

Leadless Cardiac Resynchronization Therapy Implantation: Experience at Naples Community Hospital (NCH) Healthcare System
In this interview, EP Lab Digest talks with Dinesh Sharma, MD, about the first totally leadless cardiac resynchronization therapy (CRT) implantation in the United States using the Micra Transcatheter Pacing System (Medtronic) with the WiSE CRT System (EBR Systems, Inc). Dr Sharma is chair holder of the Kathy and Fritz Friday Endowed Chair of Electrophysiology (EP) at Naples Heart Institute in Naples, Florida.
Tell us about your team at NCH and the heart failure (HF) patients you see on a daily basis.
© 2017 EBR Systems, Inc. All rights reserved. Used with permission by EBR Systems, Inc
NCH Healthcare System is a community-based hospital system with 3 electrophysiologists and approximately 20 cardiologists. Most of the cardiologists see patients with HF, and we have 1 HF specialist on staff. In terms of our demographics, most of our patients are older than 60 years, so we tend to treat a significant amount of HF.
What is your vision for the EP research team and future projects at Naples?
We envision ourselves to be one of the top cardiac centers in Florida. We have many cutting-edge trials such as pulsed field ablation, renal denervation, and left atrial appendage occlusion. We want our community to have the most cutting-edge technologies and best treatments available, which is the driving force. There is a strong hospital and physician partnership, so we receive a lot of support and encouragement from the administration and leadership. We see ourselves as being leaders in groundbreaking clinical trial research.
Would you share a bit about your experience with leadless pacing technologies? What are the advantages to leadless pacing in general, and how widely is it becoming utilized at NCH?
© 2017 EBR Systems, Inc. All rights reserved. Used with permission by EBR Systems, Inc
In terms of available leadless pacing technologies, the Micra (Medtronic) and Aveir single-chamber (VR) leadless pacemaker (Abbott) have been approved by the US Food and Drug Administration (FDA). We use the leadless pacemaker for patients with indications for ventricular pacing, including patients with atrial fibrillation. We find that there is a patient preference for leadless technology. Patients do not want to have leads in place because of physical activity restrictions. With leadless technology, patients can continue playing golf and going about their daily activities. Therefore, when the pacemaker is implanted for indications other than sinoatrial node dysfunction at our hospital, we tend to choose the leadless pacemaker.
The WiSE CRT System provides leadless, left ventricular (LV) endocardial pacing for patients who would benefit from CRT. There are challenges with conventional devices, such as access issues or the inability to implant the coronary sinus lead in the target branch. In those situations, the WiSE CRT System is particularly beneficial. Because of vascular access issues with our patient, the use of the WiSE CRT System was a natural choice for us for the first leadless implant at our hospital. Because the patient did not qualify for the SOLVE-CRT trial because their ejection fraction (EF) was above 35%, we received a compassionate use provision from the FDA. In addition, the patient was thrilled about the technology because it gave him the option for cardiac resynchronization.
The WiSE CRT System is an investigational device in the United States, limited by US (federal) law to investigational use only. You and your team at NCH performed the first totally leadless CRT pacemaker system implant in the United States: the WiSE CRT System operating in conjunction with a leadless intracardiac pacemaker. What can you tell us about this first procedure?
© 2017 EBR Systems, Inc. All rights reserved. Used with permission by EBR Systems, Inc
This was the first case in the United States to combine 2 leadless systems, the Micra with the WiSE CRT System. While we perform Micra implantation quite frequently, there was a learning curve with the WiSE CRT System, as with any new technology. However, we received excellent technical support from the EBR team during the case, and after putting their best practices into place, we had a great outcome. The implantation went very well and it was an exhilarating experience.
What are the components of the WiSE CRT System? Why is the WiSE CRT System a viable option to upgrade a leadless pacemaker to CRT without replacing a patient’s current pacing device?
The patient had left bundle branch block and an EF of 40%-45%. As the Micra provides only right ventricle (RV) pacing, there were concerns regarding dyssynchrony and a further decrease in the patient’s EF. Ideally, implanting a conventional biventricular pacemaker with a lead in the RV and a lead in the LV would make sense. However, with a vascular access issue, such as if the subclavian vein could not be accessed to place the leads, the WiSE CRT System is a more viable option because subclavian access is not needed. Either a retrograde aortic or transseptal approach is used to access the LV.
