Outcomes of Complex Wound Reconstruction in High-Risk Patients Using Decellularized Extracellular Matrix from Porcine Urinary Bladder
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Background. The treatment of complex wounds remains a challenging aspect of reconstructive surgery, given their diverse nature and the frequent need for high-level surgical procedures. Standard treatment with flap coverage can achieve many goals; however, it is not without difficulties, including technical complexity, extended recovery times, donor site morbidity, and vascular complications, particularly in non-optimized patients. Acellular extracellular matrices, such as porcine urinary bladder matrices, have emerged as an alternative approach to support wound healing without the risks of high-level reconstruction. Urinary bladder matrix provides an extracellular matrix scaffold that supports intrinsic tissue regeneration mechanisms, allowing for stable, well-vascularized wound bed formation.
Methods. This retrospective case series examines the outcomes of urinary bladder matrix for the treatment of complex wounds in 21 patients deemed high-risk or unfavorable candidates for surgical management with local or free flap techniques. The patients were treated by 2 surgeons at 2 separate level 1 trauma centers from October 2019 through June 2022. Urinary bladder matrix was the primary wound management modality with serial wound debridement, matrix reapplication, and subsequent wound care tailored to each patient until definitive, stable coverage.
Results. In all cases, urinary bladder matrix facilitated soft tissue remodeling, permitting complete wound re-epithelization or preparation for skin grafting and/or flap coverage. Four patients’ wounds re-epithelized on their own, while 17 patients received subsequent skin graft. In 2 of these cases, the initial split-thickness skin graft failed, requiring a second skin graft and or/flap coverage.
Conclusions. Our results demonstrate that urinary bladder matrix facilitates definitive soft tissue reconstruction and can be a valuable adjunct to wound repair, providing a simpler, less morbid treatment option for patients with various comorbidities and injury mechanisms.
Introduction
The reconstructive ladder has historically guided wound coverage decisions, endorsing the simplest method of coverage that meets defect requirements.4 Injuries involving large or multilayer defects are generally addressed by increasingly complex rungs on the ladder, ranging from skin grafts to free vascularized tissue transfer. Each of these rungs has their own benefits and challenges. Skin grafting can be utilized for well-vascularized defects that are too large for primary closure but are not amenable to wounds with exposed tendons, bones, or neurovascular structures.5 Local pedicled flaps can address small- and medium-sized defects by providing durable tissue with minimized donor-site morbidity and without the need for a large donor vessel; however, they are associated with higher complication rates, particularly partial flap necrosis and venous congestion.6-14 Free tissue transfer has become the predominate treatment modality for injuries with extensive soft tissue damage or exposed vital structures as it provides multicomponent replacement of damaged or lost tissues. Yet, free flaps are technically difficult and time intensive and may not be a feasible option at many institutions.15,16 Even when available, failure rates range from 3.2% to 8.5%, resulting in increased resource utilization and morbidity for take-back procedures or additional salvage surgeries.17,18
Given the challenges faced in the reconstruction of complex wounds, there is an interest in techniques that support healing without the risks associated with higher rungs of reconstruction. Acellular extracellular matrix (ECM) products, including acellular dermal matrices (ADMs), augment the traditional reconstructive ladder and can allow for simplified approaches to difficult wounds. Rather than replacing lost tissue, acellular ECMs support intrinsic tissue regeneration by providing an ECM scaffold. When implanted in the injury site, the ECM provides a framework for the tissue to remodel into a stable, vascularized wound bed, allowing for re-epithelization or secondary coverage.19 Current data support the use of acellular ECM products in injuries with exposed vital structures, sparing the morbidity of complex flap reconstruction.20,21 This may be an effective treatment option for patients who are not good candidates for flaps or traditional reconstructive techniques.
Urinary bladder matrix (UBM) is a type of acellular ECM derived from decellularized porcine urinary bladder. UBM products are available as a single-layer sheet or micronized particulate. Sheet UBM is favorable for partial-thickness wounds, while micronized UBM is favorable for full-thickness deficits with exposed organ structures due to its increased surface area.22 There is a growing body of literature evaluating UBM as an adjunct to wound repair. Various case reports have shown successful applications of UBM in difficult to heal wounds such as combat casualty wounds,23 radiation wounds,24,25 a wide variety of open wounds including degloving injuries,26-28 deep partial-thickness burns,29 and chronic diabetic wounds.30-33 In the present clinical case series, we report clinical outcomes of UBM application for treatment of complex wounds in patients with various comorbidities and injury mechanisms.
Methods and Materials
From October 2019 through June 2022 a total of 21 patients with complex wounds were treated by 2 surgeons at 2 separate level 1 trauma centers. Porcine UBM (MicroMatrix, Cytal Wound Matrix, and Cytal Burn Matrix, ACell Inc; acquired by Integra LifeSciences in 2021) were used as the primary wound management modalities. Despite resources available for microsurgical reconstruction, the surgeons elected to use this technology due to the depth and complexity of wounds in patients with multiple medical comorbidities that were deemed high-risk or unsuitable candidates for routine surgical management with local or free flap techniques.
Treatment protocols entailed irrigation and debridement (I&D) to remove debris and necrotic or infected tissue before reconstruction. Further reconstruction was planned at the discretion of the operating surgeon. Micronized powder (MicroMatrix) and/or sheet (Cytal Wound or Burn Matrices) UBM materials were applied separately or in combination to each wound bed. Timing of application, type(s) of UBM used, and wound care strategies were determined by the surgeon according to specific needs and reconstructive goals for each patient. Water-soluble gel and Xeroform were placed over the UBM product(s) and covered with a soft sterile dressing or wound vac. Subsequent wound care included negative pressure wound therapy and routine dressing changes. Serial surgical irrigation and debridement procedures were performed as necessary until the patient’s wounds were amenable to definitive reconstruction. In larger wounds where primary skin closure or re-epithelization was not feasible, some patients received a partial- or full-thickness skin graft to attain final coverage once wound volume was restored and well-vascularized. Demographic data, medical comorbidities, injury characteristics, and treatments utilized for each patient are summarized in the Table.
