Peer Reviewed
Collagen Matrix and Staged Skin Grafting for Plantar Reconstruction: Lessons Learned in Treatment of Palmoplantar Keratoderma
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Background. Tissue defects of the weight-bearing surface of the foot are challenging wounds to reconstruct. Traditionally, skin grafting has had limited success in achieving both a durable and functional construct for ambulation. This case series describes a 2-staged approach to using a collagen bilayer matrix with subsequent skin grafting for plantar reconstruction in 3 sisters with palmoplantar keratoderma (PPK).
Methods. Outcomes of 3 patients (ages 7, 13, and 15 years) who underwent plantar excisions of both feet for treatment of PPK were reviewed retrospectively. Data collection included tissue defect size, duration of non-weight-bearing activity, skin grafting technique, surgical complications, incidence of graft loss, total inpatient stay, and long-term functional status. Sensory outcomes were measured using Semmes Weinstein monofilament testing, along with patient-reported outcomes utilizing the Manchester-Oxford Foot Questionnaire (MOXFQ).
Results. All 3 patients, totaling 6 feet, underwent plantar excisions of PPK. A collagen bilayer matrix was applied, followed by staged skin grafting (mean = 25.5 days between stages). Average total inpatient stay across treatment course was 2.6 days. There were 2 surgical site infections and 2 unanticipated returns to the operating room for excision of PPK recurrence. There were no incidences of graft loss. At an average of 6.9 years follow-up, all 3 patients had an intact reconstruction, preserved protective sensation, and normal gait and shoe-wear. Patient-reported ratings for foot pain varied from poor to excellent.
Conclusions. A method of plantar reconstruction utilizing a collagen bilayer matrix and staged skin grafting is presented, demonstrating excellent long-term durability and functional outcomes.
Introduction
Acquired plantar skin defects can have both acute and chronic etiologies, including trauma, burns, or post-extirpation of neoplastic and hypertrophic disease.1,2 Chronic trophic or neuropathic causes of plantar defects can be attributed to diabetes, leprosy, polyneuropathies, or other skin conditions.3,4 Soft tissue reconstruction of these defects remains a challenge in plastic surgery due to the difficulty in replacing the unique biomechanical and sensory characteristics of plantar skin that enable comfortable ambulation.5,6 Optimal reconstruction of the weight-bearing surface should be durable enough to withstand shearing forces under body weight while maintaining enough flexibility to allow normal range of motion. It should provide protective sensation without being hypersensitive or painful.7 Aesthetically, the reconstruction should be appropriately contoured without step-offs or excessive bulk to allow comfortable shoe-wear and should minimize disfigurement or alterations of skin color and texture.
Achievement of these functional ideals should be balanced against collateral morbidity from any donor sites while providing reproducible, predictable outcomes and minimizing overuse of medical resources. Traditional treatment approaches such as open wound care, secondary healing, and surgical reconstruction can be associated with prolonged course of treatment, high failure rates, ulceration, poor functional recovery, and/or significant donor site morbidity.1,8 Failed plantar reconstruction can result in prolonged treatment of persistent open wounds, creating a heavy cost burden on hospital, nursing, and wound care resources, as well as extensive periods of non-weight-bearing status on the part of the patient.9
The specific instance of subtotal or complete plantar skin loss, while rare, eliminates the option of a true like-with-like replacement using local flaps or glabrous skin graft10,11 since the surface area of a large wound exceeds available donor sites. Defects of this nature are typically treated with skin grafting when the tissue defect is pre-fascial.12 Skin grafting alone—whether split thickness, full thickness, or dermal—frequently fails as a long-term solution due to stiffness, hyperkeratosis, pain, breakdown, and/or ulceration of graft sites placed on the weight-bearing surface.12-15 Dermal substitutes, such as Apligraf16,17 or acellular dermal matrix,18 have been applied with variable success but have demonstrated drawbacks of requiring multiple product applications and prolonged time to wound closure.
