Rare Case of Pediatric Lower Limb Verrucous Venous Malformation: Treatment Approach and Considerations
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Background. Verrucous venous malformation (VVM) is a rare, congenital, low-flow vascular anomaly composed of capillaries and veins in the dermis and subcutaneous tissues. Diagnosis is difficult because knowledge of cases is rare and typically identified with sonographic imaging and elevated GLUT-1. Treatment is mired by high rates of recurrence and residual pain, with further enlargement upon resection or injury. Current management strategies include a combination of laser therapy, surgery, cryotherapy, and topical steroids, each with varying rates of success.
Methods. The authors examine a case of confirmed VVM, which was initially treated with a candela pulsed dye laser and propranolol to no avail. A combination of surgical approaches were chosen.
Conclusions. We now look to topical sirolimus 1% as an adjunct for this patient with residual lesions. Questions remain as to the effectiveness, optimal dose, and duration of topical sirolimus and whether this combination of surgical and topical intervention will be effective in the treatment for VVM.
Introduction
Verrucous venous malformations (VVMs), previously known as verrucous hemangiomas, are rare, congenital, low-flow vascular anomalies composed of capillaries and veins in the dermis and subcutaneous tissues.
Case Presentation
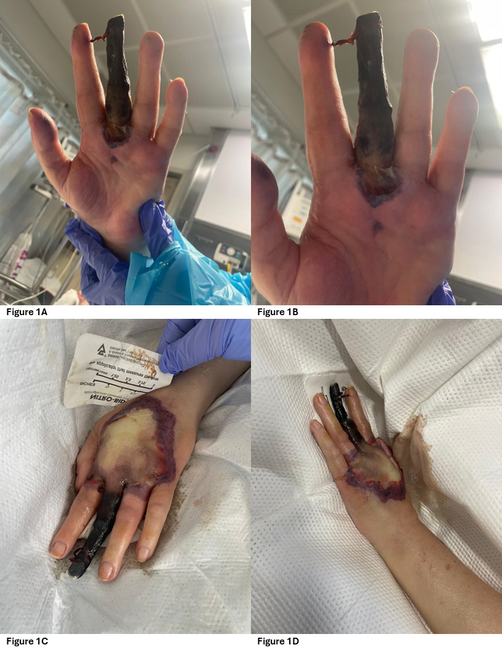
A 4-year-old boy presented to the clinic 2 years ago with well-defined, hyperkeratotic, erythematous plaques in a linear pattern over the medial aspect of his right tibia, extending to his ankle. These lesions were present at birth as flat, pink macules that were initially identified as a port wine stain (Figure 1). The initial treatment was with a pulsed dye laser (595-nm wavelength), but it did not respond. The macules grew hyperkeratotic and verrucous over time (Figure 2). Oral propranolol (20 mg bid) was initiated to no avail. Sonographic assessment of the medial aspect of the right ankle showed a widening of the subcutaneous space with amorphous, hyperechoic lesions without any significant internal flow (Figure 3). Further contrast-enhanced computed tomography shows skin thickening and soft tissue density at the medial aspect of the right ankle in the dermal and subcutaneous space (Figure 4). Additional magnetic resonance imaging (MRI) from March 2020 to evaluate superimposed cellulitis showed a 3.5 × 1.1 × 4.3-cm T1 intermediate, T2 hyperintense mass confined to the subcutaneous soft tissue along the medial aspect of the ankle along with extensive subcutaneous edema (Figure 5). The lesions were biopsied and positive for GLUT1 and a diagnosis of VVM was made. During his results at 1 year, a surgical approach was chosen. However, due to the location in the distal third of the lower leg involving the ankle, complete extirpation was not possible without necessitating a complex reconstruction (Figure 6). The lesions were partially excised to a depth of normal-appearing subcutaneous tissue. The resultant wounds were closed primarily. Our patient recovered well and healed without complications.

Figure 1. Verrucous venous malformation lesions at birth.

Figure 2. Preoperative picture of the verrucous venous malformation lesions.

Figure 3. Sonographic assessment at the medial aspect of the right ankle/foot shows amorphous hypoechoic changes with widening of the subcutaneous space.