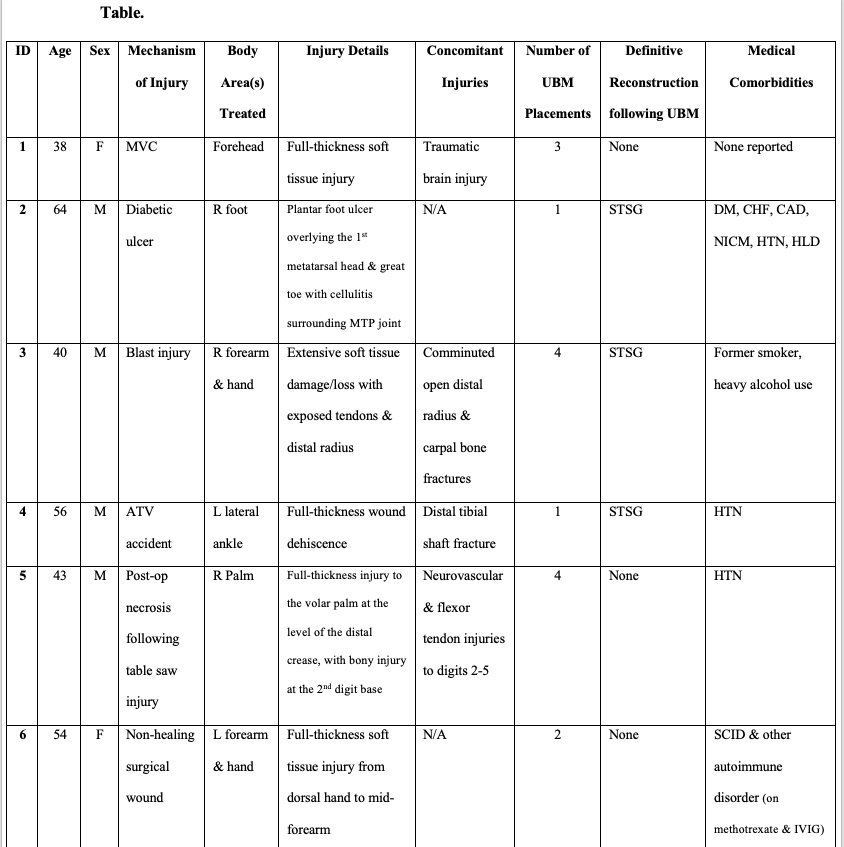
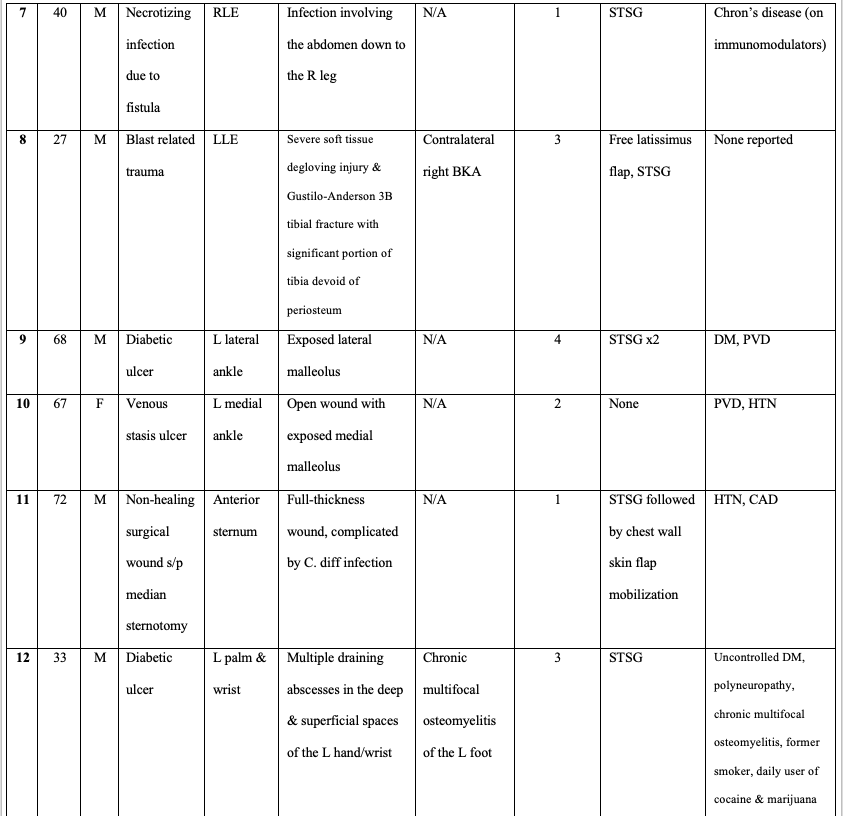
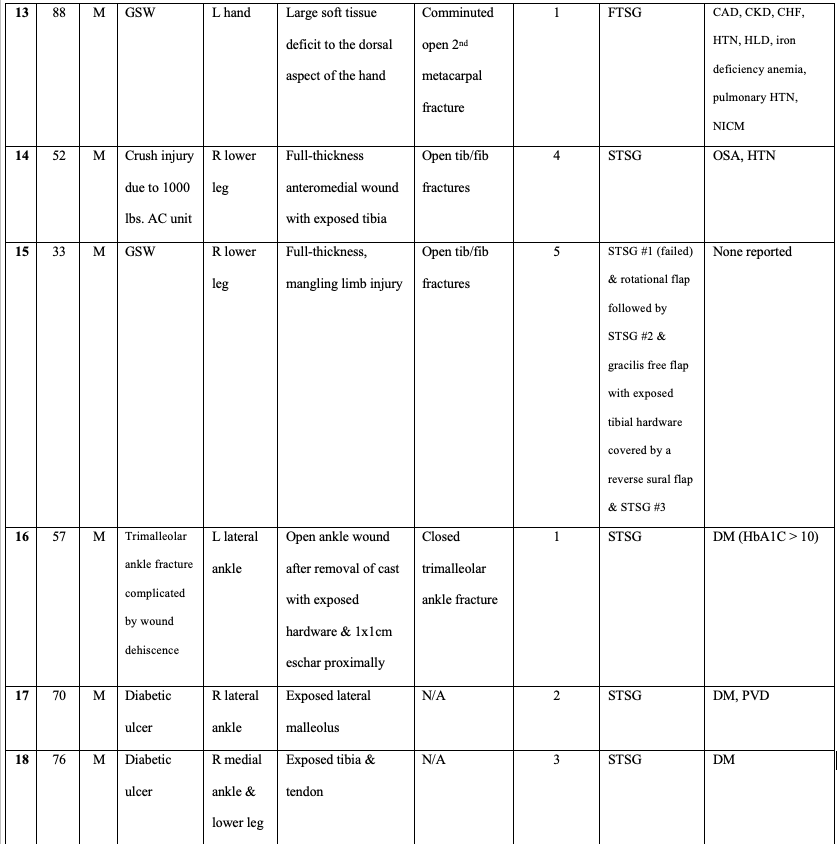
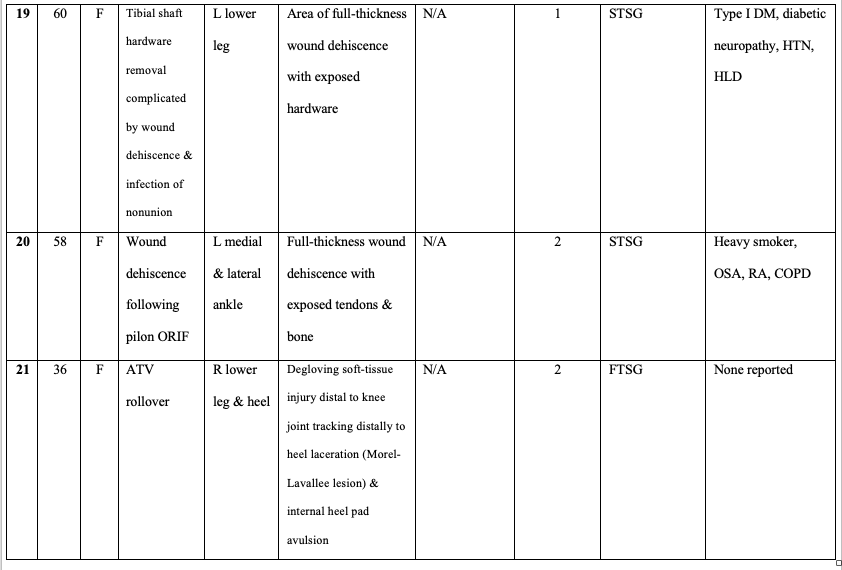
AC unit, air conditioning unit; ATV, all-terrain vehicle; BKA, below knee amputation; CAD, coronary artery disease; CHF, congestive heart failure; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DM, diabetes; FTSG, full-thickness skin graft; GSW, gunshot wound; HLD, hyperlipidemia; HTN, hypertension; MVC, motor vehicle collision; NICM, nonischemic cardiomyopathy; ORIF, open reduction and internal fixation; OSA, obstructive sleep apnea; PVD, peripheral vascular disease; RA, rheumatoid arthritis; SCID, severe combined immune deficiency; STSG, split-thickness skin graft; UBM, urinary bladder matrix.
Results
In total, 21 cases were included in our series. Patient and injury characteristics as well as treatment algorithms for each are shown in the Table. Clinical images were compiled for each patient, showing the progression from time of injury to final healing. Images for patients 1 through 16 were included (Figures 1-16) with corresponding videos for patients 1 and 15. The average patient age was 53.9 years (range: 27-88) and 71.4% were male. All but 4 patients had comorbidities known to impair wound healing, and many patients had multiple risk factors that made them poor candidates for traditional reconstructive methods.
The average number of serial UBM placements (sheet matrix and/or micronized powder) was 2.38 (range: 1-5). In all cases, UBM stimulated formation of healthy granulation tissue and/or facilitated wound bed preparation for secondary skin grafting and/or flap coverage. Four patients’ wounds re-epithelized on their own without requiring secondary coverage. Seventeen patients had skin grafting following treatment with UBM products. In 2 of these cases (patients 9 and 15), the initial split-thickness skin graft (STSG) did not take to the entire wound bed, requiring a second skin graft and or/flap coverage. While data for all 21 cases has been summarized in the Table, details from 5 representative cases are presented below to provide a more robust clinical context for a variety of wound presentations.
