

Improving Electrophysiology Lab Efficiency

Those who work in the cardiac electrophysiology (EP) lab know that when leaving the house in the morning, there isn’t a guarantee you will be home in time for dinner. Some of this is due to external elements that are out of our control. There is a long list of contributing factors. For example, it is impossible to predict if a patient will arrive late or if the mapping system will not power up correctly. In recent years, we have collectively shifted our focus to the things that can be controlled to improve efficiency in our day-to-day clinical practice. Included here is a brief review of some of our best practices.
About Our Program
At Gundersen Health System, the cardiac catheterization and EP labs are one entity. We have 23 total staff members, including 10 dedicated EP staff. The core EP team consists of 4 nurses, 6 technicians, and 1 electrophysiologist. A dedicated call team is scheduled by rotation every night and on weekends, with an additional “late” team scheduled on days the EP lab is open. Our facility has 1 dedicated EP lab for ablations and device implants. We do additional device implants in either of the 2 cath labs as well. The EP lab is open 3 days per week, with an occasional add-on day for inpatient device implants or ablations. On a typical day in the EP lab, we perform at least 2 ablations or 2 device implants, or a combination of these procedures. From the start of 2020 to May 2022, we have performed 464 ablations and 250 device implants in our EP lab.
More Efficient Procedural Workflow
Since we have one lab solely for EP and one provider, efficiency is key to our practice. This begins with having dedicated cath lab staff. There are always 4 total staff members scheduled to the EP lab, with at least one being an EP core member.
The lab is often set up the afternoon or evening prior to procedures. This includes having leads laid out with electrodes in place, mapping patches set up, and the ultrasound machine placed in the room. Catheters, cables, sheaths, and tubing for the first procedure are also set aside.
The first patient is usually in the room by 7:30 AM. The 4 EP staff members work together to prepare the patient, including positioning, placing patches, and inserting a Foley catheter if necessary, while anesthesia staff intubates and places an arterial line. Once the procedure is underway, an EP core member gathers necessary equipment and primes the flush bags and tubing for the next case. This is also sometimes done by an EP core member who is scheduled in the cath lab for the day, but is in-between cases. Teamwork and communication throughout the case and within the entire cath lab are critical for finishing the first case and starting on the second procedure.
There are many moving parts to a timely turnover. In our next patient’s chart, the circulating nurse will input a “hypo start time” in the events tab of the electronic health record (Epic) about an hour before the first procedure is finished. This signals the anesthesiologist to see the next patient and for preop medication to be given. Patient readiness is then checked by the circulating nurse about 20 minutes before the first patient is about to leave the room. At this time, we call anesthesia if they have not yet seen the next patient, double check labs, anticoagulant status, and current medications. These are the key steps for ensuring the next patient will be ready.
When the procedure is finished, catheters and cables are removed from the sterile field. The scrub person caps and secures sheaths, placing extra gauze, syringes, towels, and dressings in a sterile bag while anesthesia extubates the patient. Patches and monitoring equipment are removed, and the patient is transferred to the post-anesthesia care unit (PACU) with the circulating nurse and anesthesia staff. Two available staff members from either the cath or EP staff will then pull sheaths and hold pressure in the PACU. This allows extra time for cleaning, finishing necessary documentation, and setting up for the next case.
After the patient has left the room, anesthesia techs and environmental assistants are paged to clean and restock equipment. EP staff stays to wipe down cables and equipment as well as assist anesthesia techs and environmental assistants to thoroughly clean the entire lab before the next procedure.
EP team members then set up the lab for the second case. Equipment is moved in, powered on, and tested if not done so already. The catheters, cables, tubing, and flush bags that were set aside earlier are quickly moved into the lab. The sterile table is opened and set up, while grounding pads, leads, defibrillator patches, and mapping patches are laid out.
The circulating nurse who transferred the first patient to the PACU returns to the lab to check on the status of setup. After checking the lab with the rest of the team, the nurse sends for the second patient. If staffing needs require it, this nurse may instead stay in the PACU to pull sheaths and hold pressure. In this instance, an available nurse from the cath lab or a nurse from the EP team will come to the EP lab to send for the second patient.