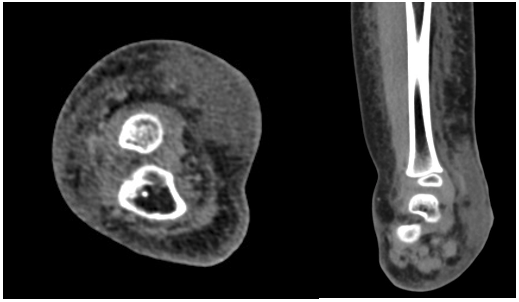
Figure 4. Contrast-enhanced computed tomography images (axial and coronal) show skin thickening and widening of the subcutaneous space due to infiltrating soft tissue density.
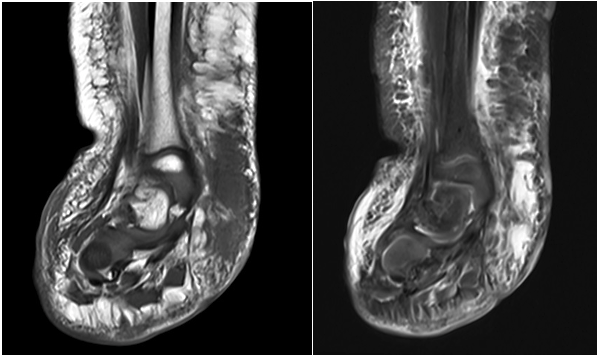
Figure 5. Coronal magnetic resonance imaging demonstrates a T1 intermediate T2 hyperintense lesion in the subcutaneous space.

Figure 6. Postoperative picture of the verrucous venous malformation lesions.
At 4 months of follow-up, the residual VVM lesions remained stable in size and character. The patient could wear footwear without discomfort. However, 2 years later the lesions returned and grew. To address these concerns, we empirically prescribed topical sirolimus 1%. After a trial with topical timolol and topical sirolimus 1%, along with pulsed dye laser therapy set at a fluency of 7.5 J/cm2 and excision, the patient continued to experience growth, requiring further pulsed dye laser therapy and injection of Kenalog (1.5 mL of 20 mg mixed with 1% lidocaine and epinephrine) as a treatment for pruritis under the verrucous lesions. Three months after these treatments the lesions recurred (Figure 7). The patient’s parents had previously opted not to use oral sirolimus due to concerns about the patient’s age and the possible side effects of the drug. At their last visit, there was further discussion about additional excision to address the growing lesions when the patient was older. The patient was not interested in discussing the use of oral sirolimus at that time.
All participants in this case provided informed consent for human subjects as required, and research was conducted in accordance with the Declaration of the World Medical Association.
Discussion
Our case study is a 4-year-old male treated with prednisone, propranolol, pulsed dye laser therapy, and surgical resection with frequent relapses. The results of the topical sirolimus were unimpressive and did not result in lesion reduction, though we did not confirm empirically through blood levels that parents were consistently using the topical sirolimus. The parents declined to use oral sirolimus due to their concern about adverse side effects for one so young. This case is a valuable experience of an example of verrucous malformation, the morbidity that patients experience through lesion reoccurrence, and the risks and benefits to various treatment regimens.
Because of their rare incidence, VVMs are often misdiagnosed and mistaken for lymphatic malformations and angiokeratoma. Similar to our patient, the literature suggests that VVMs have been treated with laser therapy, cryotherapy, topical corticosteroids, surgery, and sirolimus, with complete excision as most optimal.9 Studies suggest that complete excision is optimal because the VVMs grow in response to injury, infection, or incomplete resection.10 This was the case in our patient, where the location of the VVM on the dorsum of the food prevented complete excision, resulting in recurrence and irritation.