For these reasons, continued refinements to treatment protocols and surgical techniques are needed. This case series presents a method of plantar skin reconstruction post-extirpation of palmoplantar keratoderma (PPK), utilizing a collagen-silicone bilayer matrix followed by skin grafting, and is the first to analyze surgical, functional, and patient-reported outcomes with long-term follow-up using this technique.
Methods
A single-surgeon case series of 3 sisters (totaling treatment of 6 feet) who underwent radical excision of debilitating, hyperkeratotic cutaneous disease due to PPK (Figure 1) from the plantar surface of the foot and subsequent tissue defect reconstruction was reviewed. All 3 patients involved in this study were sisters who were initially evaluated by a dermatologist and diagnosed with hereditary focal palmoplantar keratoderma. Their initial presentation revealed localized symptoms of hyperkeratotic scaling and thick plaques on their plantar surfaces, with palms and fingernails largely uninvolved. However, they developed palmar symptoms as their disease progressed. The patients had failed medical management using topical treatments, including lactic acid–based moisturizers and Urea cream, with minimal improvement of symptoms, ultimately resulting in referral to a plastic surgeon for surgical intervention. This case study outlines the reconstructive techniques used to address only the plantar presentation of PPK.
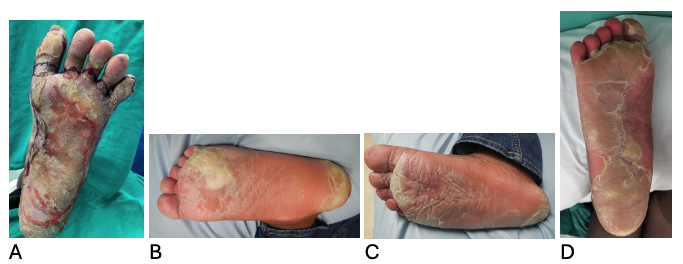
Figure 1. Preoperative photos of patient 1 (A), patient 2 (B, C), and patient 3 (D) demonstrating callus from palmoplantar keratoderma.
Data from the operative and postoperative course of each patient were collected retrospectively, including tissue defect size, duration of non-weight-bearing activity, skin grafting technique, surgical complications, unanticipated return to operating room, early (<30 days) or late (>30 days) incidence of graft loss, incidence of pressure ulceration, total inpatient length of stay, length of follow-up, and functional status following treatment. At final follow-up, sensory evaluation of each treated foot was measured using Semmes Weinstein monofilament testing, and patient reported outcomes were assessed utilizing the MOXFQ.19
Surgical technique
General considerations. All patients were fully evaluated and counseled in an office setting to determine their candidacy for surgical treatment of PPK disease, and an appropriate informed consent was obtained from patients and their parents (all patients were minors at the time of initial presentation) prior to all surgical procedures. Patients were treated in an operating room setting, under general anesthesia, with prone positioning and standard sterile technique. For each patient, 1 foot at a time was treated to allow the opposite foot to be available for weight support during the healing process. Patients were discharged home following most of the surgical procedures but were admitted to an inpatient setting at the discretion of the operating surgeon if it was deemed necessary for postoperative pain control, or to enable compliance with non-weight-bearing status on the operative foot. Prior to discharge, it was ensured that all patients had necessary durable medical equipment, such as a wheelchair or crutches, to aid in mobility at home.
Stage I. At the time of surgical excision, areas of planned tissue removal were identified and outlined. Early in the experience, only the most severe areas of callus were resected, in segments, sparing unaffected skin. Later, as it became apparent that unaffected areas were prone to disease, this approach gave way to a full en-bloc excision of all plantar skin, including both callus and unaffected adjacent areas of glabrous skin with disease potential. For all 3 patients, resection would eventually include complete forefoot, midfoot, and hindfoot subunits, with sparing of the high instep. A full-thickness excision of cutaneous tissue was performed under tourniquet in a subdermal plane down to normal, viable fibro-adipose subcutaneous tissue throughout the wound bed (Figure 2). Care was taken to removal all deep dermal appendages and callus, creating focal areas of excision that were down to plantar fascia. Tourniquet was released and hemostasis obtained with electrocautery.