Case 1
A 38-year-old healthy female was involved in a motor vehicle collision, sustaining a full-thickness soft tissue injury to the forehead area in addition to a traumatic brain injury (Figure 1A). After I&D and initial micronized UBM powder application, the patient’s forehead had exposed calvarium, no periosteum, and loss of frontalis muscle (Figure 1B). The patient underwent a second micronized UBM powder application, with a UBM sheet matrix sheet sewn over (Figure 1C). Overall, it took 8 weeks for the full-thickness wound to epithelialize, and no grafting was required. The resulting product is cosmetically appealing with restored musculature function of sensitive area (Figure 1E).
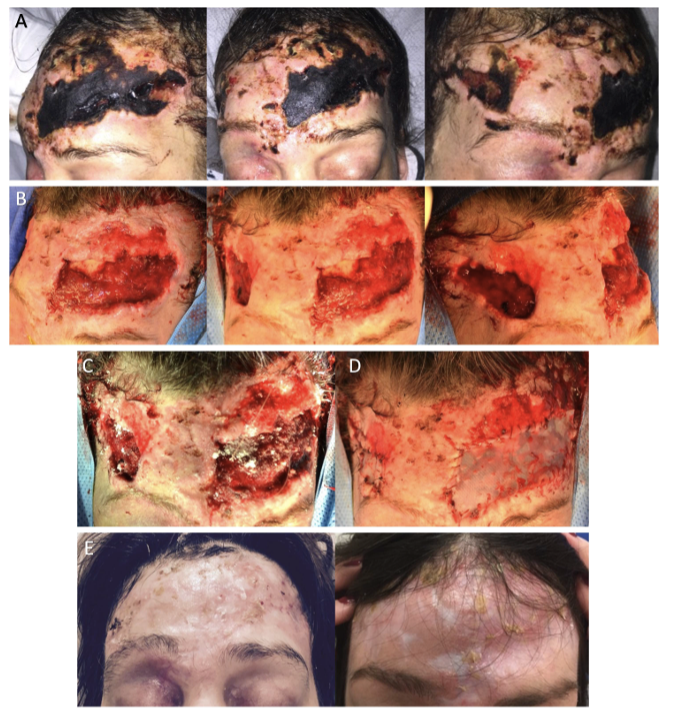
Figure 1. A 38-year-old healthy female involved in a motor vehicle collision sustained a traumatic brain injury and a full-thickness soft tissue injury to the forehead. (A) Initial wound with eschar formation. (B) Following I&D and initial micronized UBM powder application, revealing exposed calvarium with no periosteum and loss of frontalis muscle. (C) Second UBM powder application. (D) Third UBM powder application, covered with a UBM wound matrix sheet. (E) Six-month follow-up showing full re-epithelialization without secondary grafting.
Video 1. Demonstrates functional recovery of the forehead region with good gliding function.
Case 2
A 64-year-old male with multiple medical comorbidities (DM, hypertension, hyperlipidemia, CAD, congestive heart failure, and cardiomyopathy) presented to the hospital with a chronic diabetic foot ulcer of the plantar right foot overlying the first metatarsal head and an ulcer over the plantar aspect of the great toe with associated osteomyelitis. He had associated cellulitis surrounding the toe and the metatarsophalangeal (MTP) joint as well as fluctuance consistent with an abscess. Amputation of the great toe at the MTP joint was performed followed by copious I&D. Four days later, a trans-metatarsal amputation of the first and second ray was performed (Figure 2A). The patient returned for repeat I&D 30 days later where 14 cm of the wound was closed, leaving a 7 × 3 × 2-cm wound open in the middle of the incision (Figure 2D). This was packed with 500 mg of micronized UBM powder and covered with a 5 × 5-cm UBM sheet matrix bilayer. This healed to a 6 × 3-cm partial-thickness wound with a healthy granulation tissue bed that was covered with a STSG from the proximal thigh 6 weeks later (Figure 2H). Nine weeks after the STSG, the wound size and drainage had greatly decreased. The patient noted that he would occasionally see a scant amount of clear fluid on his dressing during changes (Figure 2K). The patient returned 29 weeks after the STSG, and the wound was well healed (Figure 2L).

Figure 2. A 64-year-old male with a chronic diabetic foot ulcer over the plantar right foot at the first metatarsal head and plantar great toe with osteomyelitis. The patient underwent amputation of the great toe at the metatarsophalangeal joint, followed by copious I&D. (A) Four days later, a transmetatarsal amputation of the first and second ray was performed. (B, C) Images at 1 and 2 weeks postoperatively. (D) One month later, repeat I&D was performed, closing 14 cm of the wound, leaving a 7 × 3 × 2 cm wound open in the middle of the incision, packed with 500 mg of UBM powder and covered with a 5 × 5 cm UBM sheet matrix bilayer. (E-G) Incremental healing at 10 days, 24 days, and 5 weeks post-UBM application. (H) At 6 weeks post-UBM, a STSG from the proximal thigh was applied. (I, J) Images at 4 days and 7 weeks post-STSG. (K) At 9 weeks post-STSG, the wound size and drainage decreased. (L) At 38 weeks post-STSG, the wound was healed with a central crusted lesion remaining.
Case 3
A 40-year-old male who was a former smoker sustained a firework injury to the right hand from an artillery shell. This resulted in a comminuted, open distal radius fracture, initially fixated with an external fixator, and carpal bone fractures. He underwent 2 I&D procedures followed by wound vac placement prior to a radiocarpal fusion with bone graft application to the large bony defect of the radius. During this procedure, 500 mg micronized UBM powder, a 10 × 15-cm UBM 3-layer sheet matrix, and a wound vac were applied to the wound (Figure 3A, 3B). Two weeks later, the patient underwent subsequent I&D and a second application with UBM powder covered with a 2-layer sheet matrix and wound vac (Figure 3C, 3D). I&D to the muscle was repeated 3 weeks later, and the deep portion of the wound was filled with UBM powder and covered by a 10 × 12-cm sheet of Integra and wound vac (Figure 3F). Four weeks later, the final I&D procedure with placement of UBM powder surrounding the exposed tendon was performed followed by a STSG and wound vac (Figure 3G). Eight weeks after the final UBM placement and STSG, the patient had returned to work and was pleased with the improvement in range of motion (Figure 3I). The wound was fully healed 16 weeks after the final UBM placement and STSG (Figure 3J).
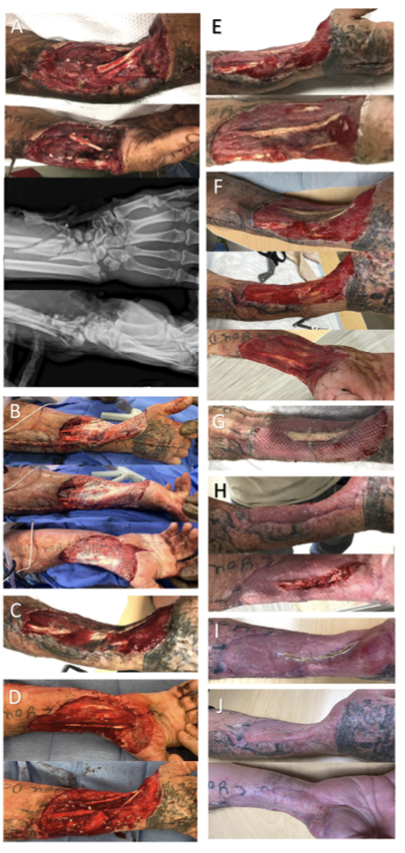
Figure 3. A 40-year-old male sustained a firework injury to the right hand, resulting in a comminuted, open distal radius fracture and carpal bone fractures. (A) Initial I&D with wound VAC placement. (B) One week later, a second I&D and radiocarpal fusion with bone grafting; 500 mg of UBM powder, a 10 × 15-cm UBM 3-layer sheet matrix, and a wound VAC were applied. (C, D) Images at 2 weeks and after a second I&D and UBM application. (E) One week later. (F) Two weeks later, another I&D (11 × 10 × 1 cm), UBM powder, and a 10 × 12-cm sheet of Integra and wound VAC application. (G) Four weeks later, I&D with UBM powder placement over the exposed tendon, followed by STSG and wound VAC. (H) Four weeks post-final UBM placement and STSG. (I) Eight weeks post-final UBM placement and STSG. (J) Wound fully healed at 16 weeks.