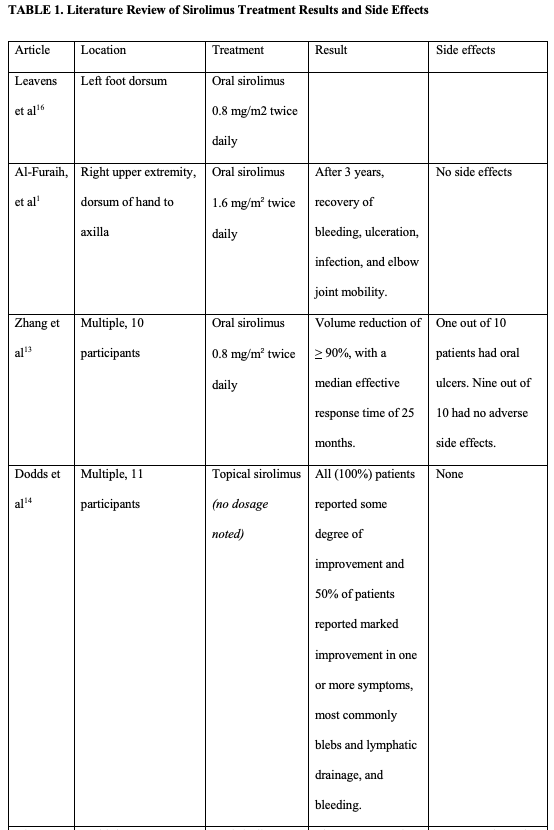
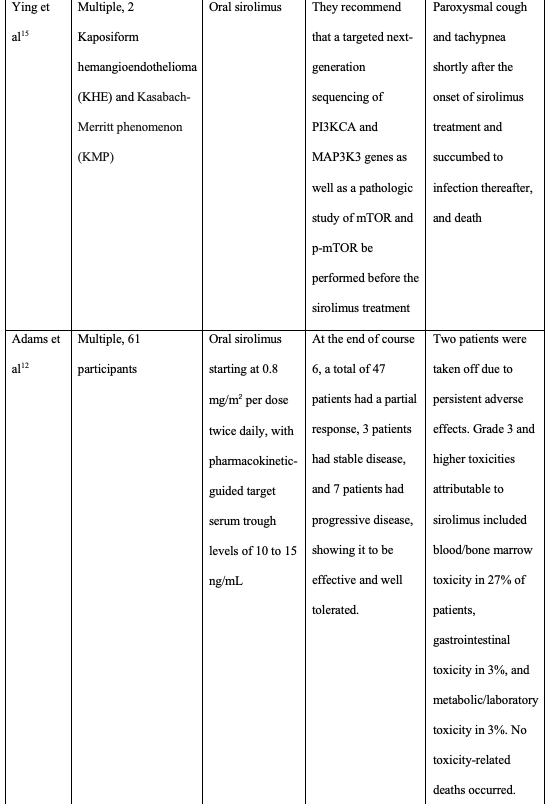
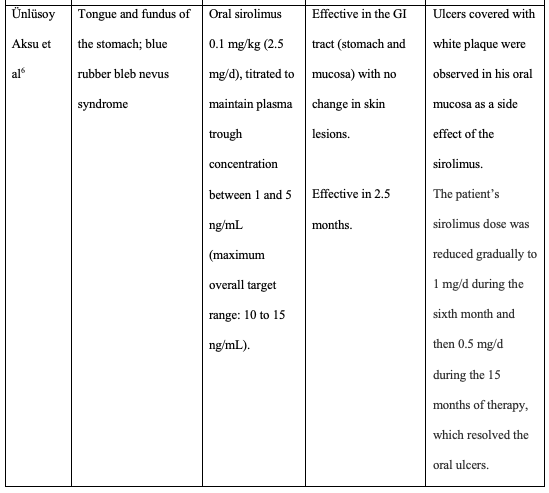
The most common side effect of oral sirolimus noted by 2 case studies were oral ulcers, which improved with reduced sirolimus dosage.6,13 Most of the participants in these studies had no adverse side effects from oral sirolimus. Adams et al treated 61 participants with oral sirolimus starting at 0.8 mg/m2 per dose twice daily, with pharmacokinetic-guided target serum trough levels of 10 to 15 ng/mL.12 In their study, of the 61 participants, 2 were taken off the drug due to adverse side effects, with the most common being blood/bone marrow toxicity (27%), gastrointestinal toxicity, and metabolic/laboratory toxicity. Of note, this study had no toxicity-related deaths. The most severe side effect noted was death, reported by Ying et
Conclusions
VVM is a rare congenital vascular anomaly that appears at birth and slowly becomes hyperkeratotic and verrucous with age. Our diagnosis was predicated upon clinical exam, imaging, histopathology, and GLUT-1 positivity. Initial treatment with laser therapy and propranolol was unsuccessful. Partial excision provided short-term success for our patient. After the use of topical sirolimus and timolol as an adjunct for this patient with residual lesions, the lesions have returned. Evidence from other VVM cases has shown that oral sirolimus has been effective in the treatment of VVM.12 However, questions remain as to whether oral sirolimus is the safest and most effective intervention for pediatric patients.7,8,12 The literature suggests that caution should be taken on initiating patients on oral sirolimus if patients have immune-compromised comorbidities. However, much of the literature suggests that oral sirolimus at a dosage of 0.8 mg/m2 twice daily was effective at shrinking lesions, preventing bleeding, and recurrence with limited side effects, including oral ulcers and blood/bone marrow toxicity. Topical sirolimus had no side effects and all cases showed modest improvement in lesion size and symptoms. Additional questions that remain include the effectiveness, optimal dose, and duration of topical sirolimus and the role of systemic MAP3 kinase inhibitors for this patient population moving forward and what combination of surgical and medical intervention will be most effective in treatment for VVM.
