Commercial Experience With the PulseSelect™ Pulsed Field Ablation System
Interview With Arash Aryana, MD, PhD, FACC, FHRS
Interview With Arash Aryana, MD, PhD, FACC, FHRS
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2024;24(5):10,12-13.
 In this article, Arash Aryana, MD, PhD, FACC, FHRS, describes his early commercial experience with the PulseSelect™ Pulsed Field Ablation (PFA) system (Medtronic), the first PFA system available in the United States and the only PFA system approved to treat both paroxysmal and persistent atrial fibrillation (AF) patients. Dr Aryana is the Director of the Cardiovascular Services and also the Cardiac Electrophysiology Laboratory at Mercy General Hospital in Sacramento, California.
In this article, Arash Aryana, MD, PhD, FACC, FHRS, describes his early commercial experience with the PulseSelect™ Pulsed Field Ablation (PFA) system (Medtronic), the first PFA system available in the United States and the only PFA system approved to treat both paroxysmal and persistent atrial fibrillation (AF) patients. Dr Aryana is the Director of the Cardiovascular Services and also the Cardiac Electrophysiology Laboratory at Mercy General Hospital in Sacramento, California.
Can you describe the PulseSelect PFA system?
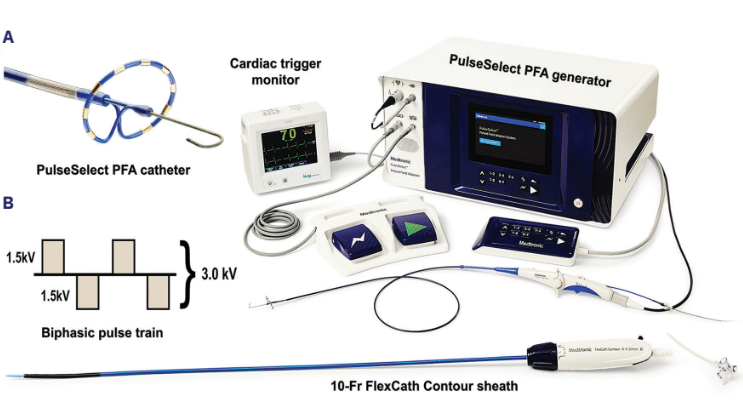
The PulseSelect PFA system (Medtronic) consists of a 9 French (F), 25-mm mapping/PFA array catheter (Figure 1A) with bidirectional steering. The catheter is equipped with nine 3-mm gold electrodes spaced 3.75 mm apart, delivered over a guide wire and paired with a 10F bidirectional steerable sheath (FlexCath Contour, Medtronic). The catheter delivers a bipolar, biphasic pulsed field waveform, with each application consisting of 4 pulsed trains. Alternating positive and negative electrodes deliver a high-intensity (1.5 kV) bipolar electric field for short durations (100-200 ms) to the cardiac tissue (Figure 1B). The applied electric field results in formation of pores within the cell membrane, which in turn leads to cell death through irreversible electroporation.1
What were key learnings in your first 5-10 procedures?
Catheter positioning and contact are key during PFA. Since the PulseSelect array exhibits a horseshoe configuration (Figure 2), it is important to carefully and methodically rotate the PFA catheter to a new position after each application to attain contiguous, circumferential pulmonary vein isolation (PVI). Given the 25-mm diameter of the catheter, placement may be initially more distal at the PV ostia. Although it is reasonable to first begin ablation at the PV ostia using this catheter, in order to ensure clinical efficacy, it is critical that pulsed field applications are also delivered more proximally at the PV antra to achieve wide area, antral circumferential PVI.
