
- Huang W, Chen X, Su L, Wu S, Xia X, Vijayaraman P. A beginner’s guide to permanent left bundle branch pacing. Heart Rhythm. 2019;16:1791-1796. doi: 10.1016/j.hrthm.2019.06.016