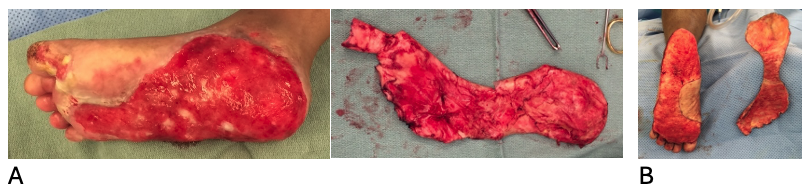
Figure 2. Full-thickness excisions of cutaneous tissue for patient 1 (A) and patient 3 (B).
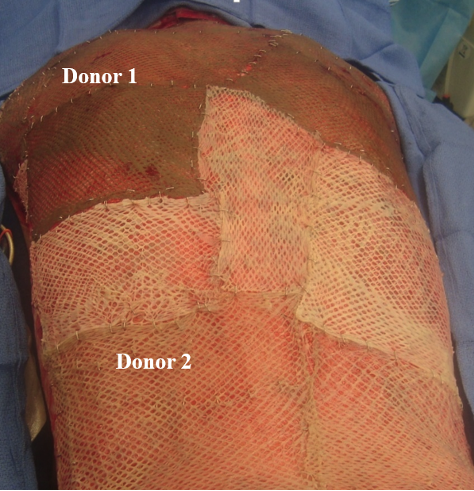
Next, bilayer wound matrix (Integra, Integra LifeSciences) consisting of collagen and laminated silicone was placed over the entire wound and custom trimmed to fit the edges, leaving the collagen layer interfaced to the tissue bed and silicone layer outward. The silicone portion of the bilayer was then fixed to the peripheral skin with monofilament suture. A non-adherent, protective bolster dressing was applied using a sliver silicone foam dressing (Mepilex Ag Transfer, Mölnlycke), gauze, cotton batting, and Coban wrap. Patients were instructed to remain non-weight-bearing on the operative foot and were seen in the office setting on a weekly basis for dressing changes and assessment of the collagen matrix.
Stage II. Approximately 3 to 4 weeks after stage I, once the collagen matrix appeared integrated based on adherence to the wound bed and pink salmon color (Figure 3), the patient was returned to the operating room for skin grafting. First, the outer silicone layer of the Integra was carefully lifted away. The surface of the collagen matrix was skimmed with the edge of a scalpel to remove superficial slough, biofilm, and loose debris, and dermal edges were freshened at the wound periphery. Following thorough antibiotic irrigation either a full-thickness skin graft or a .016- inch split-thickness skin graft (STSG) was harvested from an appropriate donor site. Both meshed and nonmeshed grafts were employed. All STSG were meshed to expand graft size, maximize area of coverage, and allow for egress of fluid. The graft was then inset with peripheral absorbable sutures, fixing the graft edge to the surrounding intact skin edge, along with quilting sutures to fix the graft to the wound bed. A standard bolster dressing was applied over a non-adherent interface, followed by cotton impregnated with mineral oil to maintain a moist environment, and ample cotton batting secured by Coban wrap. Patients were seen in the office for the first dressing change 5 to 7 days post-op, and twice-weekly dressing changes were provided by home health services for 2 to 3 weeks. Patients were instructed to remain non-weight-bearing on the operative foot until grafts had adequately taken to the wound bed.
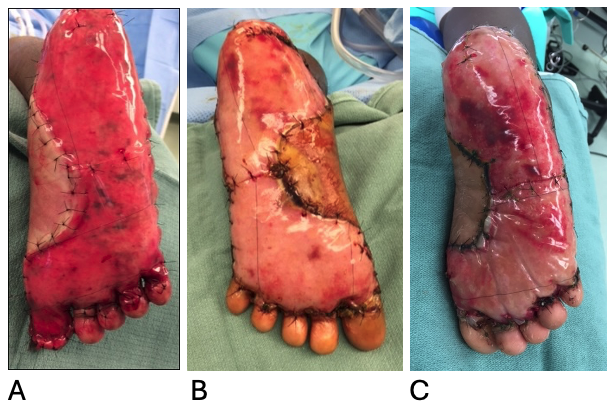
Figure 3. Appearance of fully integrated bilayer wound matrix, Integra on patient 1 (A), Patient 2 (B), and patient 3 (C).