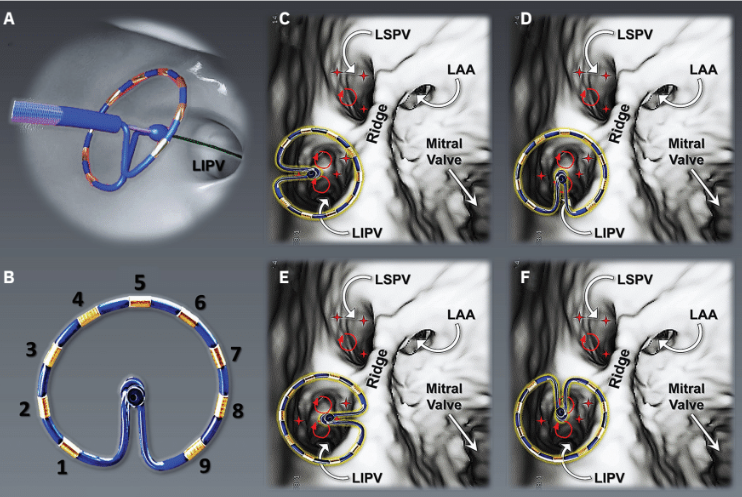
LAA=left atrial appendage; LIPV=left inferior pulmonary vein; LSPV=left superior pulmonary vein.
Can you describe the workflow you have developed with PulseSelect? What visualization techniques do you use? Can you describe the catheter and sheath handling?
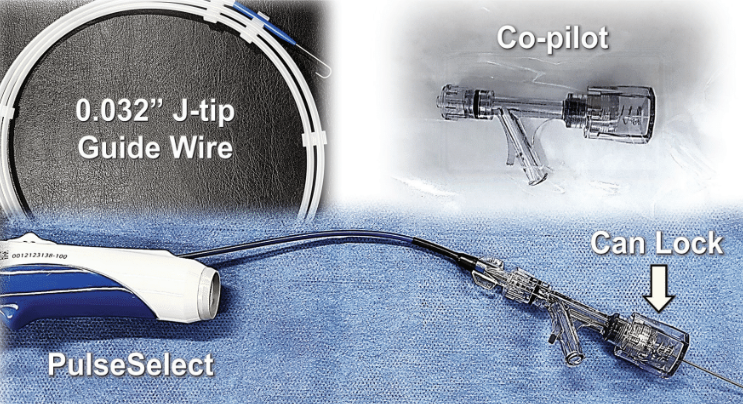
I perform these procedures either under general anesthesia or monitored anesthesia care. I typically begin by creating a 3-dimensional (3D) map of the left atrium (LA) and the PVs. Once the PV and the LA anatomy have been defined, I proceed with PFA. I typically ablate each PV first ostially and then antrally, working my way proximally into the PV component (the LA tissue lying between the PVs on the posterior LA wall). The PFA catheter is delivered over a 0.032” J-tip guide wire (Figure 3). By advancing the guide wire deeper into the PV, the operator can stably position the PFA catheter more proximally at the PV antrum. Catheter stability is facilitated through the use of a copilot (Figure 3) to secure (lock) the guide wire in place. This maneuver is then used to systematically ablate the LA roof and the PV component of the LA posterior wall. I also deliver additional applications to the LA ridge and the carina to achieve wide area antral isolation anterior to the PVs. Otherwise, these areas may be spared, as is also often the case with other conventional circular or single-shot ablation catheters (ie, the cryoballoon).
To achieve effective tissue contact, deflection and clockwise versus counterclockwise rotation of the introducer are required. When targeting the left PVs, turning the introducer clockwise allows the operator to position the catheter posteriorly, whereas a counterclockwise rotation positions the catheter anteriorly. On the contrary, when facing the right PVs, a clockwise rotation yields an anterior position, while turning the introducer counterclockwise results in positioning it posteriorly. In general, I find 3D mapping highly beneficial in guiding catheter positioning (Figure 4A and 4B). Furthermore, intracardiac echocardiography (ICE) is very helpful in facilitating this procedure. ICE not only aids with catheter positioning (ie, at PV ostia versus antra), but it can also guide and confirm electrode–tissue contact (Figure 4C).
What did you appreciate most about the system?
First and foremost, I appreciate the excellent safety of PFA using the PulseSelect system. Moreover, I appreciate its ease of use and gentle learning curve, which I would compare to that of the cryoballoon. I also appreciate the improved procedural efficiency associated with a PulseSelect PFA procedure.
How do you see PFA fitting into your lab in the future?