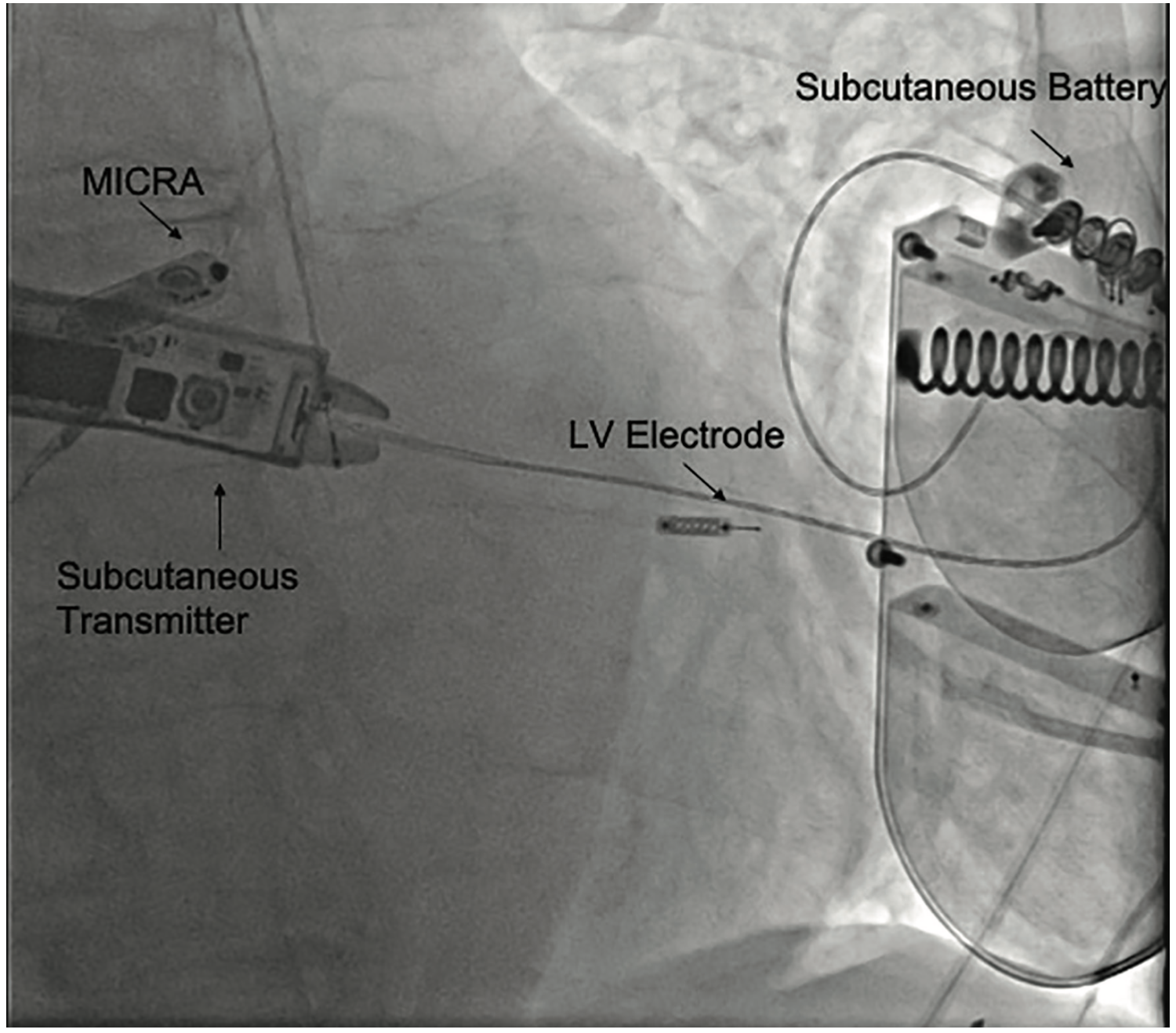
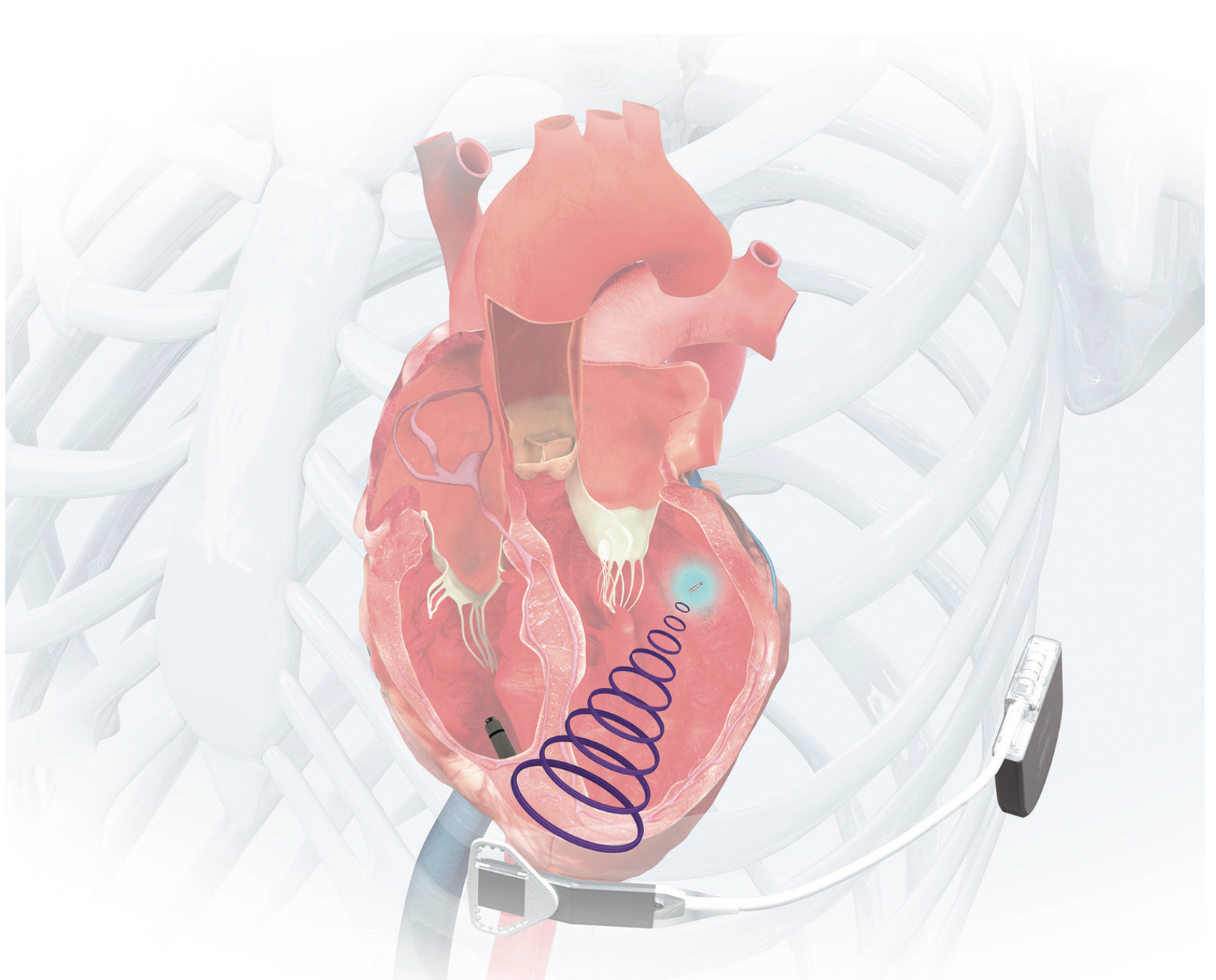
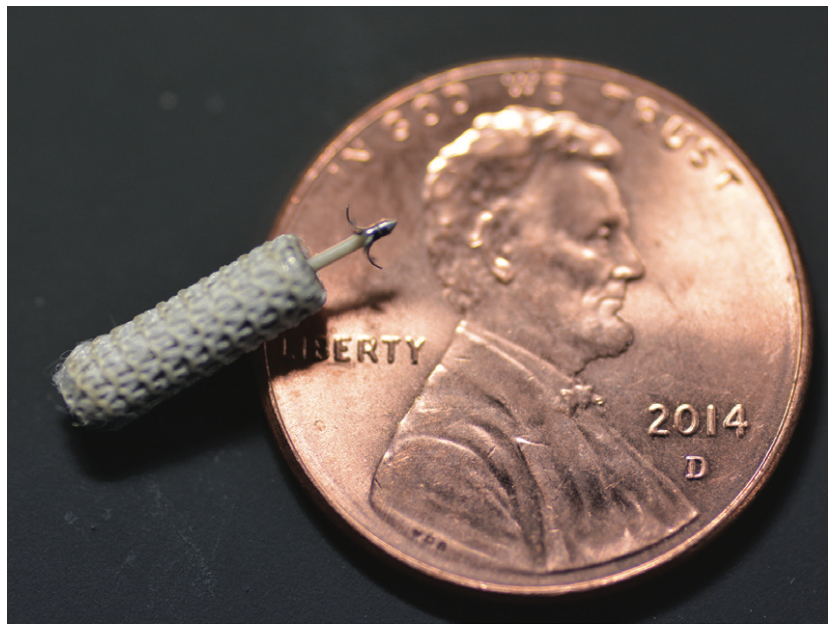
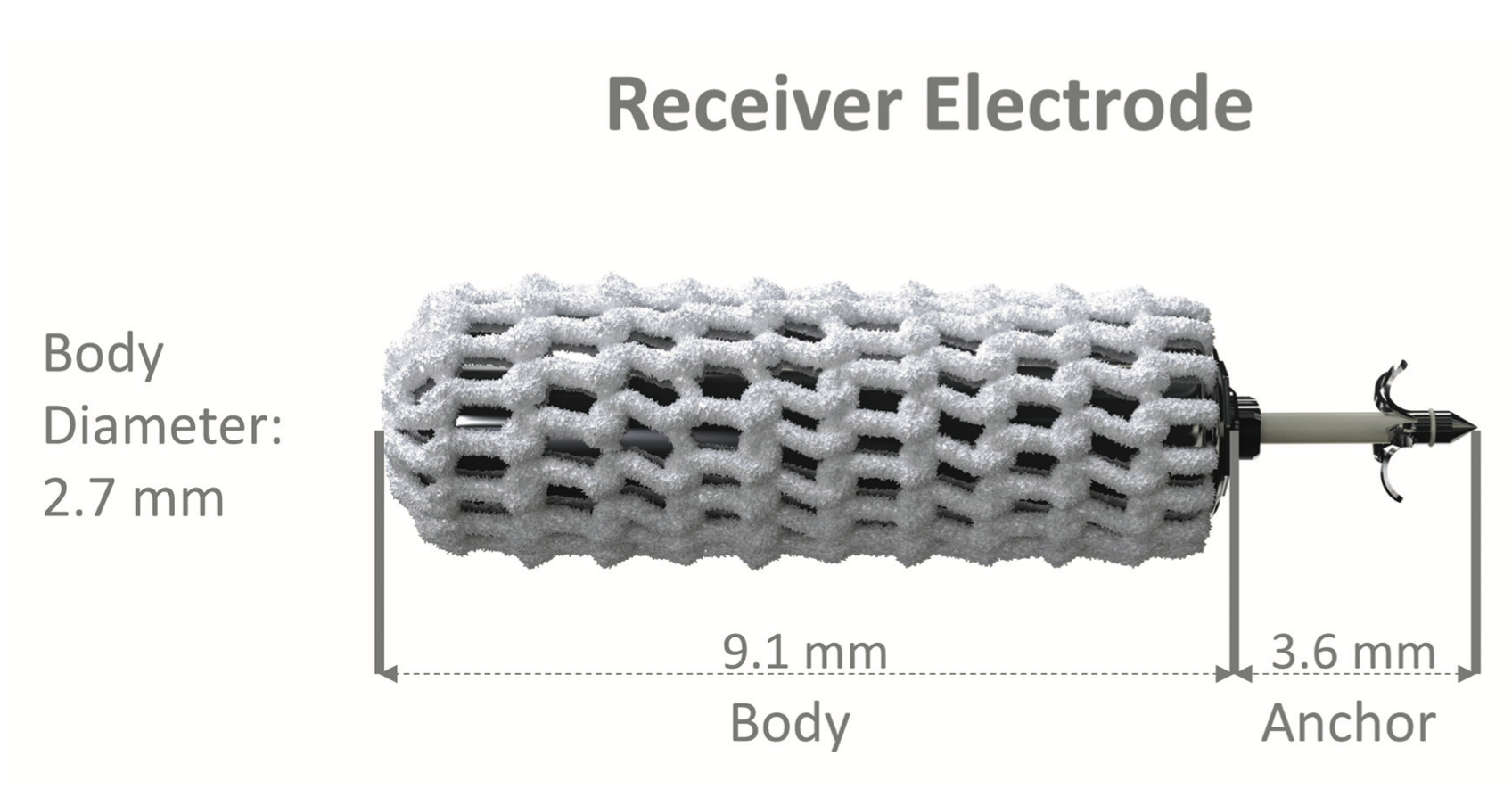
In this case, we used a retrograde aortic approach. We went through the femoral artery and the aortic valve and entered the LV to implant the electrode. With the WiSE CRT System, the electrode is the size of a grain of rice. It is implanted in the LV and stimulated by an ultrasound transmitter.
As the Micra paces the RV, the WiSE CRT System senses it and simultaneously paces the LV. It works by the transmitter sending an ultrasound wave to the electrode, which then converts this ultrasonic energy into an electric current.
Looking forward, what future applications of the WiSE CRT System do you believe could provide the most exciting patient benefits? What excites you most about the direction leadless pacing could take over the next 5+ years?
If, in the future, we can use the WiSE CRT System to reliably pace the His bundle or left bundle area, that would be a game-changer, because we will then have the benefit of physiological pacing. At the same time, patients will no longer need leads, which are the Achilles’ heel of the pacing system. That would be a win-win situation to no longer have leads and still provide physiological pacing. Regarding future applications of de novo implants of the WiSE CRT System implants with a leadless pacemaker to provide CRT to HF patients, if a defibrillator is not needed in those situations, using the WiSE CRT System combined with a leadless pacemaker would seem to be a very viable option. Finally, there is potential for combined use of the WiSE CRT System with a dual-chamber leadless pacing system, although that has not yet been done.
This article was published with support from EBR Systems, Inc.
Disclosures: Dr. Sharma has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. He has no conflicts of interest to report regarding the content herein.