Case 4
A 56-year-old male with HTN was involved in an all-terrain vehicle accident. He sustained a closed, left distal tibial shaft fracture that was initially stabilized with a spanning delta frame external fixation device, then converted to open reduction and internal fixation (ORIF) 16 days later. Four weeks following ORIF, the patient presented with full-thickness wound dehiscence (3 × 10 cm) over the fracture site. He underwent I&D of the lateral ankle involving skin, dermis, subcutaneous tissue, muscle, fascia, and bone, and the site was covered with a wound vac (Figure 4A). Three weeks following the second I&D procedure, 500 mg micronized UBM powder and a 10 × 15-cm UBM 3-layer sheet matrix were placed in the wound and covered with a wound vac (Figure 4B). Nearly 3 months later, the patient underwent I&D and placement of STSG from his left thigh (Figure 4F). One month later, the wound was healed with no drainage and a healthy skin graft. The patient was able to ambulate with minimal soreness to the ankle at this time (Figure 4h).
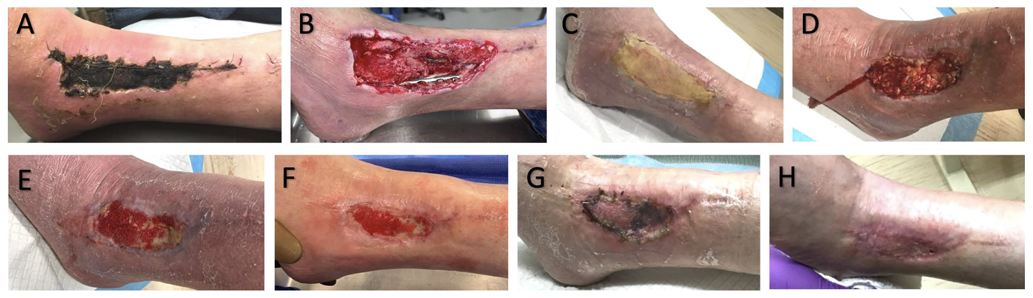
Figure 4. A 56-year-old male involved in an all-terrain vehicle accident sustained a closed left distal tibial shaft fracture. (A) Four weeks after ORIF, the patient presented with a necrotic wound over the lateral ankle fixation site requiring I&D (3 × 10 cm) and wound VAC application. (B) Three weeks later, 500 mg of UBM powder and a 10 × 15-cm UBM 3-layer sheet matrix were applied with wound VAC. (C-E) Images at 4, 6, and 8 weeks post-UBM. (F) At 11 weeks post-UBM, the patient underwent I&D and STSG. (G) One week post-STSG. (H) Five weeks post-STSG (17 weeks post-UBM), the wound was healed with no drainage and a healthy skin graft.
Case 5
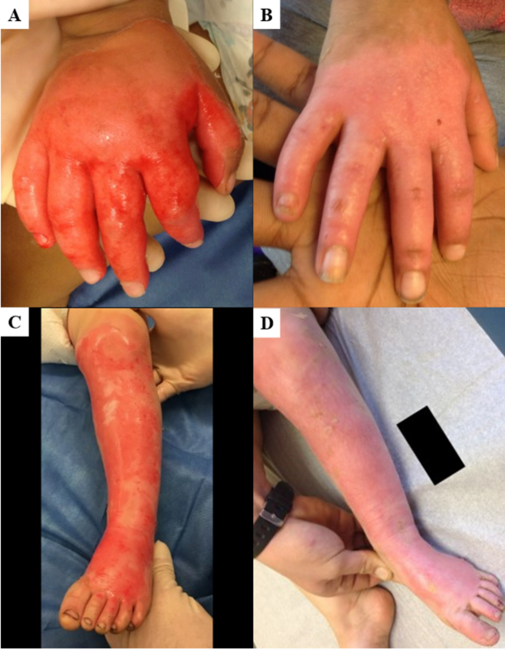
A 43-year-old, right-handed male sustained a table saw injury to the right volar palm at the level of the distal crease, with bony injury to the base of the right index finger and neurovascular injuries to the index, middle, ring, and small fingers (Figure 5A, 5B). The patient had a history of HTN but no other intrinsic risk factors for wound complications. Initially, 2 revascularization procedures; ORIF of the second metacarpal fracture; nerve repair with conduits for the digital nerves; repair of the flexor tendons in zone 2 to the index, middle, ring, and small fingers; and zone 5 extensor tendon repair of the index finger were performed (Figure 5C). Two weeks postoperatively, the wound had necrosis ranging from epidermolysis to full-thickness skin necrosis along the central portion, with no evidence of infection requiring repeat I&D. The proximal aspect of the wound was closed with interrupted prolene suture, but the remainder of the wound was not amenable to closure and was treated with topical application of micronized UBM powder followed by application of a 5 × 7-cm UBM sheet matrix (Figure 5D, 5Ee). UBM powder and sheet application was repeated 1, 2, and 3 weeks later (Figure 5F-5I).
At 6 weeks post-UBM application, there was near-complete closure of the palmar wound with no evidence of infection or necrosis (Figure 5K). At 5 months, all wounds were completely healed, and sensation had returned in the small and index fingers (Figure 5P). It was determined that the patient was able to pass functional requirements to return to work. At 6 months, the patient returned to full duty at manual construction work and reported continued improvements in function. At 1-year follow-up, the patient’s wounds were completely healed with limited scarring (Figure 5S). All fingers were vascularly intact with full sensation to the median, radial, and ulnar nerve distributions. There was some scar contracture in the small and long digits; however, since he had returned to full work and activity without pain or functional deficits, the patient elected to forgo contracture release.

Figure 5. A 43-year-old right-handed male sustained a table saw injury to the right volar palm at the distal crease. (A-C) Initial procedures included 2 revascularization procedures, ORIF of the second metacarpal fracture, digital nerve repair, and tendon repairs. (D, E) Two weeks postoperatively, the wound had central necrosis requiring I&D. The proximal wound was closed with interrupted prolene suture, while the remainder was treated with UBM powder followed by a 5 × 7-cm UBM sheet matrix. (F-I) Weekly UBM powder and sheet applications. (J) Four weeks post-UBM. (K) Six weeks post-UBM, showing near-complete closure without infection or necrosis. (L-O) Healing progression at 9 and 13 weeks. (P) At 5 months, all wounds were healed with restored sensation in the fourth and fifth digits. (Q, R) At 6 months, the patient returned to full manual labor. (S) One-year follow-up showed complete healing, limited scarring, and vascular integrity.
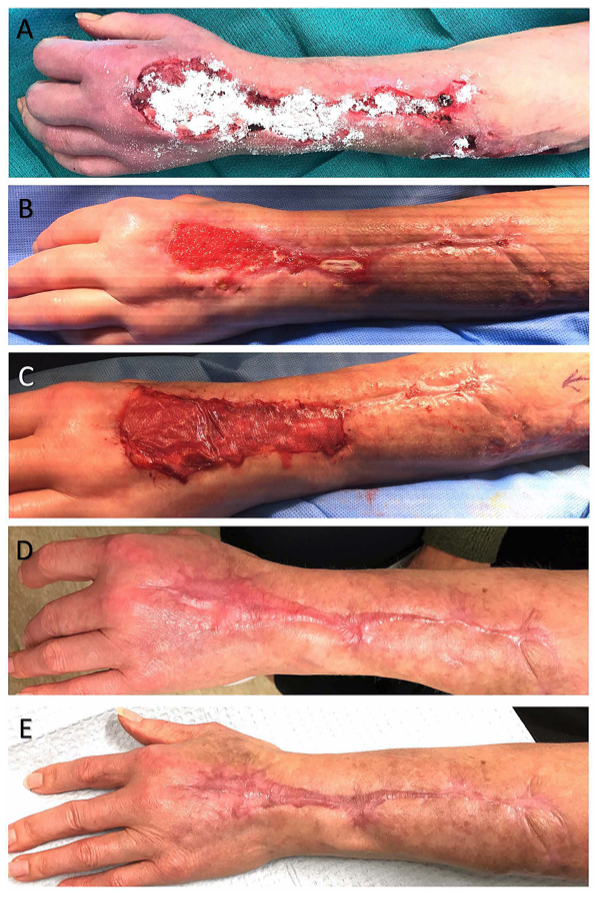
Figure 6. A 54-year-old female with severe combined immunodeficiency and an autoimmune disease on methotrexate presented with a nonhealing surgical wound. (A) After first I&D with UBM powder application. (B) Two weeks later. (C) UBM powder and 3-layer UBM sheet matrix application intraoperatively. (D) Three months later, showing a healthy wound bed. (E) Three years post-treatment.