Once a device implant or ablation procedure has begun, it can be completed with 3 of the 4 EP staff members, which allows for breaks to be taken on a rotating basis. Breaks are also sometimes taken during turnover if a cath lab staff member assists. A full 30-minute lunch and two 15-minute breaks while working in a busy lab is never guaranteed. This is fully understood, and breaks are taken as procedures and staffing allow.
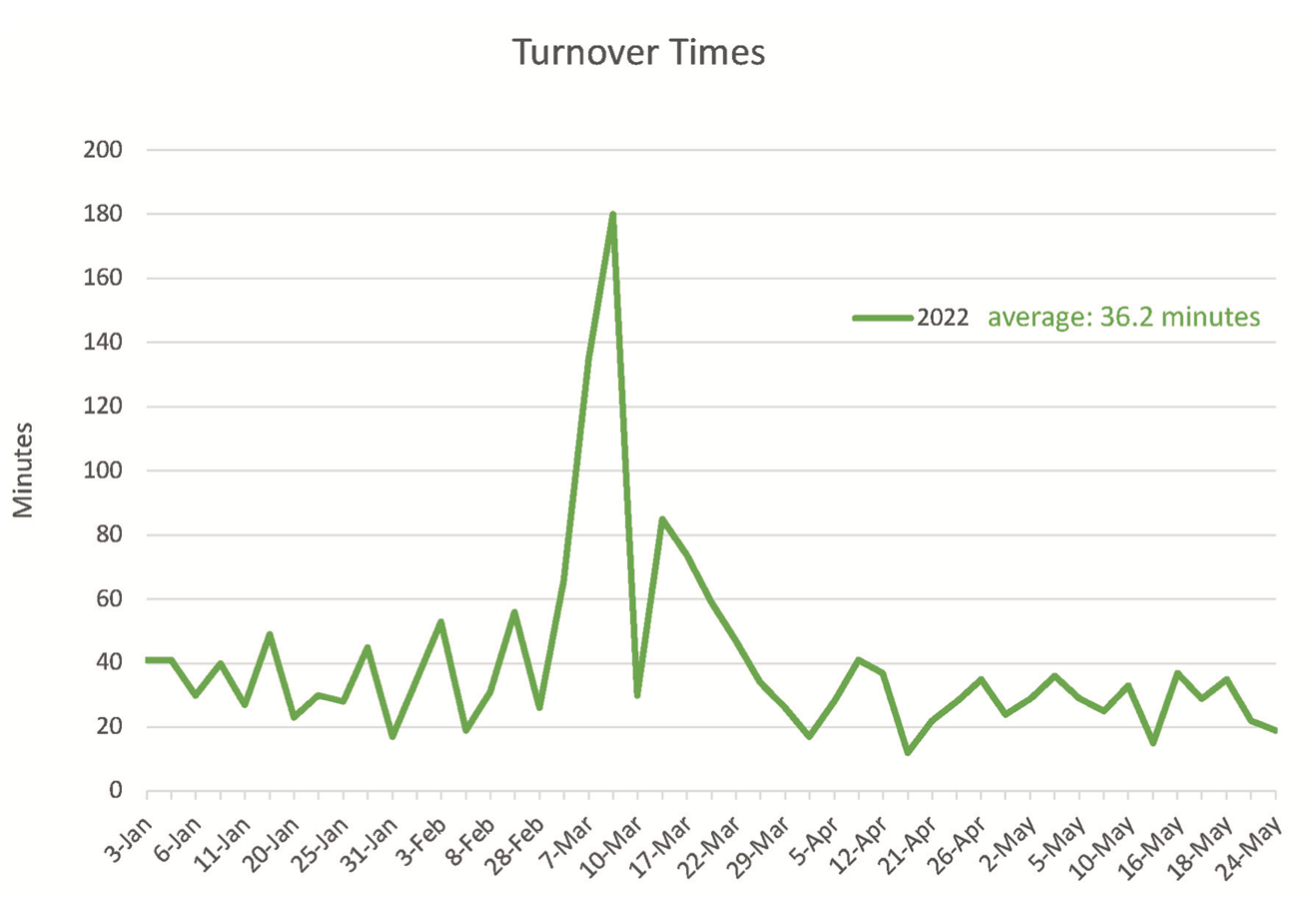
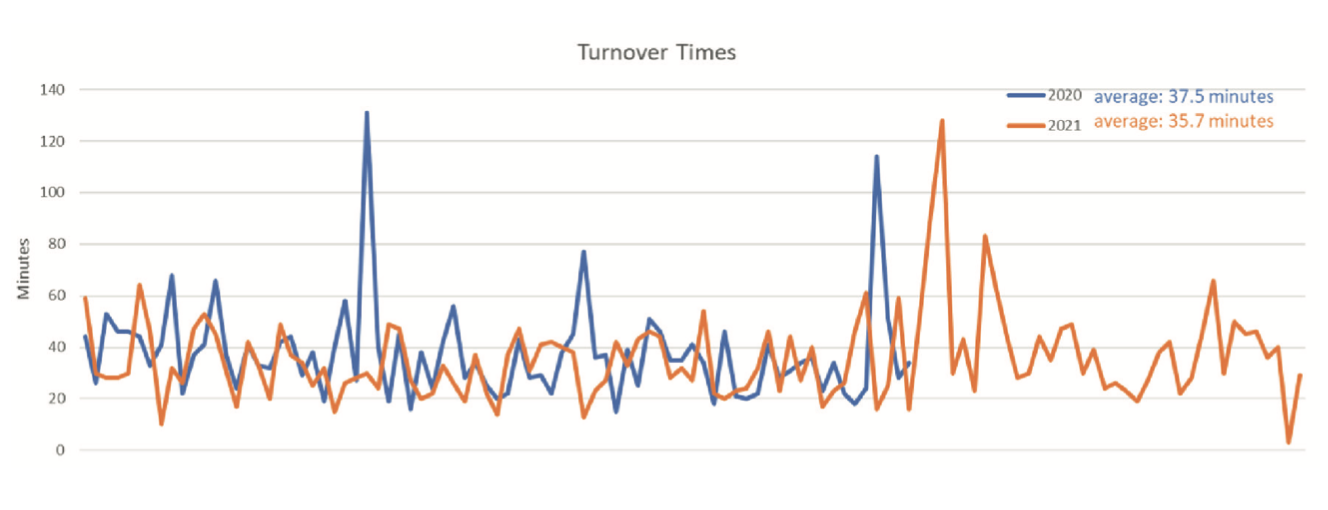
In 2022, we are averaging a 36-minute turnaround time (Figure 1). We measure turnover time from when the first patient leaves the room to when the next patient is documented in the room. During the 54 times the lab was turned over, 4 of those turnaround times exceeded 60 minutes. In one instance, the first procedure ended sooner than expected. In another, the second patient was an inpatient add-on and needed additional workup. While intraprocedural delays are documented in Epic, we are still working on a more streamlined way to keep track of delays that happen prior to the patient being in the room. Since a variety of procedures are performed in our lab, it is not uncommon for a device implant to follow an ablation, or vice versa. These data are not based on specific procedures. The average turnaround time has stayed relatively consistent since 2020 (Figure 2).
When the second patient enters the lab, we want to be prepared to start the case. If we are not ready, a page will be sent to the nurse to delay sending the patient. This keeps all focus on optimal patient care.
Summary
Teamwork and good communication were critical in helping our EP lab adopt more efficient methods for shortening the length of time between cases. For others interested in improving lab efficiency, a good place to start is to consider how many staff members are scheduled in the EP lab for any given procedure and whether sheaths will be pulled outside of the lab after an ablation, and by whom. It has been our experience that the use of the techniques mentioned in this article has resulted in faster lab turnaround times and less days stayed afterhours.
Gundersen Health System is on Twitter at @gundersenhealth.
Disclosures: The author has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest, and has no conflicts of interest to report regarding the content herein.