Acknowledgments
Authors: Annie Chen-
Affiliations: 1Virginia Commonwealth University School of Medicine, Richmond, Virginia; 2Commonwealth Dermatology, Richmond, Virginia
Correspondence: Annie Chen-
Ethics: All participants in this case provided informed consent for human subjects as required, and research was conducted in accordance with the Declaration of the World Medical Association.
Disclosures: Authors disclose no conflicts of interest related to the research or the manuscript.
References
- Al-Furaih, I. et al. Sirolimus for the management of verrucous venous malformation: a case report and literature review. Case Rep Dermatol 2021;13(2):298-303. doi:10.1159/000515984
- Croteau S, Kozakewich H, Perez-Atayde A, et al.. Kaposiform lymphangiomatosis: a distinct aggressive lymphatic anomaly. J Pediatr. 2014;164(2):383-388.
- Couto J, Vivero M, Kozakewich H, et al. A somatic MAP3k3 mutation is associated with verrucous venous malformation. Am J Hum Genet 2015;96(3):480-486.
- van Vugt LJ, van der Vleuten CJM, Flucke U, Blokx WAM. The utility of GLUT1 as a diagnostic marker in cutaneous vascular anomalies: a review of literature and recommendations for daily practice. Pathol Res Pract. 2017;213(6):591-597. doi:10.1016/j.prp.2017.04.023
- Schmidt B, El Zein S, Cuoto J, et al. Verrucous venous malformation--subcutaneous variant. Am J Dermatopathol. 2021;43(12):e181-e184. doi:10.1097/DAD.0000000000001963
- Ünlüsoy Aksu A, Sari S, Eğritaş Gürkan Ö, Dalgiç B. Favorable response to sirolimus in a child with blue rubber bleb nevus syndrome in the gastrointestinal tract. J Pediatr Hematol Oncol. 2017;39(2):147-149.
- Boccara O, Ariche-Maman S, Hadj-Rabia S, et al. Verrucous hemangioma (also known as verrucous venous malformation): a vascular anomaly frequently misdiagnosed as a lymphatic malformation. Pediatr Dermatol. 2018;35(6):e378-e381. doi:10.1111/pde.13671
- Cai R, Yang X, Gu H, Chen H, Lin X. Comment on “Sirolimus for the treatment of verrucous venous malformation: A retrospective cohort study”: Are we missing the lymphatic malformation component? J Am Acad Dermatol. 2023;88(3):e133-e134.
- Wang L, Gao T, Wang G. Verrucous hemangioma: a clinicopathological and immunohistochemical analysis of 74 cases. J Cutan Pathol. 2014;41:823-830.
- Mankani MH, Dufresne CR. Verrucous malformations: their presentation and management. Ann Plast Surg. 2000;45:31-36.
- Center for Drug Evaluation and Research. (n.d.). Drug approvals and databases. U.S. Food and Drug Administration. https://www.fda.gov/drugs/development-approval-process-drugs/drug-approvals-and-databases
- Adams DM, Trenor CC, Hammill A M, et al.. Efficacy and safety of sirolimus in the treatment of complicated vascular anomalies. Pediatrics. 2016;137(2):e20153257.
- Zhang G, Chen H, Zhen Z, et al. Sirolimus for treatment of verrucous venous malformation: A retrospective cohort study. J Am Acad Dermatol. 2019;80(2):556-558. doi:10.1016/J.JAAD.2018.07.014
- Dodds M, Tollefson M, Castello-Soccio L, et al. Treatment of superficial vascular anomalies with topical sirolimus: A multicenter case series. Pediatr Dermatol. 2020;37(2):272-277. doi:10.1111/pde.14104
- Ying, H., Qiao, C., Yang, X., & Lin, X. (2018). A Case Report of 2 Sirolimus-Related Deaths Among Infants With Kaposiform Hemangioendotheliomas. Pediatrics, 141(Suppl 5), S425–S429. https://doi.org/10.1542/peds.2016-2919
- Leavens, J., Worswick, S., & Kim, G. H. (2019). Verrucous venous malformation. Dermatology online journal, 25(12), 13030/qt9dw4w7bd.