Figure 7. A 40-year-old male with Crohn disease developed a fistula with necrotizing infection involving the abdomen and right leg. After multiple surgical debridements, the wound was treated in a single stage with UBM powder over the knee and posterior exposed tendon, followed by a single-layer Integra matrix and STSG. One-year follow-up showed wounds healed within 6 to 8 weeks.

Figure 8. A 27-year-old male sustained a left lower extremity blast-related trauma with a Gustilo-Anderson type 3B tibial fracture and extensive periosteal loss. (A) Fully debrided wound exposing the tibia. (B) Exposed tibia with absent periosteum. (C) Identification of vessel loops before reconstruction. (D) Hybrid reconstruction using latissimus dorsi free flap for superior coverage, serial UBM application, and Integra bilayer for the distal third of the tibia. (E) Initial post-reconstruction. (F) Four weeks post-reconstruction with well-vascularized tissue. (G) Four weeks post-STSG application, demonstrating coverage over hybrid reconstruction with serial UBM and Integra placement.

Figure 9. A 68-year-old male with a left lateral ankle wound due to a diabetic ulcer. (A, B) Initial wound with I&D and application of UBM powder and a 3-layer UBM sheet matrix. (C) Following the first application, granulation tissue formation covered exposed bone. A second UBM application was performed. (D) Repeat I&D and UBM placement with subsequent skin grafting. (E) The skin graft integrated around the wound margin but failed centrally. (F) The central wound was re-grafted 2 weeks later. (G) UBM powder was applied in the clinic 2 to 4 weeks later. (H) One month post-UBM powder application. (I) Two-year follow-up demonstrating complete epithelialization with no exposed bone.
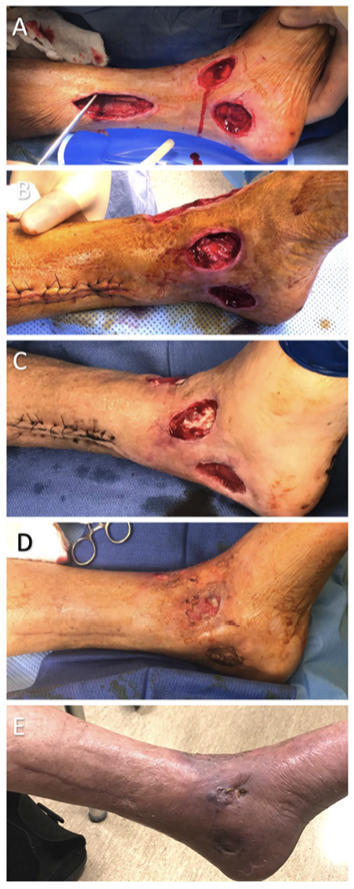
Figure 10. A 67-year-old male with a venous stasis ulcer leading to an open left ankle wound with exposed medial malleolus. (A) Serial debridement to prepare the wound. (B) The proximal wound was closed, and UBM powder and a UBM sheet matrix were applied to the remaining wounds. (C) Two weeks post-UBM, additional UBM powder was applied. (D) One month post-UBM. (E) Two-month follow-up demonstrating full epithelialization.
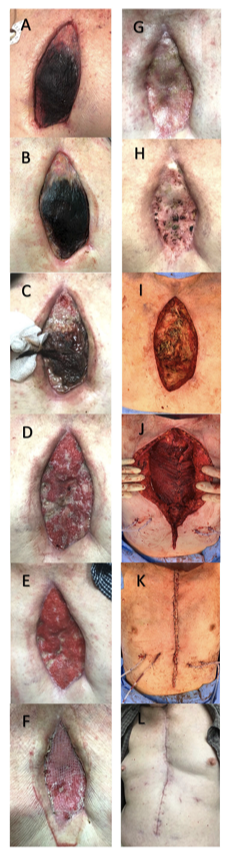
Figure 11. A 72-year-old male with a superficial sternal wound infection 3.5 months after coronary artery bypass grafting (CABG), complicated by postoperative Clostridioides difficile infection. Despite a 2-week antibiotic course, the infection progressed, requiring 3 I&Ds before applying 1500 mg UBM powder and a 10 × 15-cm UBM burn matrix, followed by a wound vac. (A) One-week post-UBM. (B) Two weeks post-UBM. (C) Three weeks post-UBM with I&D. (D) Five weeks post-UBM. (E) Six weeks post-UBM. (F) Four weeks later, superficial debridement was performed, and a 3 × 5-cm STSG was placed over the sternal wound. (G) Two weeks post-STSG. (H) Five months post-UBM with diffuse scabbing. (I-K) Fourteen weeks later, bilateral pectoralis major advancement with anterior chest wall skin flap mobilization was performed. (L) At 11 months post-UBM, the incision was well healed, and the patient resumed full activity, including pushups, without pain.

Figure 12. A 33-year-old male with uncontrolled diabetes, polyneuropathy, and chronic multifocal osteomyelitis developed a chronic left wrist and palm infection with multiple draining abscesses. (A) Serial I&D procedures followed by 500 mg UBM powder and bilayer UBM sheet matrix placement. (B) Eighteen days, (C) 3 weeks, (D) 4 weeks, and (E) 6 weeks post-UBM application showing progressive wound healing. (F) Nine weeks post-UBM with granulation tissue formation but persistent areas of exposed tendon. Additional UBM powder was applied, followed by an STSG and wound vac. (G) One week, (H) 5 weeks, and (I) 12 weeks post-STSG demonstrating progressive wound closure.

Figure 13. An 88-year-old male with multiple comorbidities sustained a gunshot wound to the left hand, resulting in a large dorsal soft tissue defect and an open comminuted second metacarpal fracture with segmental bone loss. (A) One week post-ORIF and I&D with Integra placement and a wound vac. (B) One month, (C) 2 months post-ORIF. (D) Repeat I&D with 200 mg UBM powder and a 5 × 5-cm UBM sheet matrix application. (E) One week and (F) 1 month post-UBM. (G) Three weeks post-I&D with STSG and subcutaneous fat grafting. (H) Three-month post-STSG. (I) Seven to 8 months post-STSG, with full healing. (J) One-year and (K) 13-month follow-up demonstrating durable wound closure.
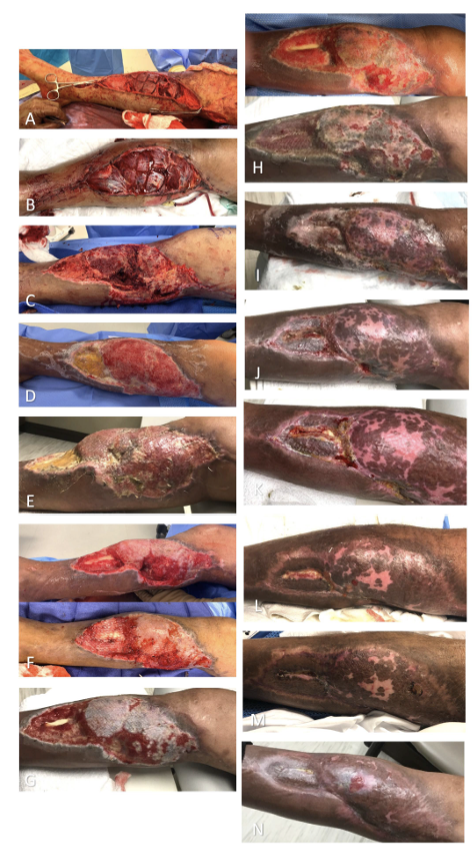
Figure 14. A 52-year-old male sustained a crush injury to the right leg from a 1000-pound air conditioning unit. (A) Initial I&D and external fixation followed by ORIF of the tibia with an intramedullary nail. (B) A bony defect was filled with an orthobiologic graft, and gastrocnemius and soleus rotational flaps were performed. (C) Two and a half weeks later, necrosis of the soleus flap was noted; UBM powder was applied with a wound vac. (D) Two weeks post-UBM, an STSG was placed. (E) Four weeks post-UBM, additional debridement was required. UBM powder and a 10 × 15-cm UBM sheet were placed over the wound. (F) One week post-UBM. (G) Three weeks post-UBM with additional STSG. (H) Two weeks, (I) 4 weeks, and (J) 5 weeks post-STSG. (K) A small area of exposed bone was debrided, and UBM powder was applied. (L) Six weeks and (M) 11 weeks post-final UBM application, demonstrating wound closure.