Results
Patients 1, 2, and 3 were each African American females, ages 7 years, 13 years, and 15 years at time of presentation, respectively. All 3 patients were siblings with confirmed diagnosis of PPK who initially presented with complaints of large, painful, and thick keratinized calluses on much of the soles of their feet. Their condition had been diagnosed by dermatologists and progressed despite conservative treatment with topical medications, water soaks, and localized filing and debridement. Symptomatically, the lesions had become so severely tender on both feet that patients were unable to walk significant distances and were using a wheelchair for mobility upon referral for surgical evaluation. All 3 patients underwent surgical excision of affected skin and plantar reconstruction using a collagen matrix bilayer followed by a staged skin graft as described in the methods. The surgical technique and outcomes for each treated foot are summarized in Table 1.
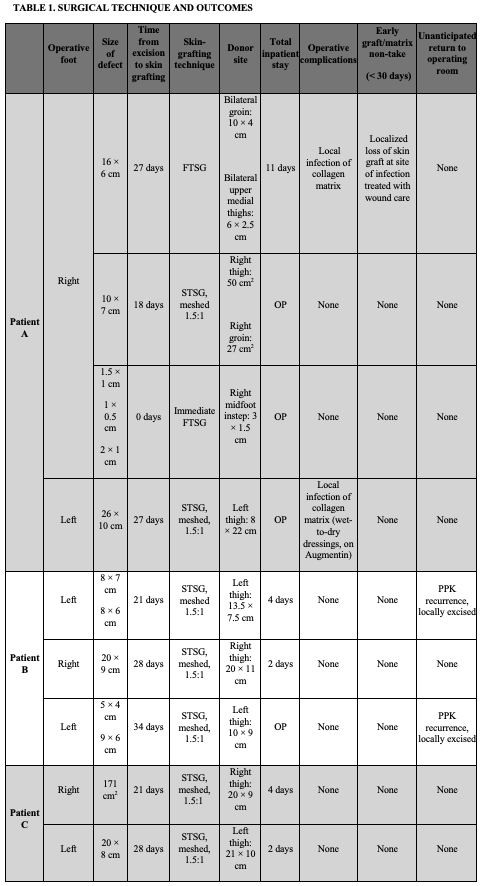
FTSG, full-thickness skin grafts; STSG, split-thickness skin grafts
The mean time between initial excision and collagen matrix application to skin grafting was 25.5 days. For each foot treated, total inpatient length of stay averaged 2.6 days through the entirety of the 2-stage process, and of the 18 operations performed for excision and grafting, 8 were accomplished on an outpatient basis.
STSG from the thighs were used in all cases except for the right foot in patient 1, where primarily full-thickness skin grafts (FTSG) were utilized. This was the first foot treated in the series, when the patient was 7 years old, and the plantar surface was sufficiently small enough that lower abdominal and groin donor sites covered the entire surface area of the initial excision defect. Subsequently, STSGs were chosen, as surface area coverage needs exceeded what could be taken with a full-thickness harvest. There were 2 surgical complications, both localized infections of the collagen matrix in patient 1, which were treated with local wound care and oral antibiotics. In one of these instances, there was a small segment of partial skin graft loss at the previous site of infection, which was allowed to heal secondarily. Otherwise, all 3 patients did not experience any additional skin graft loss.
There were 2 unanticipated returns to the operating room months after graft take, both for local excision of PPK recurrence at seams between graft sites on the left foot of patient 2, which had been treated at first with multiple segmental excisions rather than en-bloc excision and grafting of the entire plantar surface. In both cases, affected areas were small enough to be excised and closed primarily, without need for additional grafting. Patient 3, the third patient to be treated in the series, was treated with en-bloc excision of the entire plantar surface, covered by a single skin graft piece, avoiding seams, and did not have any need for return to the operating room once healed. Table 2 summarizes functional outcomes following completion of the 2-stage process.