At this point, my colleagues and I are prioritizing PFA for all our de novo ablation procedures in patients with both paroxysmal and non-paroxysmal AF over all other thermal ablation modalities, and we see this trend continuing into the future. Given our overall favorable experience with PFA at Mercy General Hospital, our group remains highly enthusiastic about this ablation strategy. Nonetheless, there is still a need for further research in this space, specifically with regard to long-term clinical efficacy and outcomes.
What do you see as the biggest benefits of PulseSelect?
In my view, the principal benefit related to PulseSelect and, for that matter, all PFA technologies, has to do with the improved safety associated with this ablation strategy, specifically with respect to adjacent collateral structures such as the esophagus and the phrenic nerve.2 This was evident in the PULSED AF (Pulsed Field Ablation to Irreversibly Electroporate Tissue and Treat AF) study, a prospective, multicenter study in which patients with paroxysmal or persistent AF refractory to class I/III antiarrhythmic drugs were treated using the PulseSelect PFA system.3 This study demonstrated an exceedingly low adverse event rate (0.7%), while maintaining a reasonable efficacy that was still consistent with thermal-based ablation strategies.3
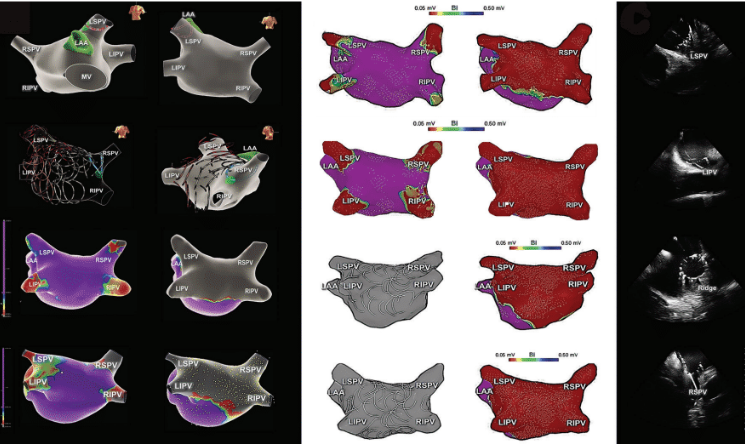
LAA=left atrial appendage; LIPV=left inferior pulmonary vein; LSPV=left superior pulmonary vein; RIPV=right inferior pulmonary vein; RSPV=right superior pulmonary vein.
What advice would you give to a physician who is about to use PulseSelect for the first time?
I would advise my colleagues who are interested in using this innovative and novel technology to remain mindful of 2 key issues: (1) electrode–tissue contact and (2) catheter positioning at the PV antra, both of which are necessary prerequisites during PFA to ensure durable and effective PVI. I would also strongly advise new users to consider employing both 3D mapping and ICE for optimal catheter visualization and positioning. Moreover, if extended lesions beyond the PVs are desired (ie, the posterior wall and the PV component), the use of visual aids such as 3D mapping is not only invaluable, but a must.
If you could describe the PulseSelect system in one word, what would it be?
If I had to describe the PulseSelect PFA system in just one word, the word “safe” is what would come to mind. Based on our own experiences and the results from the PULSED AF study,3 the safety of the PulseSelect PFA system appears exceptional.
Disclosure: Dr Aryana has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. He reports consulting fees and speaking honoraria from Medtronic.
This content was published with support from Medtronic.
References
1. Maor E, Sugrue A, Witt C, et al. Pulsed electric fields for cardiac ablation and beyond: a state-of-the-art review. Heart Rhythm. 2019;16(7):1112-1120. doi:10.1016/j.hrthm.2019.01.012
2. Reddy VY, Koruth J, Jais P, et al. Ablation of atrial fibrillation with pulsed electric fields: an ultra-rapid, tissue-selective modality for cardiac ablation. JACC Clin Electrophysiol. 2018;4(8):987-995. doi:10.1016/j.jacep.2018.04.005
3. Verma A, Haines DE, Boersma LV, et al; PULSED AF Investigators. Pulsed field ablation for the treatment of atrial fibrillation: PULSED AF Pivotal Trial. Circulation. 2023;147(19):1422-1432. doi:10.1161/CIRCULATIONAHA.123.063988
Related Content