Figure 15. A 33-year-old male sustained a gunshot wound to the right mid-tibia, resulting in a mangling limb injury with a type 3B open tibial fracture and a 120-mm tibial nerve gap. (A) Initial I&D with external fixation, followed by ORIF with 1 g UBM powder and a 10 × 15-cm UBM sheet matrix application. (B) Eight days post-injury, the wound showed granulation tissue formation. An STSG and tibial nerve allograft repair were performed. (C) Three, (D) 8, and (E) 12 days post-STSG. (F) Six weeks post-STSG, with additional UBM powder and wound vac placement. (G) Five days post-UBM, additional STSG was performed. (H) Ten days post-STSG. (I) Three weeks later, I&D and another UBM application were performed. (J) Six weeks post-STSG, with partial flap loss. (K) A gracilis free flap was used for soft tissue coverage. (L) Four days post-flap. Also see Video 2.
Video 2. Demonstrates functional recovery; at 14 weeks post-final treatment, the patient was ambulating with minimal assistance.

Figure 16. A 57-year-old male with poorly controlled diabetes sustained a closed left trimalleolar ankle fracture after a fall. (A) Seven weeks post-injury, a 10 × 3.5 cm open wound with exposed hardware was debrided and treated with a wound vac. Three days later, a 10 × 4 cm full-thickness wound was treated with 20 mg UBM powder and a 10 × 7 cm UBM sheet matrix. (B) Twelve weeks post-UBM, repeat I&D and STSG were performed. (C) Four months later, the wound showed re-epithelialization with no signs of infection. (D) Eleven-week follow-up demonstrating continued wound improvement with only minor central scabs.
Discussion
The ideal treatment of complex wounds should focus on promoting a rapid healing process that provides durable and cosmetically acceptable coverage, minimizes pain, and allows for early mobilization to prevent stiffness and joint contracture. Traditionally, complex wounds are treated with flap coverage because they can achieve many of these goals, but this is not without its own difficulties. Microvascular reconstruction is not a resource available at many institutions and if a patient requires these services, hospital transfer may need to be initiated, which is costly in terms of both money and time, assuming that an accepting hospital can be found. In addition, flap coverage can be technically complex with donor site morbidity, risk of vascular thrombosis, and long surgical recovery time.34-36 These pitfalls are further compounded in patients with medical comorbidities that hinder wound healing or put the patient at higher risk of post-op complications, including flap failure. Ideally, treatment options for complex wounds would be available to a wide range of patients, allowing them to achieve functional healing, despite geographic location or local resources. This has led to increased interest in the use of off-the-shelf products in complex wound care.
Acellular ECM products are well-researched with several clinical applications that benefit from their treatment.37-43 Positive clinical outcomes are contingent upon protocols used to engineer the ECM material. The source of the tissue, methods of decellularization, and additional processing steps influence the host response and remodeling outcome stimulated by the ECM scaffolds.44 Scaffolds can be derived from a variety of biological origins including mammalian organ tissues and plant sources, or manufactured from synthetic or composite sources. The matrices are then decellularized to remove cellular components while retaining native 3D structure, composition, and functional molecules.45 When implanted in injured tissue, the decellularized bioscaffold undergoes rapid degradation by cellular proteases followed by gradual replacement of site appropriate tissue by resident fibroblasts. This process is termed constructive remodeling and involves the release of bioactive signaling molecules, modulation of the host immune system to a pro-healing phenotype, and recruitment of stem and progenitor cells.19,44
The use of decellularized bioscaffolds in conjunction with other reconstructive techniques may be advantageous to achieve durable and cosmetically acceptable coverage. Multiple studies have reported superior outcomes when co-grafting ADMs with STSG compared to STSG alone in terms of scar quality and elasticity.46-48 ADMs can also be combined with negative pressure wound therapy to safely and effectively treat complex extremity wounds with or without subsequent skin grafting.49,50 Ultimately, knowledge of when to employ this wound care technology can grant surgical efficiency while avoiding the morbidity of more complex procedures such as free tissue transfer.
UBM has several advantages when compared to other acellular ECM products for the treatment of complex wounds. A study conducted by Brown et al examined the presence and durability of the basement membrane component in ECM scaffolds acquired from porcine liver, intestine, and urinary bladder following decellularization. UBM was identified to be the only donor organ that preserved the basement membrane and the multiple growth factors retained within it.51 A similar study paralleled these results, finding that the basement membrane plays a role in modulating cell growth patterns, making UBM uniquely amenable to native tissue regeneration.52 Preclinical evidence also supports that UBM is associated with a beneficial host response including immune modulation towards an anti-inflammatory phenotype, proliferation and infiltration of stem cells, and promotion of angiogenesis and neovascularization.53-55 UBM materials have also been found to possess antibacterial activity against S. aureus and E. coli.56-58 This evidence lends support to utilize UBM scaffolds for regenerative medicine applications in sites with compromised vascular beds or those with high potential for bacterial contamination.
UBM products have shown efficacy in the treatment of various complicated wounds, with most data focusing on the lower extremity. Geiger et al presented 13 cases of lower extremity wounds with exposed tendons and positive cultures. Compared to prolonged negative pressure wound therapy, UBM produced a more stable, less scarred wound that more closely resembled normal anatomy.26 Kraemer et al treated 9 patients with open fractures of the lower extremity with UBM and achieved healing with normal contour and appearance and without delay of fracture healing or infections, despite the presence of exposed hardware.59 Valerio et al reported a series of combat-related injuries treated with UBM where previous reconstruction techniques had failed. Ten out of 51 patients were treated for upper extremity wounds. Two of these patients experienced UBM failure requiring revision amputation of the fingers. However, the rest were successfully treated with UBM followed by secondary STSG. Overall, the authors reported that in 86% of cases, UBM effectively stimulated the formation of granulation tissue and remodeled previously devitalized wound beds to allow for re-epithelialization, secondary dermal regeneration template placement, skin grafting, and/or flap coverage.23
The patients included in this case series had complex tissue defects. Both micronized and sheet UBM were utilized to maximize tissue regeneration while allowing for flexible coverage of these wounds. Overall, UBM facilitated constructive remodeling of the injury site, establishing a healthy, vascularized wound bed which could then re-epithelialize or support skin grafting for definitive closure. The average time to closure varied in our cases, depending on the complexity of the wound and patient’s medical status. Many of our patients had multiple comorbidities that lend to poor wound healing, such as DM, PVD, CAD, COPD, autoimmune disease, older age, and tobacco use, and 2 patients had exposed orthopedic hardware in the lower extremity. Despite this, the use of UBM helped create a favorable environment for tissue revascularization.
It is important to interpret these results with a few limitations in mind. Due to the retrospective nature of this case series, data collection was not standardized or controlled, and the lack of a control group makes it challenging to assess the comparative effectiveness of UBM to alternative treatments. The wounds treated in the study are diverse in terms of etiology, location, and severity, making it challenging to draw specific conclusions for a particular type of wound. Because of this, it is challenging to quantify time to healing, and this is further complicated by the use of skin grafting and/or flap coverage in most cases. We used clinical photographs to limit subjective interpretations of healing and cosmetic appearance. Additional prospective, randomized, controlled studies are needed to validate the clinical utility of UBM and address these limitations. Future research would be beneficial to determine potential complications, success rates, and time and quality of healing of UBM versus other reconstructive treatments. There is an opportunity to optimize bioscaffold materials and identify new molecular targets to enhance complex wound management and patient outcomes as we advance our understanding of the underlying mechanisms of constructive remodeling.