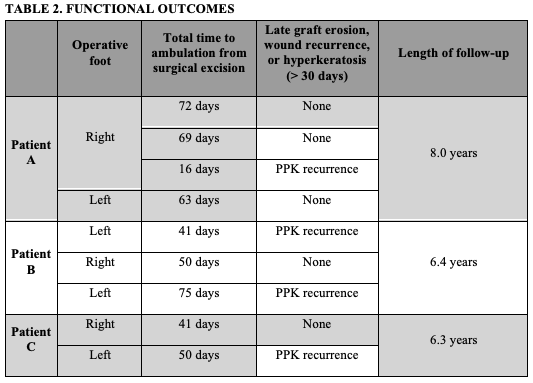
For each of the 9 sets of the 2-stage operations performed, total time from initial excision to unrestricted ambulation averaged 7.6 weeks (53 days). Throughout the follow-up period, each patient consistently reported improved levels of pain in their feet compared to pre-op, and upon completion of treatment, 3 were consistently able to ambulate comfortably in normal shoewear (Figure 4A). Other than minor noted recurrences of PPK and some callus formation in untreated areas outside of the graft sites, there were no reconstructive failures—defined as graft erosion, ulceration, open wound, or graft hyperkeratosis—during the follow-up period (Figure 4B).

Figure 4. Long-term reconstructive outcomes. Patient 3 at her 6.5-year follow-up wearing normal shoes (A). Patient 2 at her 6-year follow-up demonstrating minor recurrences of PPK and callus formation (B).
At an average of 6.9 years follow-up time, all 3 patients had an intact reconstruction at final visit. Patient-reported ratings for foot pain measured at the final follow-up visit using the MOXFQ survey were variable, with patients 1 and 2 reporting “moderate” pain “most of the time” in both feet, whereas patient 3 reported no foot pain. Of note, pain was attributed to areas of PPK recurrence outside of the grafted area when ambulating. All patients reported feeling self-conscious over shoe-wear “none of the time.” All 3 patients had preservation of protective sensation at final visit based on Semmes Weinstein testing of the plantar skin (Figure 5).
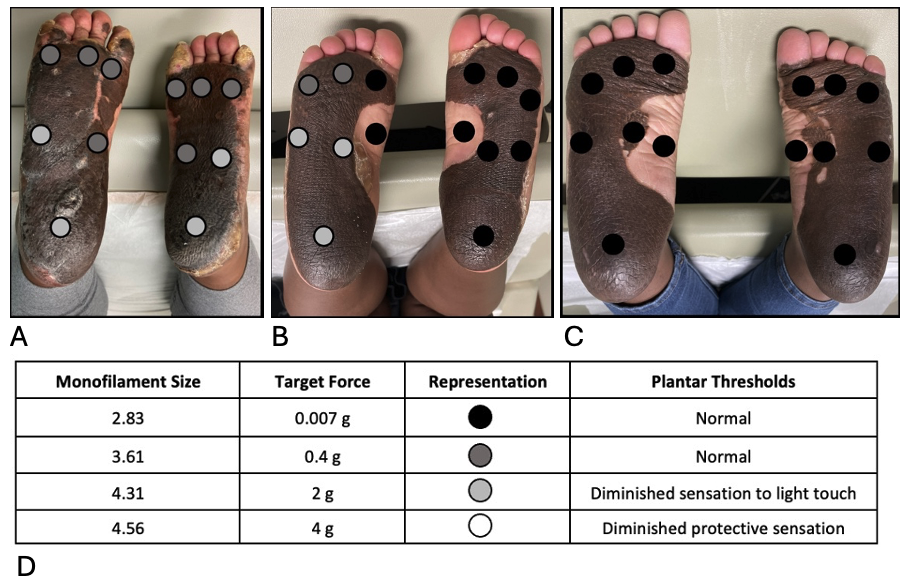
Figure 5. Semmes Weinstein monofilament testing on patient 1 (A), patient 2 (B), and patient 3 (C). Legend depicting test findings (D).
Discussion
This study presents a series of patients in which a collagen-silicone bilayer wound matrix was applied as an initial lamination to an acquired skin defect of the plantar surface, before placement of an autologous skin graft. Skin reconstruction with this method has been applied and long reported on in various contexts,20,21 with demonstrated reduced scar contraction of the skin graft and optimized elasticity and flexibility of the reconstructive site.21 This series is the largest experience, with the longest follow-up, in use of this specific technique for total plantar skin reconstruction in the literature, where only single-case reports without long-term follow-up previously existed.23,24 It is our observation that the construct of collagen matrix foundation under autologous skin graft produced a soft, flexible, durable, and optimally contoured final product that provided benefits for use in the foot.
The level of excision, and therefore the depth of tissue defect, in all 3 patients was into the subcutaneous layer, with preservation of the fibro-adipose tissue and plantar fascial layers. This technique is therefore offered as an alternative to other methods of supra-fascial plantar skin reconstruction, primarily single-stage split-thickness, full-thickness, dermal graft, and other dermal substitute options, whereas local-regional fasciocutaneous flaps, muscle flaps, and free tissue transfer would typically be reserved for subfascial defects with exposure of bone, joint, or tendon structures. Limitations of the study include its retrospective, small case-series design and lack of direct comparison or control group.
Despite these limitations, several observations can be made from the data about this surgical approach for plantar reconstruction. First, the use of a collagen matrix bilayer and staged skin grafting appears to be durable, as there were no major skin breakdowns, incidences of pressure ulceration, or need for repeat grafting, even years after surgical treatment (average follow-up 6.9 years). This approach also proved to be functionally sound in our series of patients. All 3 patients resumed normal ambulation without gait alteration or difficulty in shoe-wear, and this functional level was also maintained over many years. While this approach would not be an appropriate stand-alone choice if sensory restoration were called for, the reconstruction did not create a masking effect on sensory recovery in this series. Indeed, all 3 patients showed satisfactory preservation of protective sensation by Semmes Weinstein testing years after the initial procedures, which was likely key to avoidance of ulceration or breakdown of the reconstruction over time.
While the additional step of collagen bilayer placement adds time and expense to the initial process versus single-stage skin grafting, more study would be needed to determine if these upfront costs could be offset by improved durability and function over time. Aesthetically, this method had the drawback of hyperpigmentation on the plantar surfaces where the grafts were placed, and this was noted in the patient-reported measures. For smaller plantar defects, a glabrous skin donor site could be considered for optimized color match.10,11
The 2-staged approach calls for, at minimum, approximately 4 to 8 weeks of non-weight-bearing status, followed by graduated weight-bearing thereafter, once grafts have reached appropriate healing and maturity. Average non-weight-bearing period, which corresponded with time to wound closure in this study, was 7.6 weeks per excision. This timeframe compares favorably to average time to closure periods for various populations reported elsewhere in the literature: 18.2 weeks in diabetic plantar ulcers treated with skin grafts25; 65 days in pediatric patients with traumatic foot and ankle wounds treated with acellular dermal matrix, negative pressure wound therapy, and skin grafting26; and 65 days in non-infected, non-ischemic diabetic foot ulcers treated with living human skin equivalent.16 However, compared with other dermal substitute or biologic graft products, which can require multiple applications over weeks,16,26,28 the collagen-silicone bilayer only required a single application per wound in this series.
It is notable that the postoperative care process was refined such that the need for inpatient hospital stays was eliminated. Wound care protocols were simplified to minimize or even eliminate need for home-health resources, making this approach potentially appropriate for outpatient plastic surgical practices. The silicone layer of the collagen matrix provides a sealed, nonstick barrier over a sensate wound that virtually eliminates pain and blood loss associated with dressing changes, making them tolerable for the patient at the bedside and appropriate for the home or clinic setting. We chose a silver-impregnated silicone foam dressing (Mepilex Ag Transfer, Mölnlycke) as the interface dressing to the collagen-silicone bilayer because of its easy application as well as protective and antimicrobial properties. We found that this product did not adhere to the bilayer and could last for up to 1 week at a time to minimize dressing changes. Prolonged inpatient, microsurgical, and specialized wound care resources were not needed, making this treatment protocol potentially accessible to a larger pool of providers and minimizing need for transfer of care and patient travel to tertiary centers.