Acknowledgments
Authors: Gracie R. Baum, BS¹; Cameron T. Cox, BBA¹; Ian L. Valerio MD, MS, MBA²; Brendan J. MacKay, MD¹
Affiliations: ¹Department of Orthopedic Hand Surgery, Texas Tech University Health Science Center, Lubbock, Texas; ²Division of Plastic and Reconstructive Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts
Correspondence: Gracie R. Baum; gbaum@ufl.edu
Ethics: This project was exempt from formal review by the Texas Tech University Health Sciences Center Lubbock/Odessa Institutional Review Board (IRB L22-202). Patient consent for the use of images was not required due to the retrospective nature of the review.
Disclosures: Ian L. Valerio is a paid consultant for Integra LifeSciences. All other authors disclose no financial or other conflicts of interest.
References
1. Park H, Copeland C, Henry S, Barbul A. Complex wounds and their management. Surg Clin North Am. Dec 2010;90(6):1181-1194. doi:10.1016/j.suc.2010.08.001
2. Lee CK, Hansen SL. Management of acute wounds. Surg Clin North Am. Jun 2009;89(3):659-676. doi:10.1016/j.suc.2009.03.005
3. Beyene RT, Derryberry SL, Barbul A. The effect of comorbidities on wound healing. Surg Clin North Am. 2020 Aug;100(4):695-705. doi:https://doi.org/10.1016/j.suc.2020.05.002
4. Janis JE, Kwon RK, Attinger CE. The new reconstructive ladder: modifications to the traditional model. Plast Reconstr Surg. Jan 2011;127 Suppl 1:205s-212s. doi:10.1097/PRS.0b013e318201271c
5. Boyce DE, Shokrollahi K. Reconstructive surgery. BMJ. 2006;332(7543):710-712. doi:10.1136/bmj.332.7543.710
6. King EA, Ozer K. Free skin flap coverage of the upper extremity. Hand Clin. 2014;30(2):201-209. doi:10.1016/j.hcl.2014.01.003
7. Lecours C, Saint-Cyr M, Wong C, et al. Freestyle pedicle perforator flaps: clinical results and vascular anatomy. Plast Reconstr Surg. 2010;126(5):1589-1603. doi:10.1097/PRS.0b013e3181f02ee3
8. Sananpanich K, Tu YK, Kraisarin J, Chalidapong P. Reconstruction of limb soft-tissue defects: using pedicle perforator flaps with preservation of major vessels, a report of 45 cases. Injury. Oct 2008;39 Suppl 4:55-66. doi:10.1016/j.injury.2008.08.032
9. Ellabban MA, Awad AI, Hallock GG. Perforator-pedicled propeller flaps for lower extremity reconstruction. Semin Plast Surg. Aug 2020;34(3):200-206. doi:10.1055/s-0040-1715154
10. Georgescu AV. Propeller perforator flaps in distal lower leg: evolution and clinical applications. Arch Plast Surg. Mar 2012;39(2):94-105. doi:10.5999/aps.2012.39.2.94
11. Gir P, Cheng A, Oni G, Mojallal A, Saint-Cyr M. Pedicled-perforator (propeller) flaps in lower extremity defects: a systematic review. J Reconstr Microsurg. 2012;28(09):595-602. doi:10.1055/s-0032-1315786
12. Bekara F, Herlin C, Mojallal A, et al. A systematic review and meta-analysis of perforator-pedicled propeller flaps in lower extremity defects: identification of risk factors for complications. Plast Reconstr Surg. Jan 2016;137(1):314-331. doi:10.1097/prs.0000000000001891
13. Wang P, Lin F, Ma Y, Wang J, Zhou M, Rui Y. Predictors of the surgical outcome of propeller perforator flap reconstruction, focusing on the effective safe distance between the perforator and the wound edge. BMC Musculoskelet Disord. Jul 29 2021;22(1):643. doi:10.1186/s12891-021-04522-z
14. Cajozzo M, Jiga LP, Jandali Z, et al. Complications and solutions in propeller flap surgery. Semin Plast Surg. 2020;34(03):210-220. doi:10.1055/s-0040-1714087
15. Demir A, Kucuker I, Keles MK, Demirtas Y. The effect of learning curve on flap selection, re-exploration, and salvage rates in free flaps; a retrospective analysis of 155 cases. Microsurgery. 2013;33(7):519-526. doi:https://doi.org/10.1002/micr.22153
16. Patel UA, Hernandez D, Shnayder Y, et al. Free flap reconstruction monitoring techniques and frequency in the era of restricted resident work hours. JAMA Otolaryngol Head Neck Surg. 2017;143(8):803. doi:10.1001/jamaoto.2017.0304
17. Kwok AC, Agarwal JP. An analysis of free flap failure using the ACS NSQIP database. Does flap site and flap type matter? Microsurgery. 2017;37(6):531-538. doi:10.1002/micr.30121
18. Culliford ATt, Spector J, Blank A, Karp NS, Kasabian A, Levine JP. The fate of lower extremities with failed free flaps: a single institution's experience over 25 years. Ann Plast Surg. Jul 2007;59(1):18-21; discussion 21-22. doi:10.1097/01.sap.0000262740.34106.1b
19. Badylak SF. The extracellular matrix as a biologic scaffold material. Biomaterials. 2007 Sep;28(25):3587-3593. doi:https://doi.org/10.1016/j.biomaterials.2007.04.043
20. Iorio ML, Shuck J, Attinger CE. Wound healing in the upper and lower extremities: a systematic review on the use of acellular dermal matrices. Plast Reconstr Surg. 2012;130(5S-2):232S-241S. doi:10.1097/PRS.0b013e3182615703
21. Lanier ST, Ruter DI, Valerio IL. Regenerative medicine for soft-tissue coverage of the hand and upper extremity. Curr Ortho Prac. 2018;29(2):120-126. doi:10.1097/bco.0000000000000592
22. Daneshfar C, Suryavanshi J, Powers Wall H, Cox C, MacKay B. Palmar resurfacing of the hand With porcine urinary bladder extracellular matrix following traumatic injury. Wounds. Jul 2021;33(7):E46-E52.
23. Valerio IL, Campbell P, Sabino J, Dearth CL, Fleming M. The use of urinary bladder matrix in the treatment of trauma and combat casualty wound care. Regen Med. 2015;10(5):611-622. doi:10.2217/rme.15.34
24. Micallef CJ, Johnson JN, Johnson RM. A value analysis of microsurgical lower extremity reconstruction vs. acellular urinary bladder matrix (UBM) for radiation wounds of the lower extremity. J Surg Case Rep. 2019;2019(3)doi:10.1093/jscr/rjz051
25. Rommer EA, Peric M, Wong A. Urinary bladder matrix for the treatment of recalcitrant nonhealing radiation wounds. Adv Skin Wound Care. Oct 2013;26(10):450-455. doi:10.1097/01.ASW.0000434617.57451.e6
26. Geiger SE, Deigni OA, Watson JT, Kraemer BA. Management of open distal lower extremity wounds with exposed tendons using porcine urinary bladder matrix. Wounds. Sep 2016;28(9):306-316.
27. Lanteri Parcells A, Abernathie B, Datiashvili R. The use of urinary bladder matrix in the treatment of complicated open wounds. Wounds. Jul 2014;26(7):189-196.