Over the course of developing this technique for these 3 patients, there were also key learning points that allowed for improvements in the treatment of the underlying PPK disease. First, en-bloc excisions of all plantar skin were superior to segmental excisions due to the high incidence of PPK recurrences with the latter. Secondly, PPK recurrences within treated areas tended to happen along seams between skin-grafted segments, so every attempt was made to cover a given defect with a single sheet rather than piecemeal. Later in the experience, this became a primary driver in the use of STSG to cover broader surface areas rather than small, pieced-together FTSG. More study would be needed to determine what, if any, advantage there is to using STSG to FTSG over the collagen matrix in a generalized population, since there was equivalency in take, durability, and sensory recovery between graft types in this small series.
Soft tissue reconstruction of the plantar region remains a challenge in plastic surgery due to the distinctive anatomy and weight-bearing nature of the foot. The described method of plantar soft tissue reconstruction outlines the operative details and postoperative outcomes of 3 sisters with palmoplantar keratoderma. All 3 patients demonstrated improvement from their preoperative baseline of being in chronic pain and wheelchair-bound. This case series describes the use of a collagen matrix bilayer and subsequent staged skin grafting and demonstrates a durable, reliable, and functional option for plantar reconstruction.
Acknowledgments
Authors: Joowon Choi, MBS, MD; Matthew Applebaum, MBA, MD; Mark Feldmann, MD
Affiliations: Virginia Tech Carilion School of Medicine, Carilion Clinic, Roanoke, Virginia
Correspondence: Joowon M. Choi; jmchoi@carilionclinic.org
Ethics: IRB-22-1555, all patients signed consent for release forms to allow use of photos and images presented in this paper.
Disclosures: The authors disclose no relevant financial or nonfinancial interests.
References
1. Jeng SF, Wei FC. Classification and reconstructive options in foot plantar skin avulsion injuries. Plast Reconstr Surg. 1997;99:1695-1703.
2. Goldberg DP, Kucan JO, Bash D. Reconstruction of the burned foot. Clin Plast Surg. 2000;27:145-161.
3. Kadam D. Microsurgical reconstruction of plantar ulcers of the insensate foot. J Reconstr Microsurg. 2016;32:402-410.
4. Patel S, Zirwas M, English, J.C. Acquired palmoplantar keratoderma. Am J Clin Dermatol. 2007;8:1-11..
5. Thoolen M, Ryan TJ, Bristow I. A study of the skin of the sole of the foot using high-frequency ultrasonography and histology. The Foot. 2000;10(1):14-17. doi:https://doi.org/10.1054/foot.1999.0568
6. Cavanagh, PR. Plantar soft tissue thickness during ground contact in walking. J Biomech. 1999 Jun;32(6):623-628.
7. Robbins S, Gouw GJ, McClaran J, Waked E. Protective sensation of the plantar aspect of the foot. Foot Ankle. 1993 Jul-Aug;14(6):347-352.
8. Roggero P, Blanc Y, Krupp S. Foot reconstruction in weight bearing area. Eur J Plast Surg. 1993;16:186-192.
9. Dischinger PC, Read KM, Kufera JA, et al. Consequences and costs of lower extremity injuries. Annu Proc Assoc Adv Automot Med. 2004;48:339-353.
10. Banis JC. Glabrous skin grafts for plantar defects. Foot Ankle Clin. 2001 Dec;6(4):827-837, viii.
11. Wu LC, Gottlieb LJ. Glabrous dermal grafting: a 12-year experience with the functional and aesthetic restoration of palmar and plantar skin defects. Plast Reconstr Surg. 2005 Nov;116(6):1679-1685.