28. Behrens JR, Kraemer B. Abstract: Urinary bladder matrix-extracellular matrix (UBM-ECM) for management of complex upper extremity wounds. Plast Reconstr Surg Glob Open. 2018;6(8S):51. doi:10.1097/01.Gox.0000546782.88489.39
29. Kim JS, Kaminsky AJ, Summitt JB, Thayer WP. New innovations for deep partial-thickness burn treatment with ACell MatriStem Matrix. Adv Wound Care (New Rochelle). Dec 1 2016;5(12):546-552. doi:10.1089/wound.2015.0681
30. Kimmel H, Rahn M, Gilbert TW. The clinical effectiveness in wound healing with extracellular matrix derived from porcine urinary bladder matrix: a case series on severe chronic wounds. J Am Col Certif Wound Spec. Sep 2010;2(3):55-59. doi:10.1016/j.jcws.2010.11.002
31. Lecheminant J, Field C. Porcine urinary bladder matrix: a retrospective study and establishment of protocol. J Wound Care. Oct 2012;21(10):476, 478-480, 482. doi:10.12968/jowc.2012.21.10.476
32. Frykberg RG, Cazzell SM, Arroyo-Rivera J, et al. Evaluation of tissue engineering products for the management of neuropathic diabetic foot ulcers: an interim analysis. J Wound Care. Jul 2016;25 Suppl 7:S18-S25. doi:10.12968/jowc.2016.25.7.S18
33. Alvarez OM, Smith T, Gilbert TW, et al. Diabetic foot ulcers treated with porcine urinary bladder extracellular matrix and total contact cast: interim analysis of a randomized, controlled trial. Wounds. May 2017;29(5):140-146.
34. Classen DA, Ward H. Complications in a consecutive series of 250 free flap operations. Ann Plast Surg. May 2006;56(5):557-561. doi:10.1097/01.sap.0000205830.39108.9a
35. Bui DT, Cordeiro PG, Hu Q-Y, Disa JJ, Pusic A, Mehrara BJ. Free flap reexploration: indications, treatment, and outcomes in 1193 free flaps. Plast Reconstr Surg. 2007;119(7):2092-2100. doi:10.1097/01.prs.0000260598.24376.e1
36. Bigdeli A, Gazyakan E, Schmidt V, et al. Long-term outcome after successful lower extremity free flap salvage. J Reconstr Microsurg. 2019;35(04):263-269. doi:10.1055/s-0038-1675146
37. Maruccia M, Marannino PC, Elia R, et al. Treatment of finger degloving injury with acellular dermal matrices: functional and aesthetic results. J Plast Reconstr Aesthet Surg. 2019 Sep;72(9):1509-1517. doi:https://doi.org/10.1016/j.bjps.2019.05.029
38. Jansson K, Haegerstrand A, Kratz G. A biodegradable bovine collagen membrane as a dermal template for human in vivo wound healing. Scand J Plast Reconstr Surg Hand Surg. Dec 2001;35(4):369-375. doi:10.1080/028443101317149336
39. Helgeson MD, Potter BK, Evans KN, Shawen SB. Bioartificial dermal substitute: a preliminary report on its use for the management of complex combat-related soft tissue wounds. J Orthop Trauma. Jul 2007;21(6):394-399. doi:10.1097/BOT.0b013e318070c028
40. Kahn SA, Beers RJ, Lentz CW. Use of acellular dermal replacement in reconstruction of nonhealing lower extremity wounds. J Burn Care Res. Jan-Feb 2011;32(1):124-128. doi:10.1097/BCR.0b013e318204b327
41. Weigert R, Choughri H, Casoli V. Management of severe hand wounds with Integra® dermal regeneration template. J Hand Surg Eur Vol. Mar 2011;36(3):185-193. doi:10.1177/1753193410387329
42. Clerici G, Caminiti M, Curci V, Quarantiello A, Faglia E. The use of a dermal substitute to preserve maximal foot length in diabetic foot wounds with tendon and bone exposure following urgent surgical debridement for acute infection. Int Wound J. Jun 2010;7(3):176-183. doi:10.1111/j.1742-481X.2010.00670.x
43. Taras JS, Sapienza A, Roach JB, Taras JP. Acellular dermal regeneration template for soft tissue reconstruction of the digits. J Hand Surg. 2010;35(3):415-421. doi:https://doi.org/10.1016/j.jhsa.2009.12.008
44. Cramer MC, Badylak SF. Extracellular matrix-based biomaterials and their influence upon cell behavior. Ann Biomed Eng. Jul 2020;48(7):2132-2153. doi:10.1007/s10439-019-02408-9
45. Badylak SF, Taylor D, Uygun K. Whole-organ tissue engineering: decellularization and recellularization of three-dimensional matrix scaffolds. Annu Rev Biomed Eng. 2011;13(1):27-53. doi:10.1146/annurev-bioeng-071910-124743
46. Yi JW, Kim JK. Prospective randomized comparison of scar appearances between cograft of acellular dermal matrix with autologous split-thickness skin and autologous split-thickness skin graft alone for full-thickness skin defects of the extremities. Plast Reconstr Surg. Mar 2015;135(3):609e-616e. doi:10.1097/prs.0000000000001204
47. Lee YJ, Park MC, Park DH, Hahn HM, Kim SM, Lee IJ. Effectiveness of acellular dermal matrix on autologous split-thickness skin graft in treatment of deep tissue defect: esthetic subjective and objective evaluation. Aesthet Plast Surg. 2017;41(5):1049-1057. doi:10.1007/s00266-017-0891-2
48. Lee MC, Jang YJ, Yun IS, Lew DH, Lee WJ. Comparative skin evaluation after split-thickness skin grafts using 2 different acellular dermal matrices to cover composite forearm defects. J Hand Surg Am. Apr 2017;42(4):297.e1-297.e10. doi:10.1016/j.jhsa.2017.01.026
49. Menn ZK, Lee E, Klebuc MJ. Acellular dermal matrix and negative pressure wound therapy: a tissue-engineered alternative to free tissue transfer in the compromised host. J Reconstr Microsurg. Feb;28(2):139-144.
50. Hutchison RL, Craw JR. Use of acellular dermal regeneration template combined with NPWT to treat complicated extremity wounds in children. J Wound Care. Dec 2013;22(12):708-712. doi:10.12968/jowc.2013.22.12.708
51. Brown B, Lindberg K, Reing J, Stolz DB, Badylak SF. The basement membrane component of biologic scaffolds derived from extracellular matrix. Tissue Eng. Mar 2006;12(3):519-526. doi:10.1089/ten.2006.12.519
52. Brown BN, Barnes CA, Kasick RT, et al. Surface characterization of extracellular matrix scaffolds. Biomaterials. Jan 2010;31(3):428-437. doi:10.1016/j.biomaterials.2009.09.061
53. Bullers SJ, Baker SC, Ingham E, Southgate J. The human tissue-biomaterial interface: a role for PPARγ-dependent glucocorticoid receptor activation in regulating the CD163+ M2 macrophage phenotype. Tissue Eng Part A. Sep 2014;20(17-18):2390-2401. doi:10.1089/ten.TEA.2013.0628
54. Capella-Monsonís H, De Pieri A, Peixoto R, Korntner S, Zeugolis DI. Extracellular matrix-based biomaterials as adipose-derived stem cell delivery vehicles in wound healing: a comparative study between a collagen scaffold and two xenografts. Stem Cell Res Ther. 2020/11/27 2020;11(1):510. doi:10.1186/s13287-020-02021-x
55. Wang JY, Liou A, Ren ZH, et al. Neurorestorative effect of urinary bladder matrix-mediated neural stem cell transplantation following traumatic brain injury in rats. CNS Neurol Disord Drug Targets. May 1 2013;12(3):413-425. doi:10.2174/1871527311312030014
56. Brennan EP, Reing J, Chew D, Myers-Irvin JM, Young EJ, Badylak SF. Antibacterial activity within degradation products of biological scaffolds composed of extracellular matrix. Tissue Eng. Oct 2006;12(10):2949-2955. doi:10.1089/ten.2006.12.2949
57. Jiménez-Gastélum GR, Aguilar-Medina EM, Soto-Sainz E, Ramos-Payán R, Silva-Benítez EL. Antimicrobial properties of extracellular matrix scaffolds for tissue engineering. BioMed Res Int. 2019 Dec 13;2019:9641456. doi:10.1155/2019/9641456
58. Lin Q, Zhang X, Yang D, et al. Treatment with a urinary bladder matrix alters the innate host response to pneumonia induced by Escherichia coli. ACS Biomater Sci Eng. Mar 8 2021;7(3):1088-1099. doi:10.1021/acsbiomaterials.0c01090
59. Kraemer BA, Geiger SE, Deigni OA, Watson JT. Management of open lower extremity wounds with concomitant fracture using a porcine urinary bladder matrix. Wounds. Nov 2016;28(11):387-394.