12. Crowe CS, Cho DY, Kneib CJ, Morrison SD, Friedrich JB, Keys KA. Strategies for reconstruction of the plantar surface of the foot: a systematic review of the literature. Plast Reconstr Surg. 2019 Apr;143(4):1223-1244.
13. Ramanujam CL, Han D, Fowler S, Kilpadi K, Zgonis T. Impact of diabetes and comorbidities on split-thickness skin grafts for foot wounds. J Am Podiatr Med Assoc. 2013 May-Jun;103(3):223-232.
14. Wexler MR, Barlev A, Peled IJ. Plantar split-thickness skin grafts for coverage of superficial pressure ulcers of the foot. J Dermatol Surg Oncol. 1983 Feb;9(2):162-164.
15. Yan H, Liu S, Gao W, Li Z, Chen X, Wang C, Zhang F, Fan C. Management of degloving injuries of the foot with a defatted full-thickness skin graft. J Bone Joint Surg Am. 2013 Sep 18;95(18):1675-1681.
16. Veves A, Falanga V, Armstrong DG, Sabolinski ML; Apligraf Diabetic Foot Ulcer Study. Graftskin, a human skin equivalent, is effective in the management of noninfected neuropathic diabetic foot ulcers: a prospective randomized multicenter clinical trial. Diabetes Care. 2001 Feb;24(2):290-295.
17. Karr J. Utilization of living bilayered cell therapy (Apligraf) for heel ulcers. Adv Skin Wound Care. 2008 Jun;21(6):270-274.
18. Bingol UA, Cinar C, Arslan H, Altındas M. A novel and alternative treatment method for diabetic heel ulceration exposing the calcaneus which is not suitable for flap surgery: vacuum assisted sandwich dermal matrix. Biomed Res Int. 2015;2015:785819.
19. Morley D, Jenkinson C, Doll H, Lavis G, Sharp R, Cooke P, Dawson J. The Manchester-Oxford Foot Questionnaire (MOXFQ): development and validation of a summary index score. Bone Joint Res. 2013 Apr 3;2(4):66-69.
20. Suzuki S, Matsuda K, Isshiki N, Tamada Y, Yoshioka K, Ikada Y. Clinical evaluation of a new bilayer "artificial skin" composed of collagen sponge and silicone layer. Br J Plast Surg. 1990 Jan;43(1):47-54.
21. Burke JF, Yannas IV, Quinby WC Jr, Bondoc CC, Jung WK. Successful use of a physiologically acceptable artificial skin in the treatment of extensive burn injury. Ann Surg. 1981 Oct;194(4):413-428.
22. Min JH, Yun IS, Lew DH, Roh TS, Lee WJ. The use of matriderm and autologous skin graft in the treatment of full thickness skin defects. Arch Plast Surg. 2014 Jul;41(4):330-336.
23. Asif M, Ebrahim S, Major M, Caffrey J. The use of IntegraTM as a novel technique in deep burn foot management. JPRAS Open. 2018 Jun 14;17:15-20.
24. Nusbaum AG, Martell EG, Bard S, Connelly EA, Thaller SR. Excision and grafting of palmoplantar keratoderma. J Craniofac Surg. 2009 Nov;20(6):2241-2243.
25. Walters ET, Pandya M, Rajpal N, et al. Long term outcomes of split-thickness skin grafting to the plantar foot. J Foot Ankle Surg. 2020 May-Jun;59(3):498-501.
26. Hutchison RL, Craw JR. Use of acellular dermal regeneration template combined with NPWT to treat complicated extremity wounds in children. J Wound Care. 2013 Dec;22(12):708-712.
27. Garoufalis M, Tettelbach W. Expandable dehydrated human umbilical cord allograft for the management of nonhealing lower extremity wounds in patients with diabetes: a case series. Wounds. 2022 Sep;34(9):E91-E95.
28. Hawkins B. The use of micronized dehydrated human amnion/chorion membrane allograft for the treatment of diabetic foot ulcers: a case series. Wounds. 2016 May;28(5):152-157.