Breast Implant Illness: Treatment Using Total Capsulectomy and Implant Removal
Abstract
Background. Breast implant illness (BII) is extramammary systemic symptoms that are caused by breast implants. The emergence of this controversial topic has spurred patients with breast implants who are experiencing these symptoms to seek implant removal, hoping to feel better. This article presents novel outcomes and suggestions for plastic surgeons in managing BII using total capsulectomy and breast implant removal.
Methods. In this retrospective cohort study conducted between 2016 and 2020, medical records of all patients undergoing breast implant removal were reviewed. Inclusion criteria consisted of all patients with history of breast implant placement presenting with mastodynia and capsular contracture on physical examination. Patients with history of implant-based reconstruction following mastectomy and patients who underwent implant exchange were excluded. All patients underwent bilateral implant removal and total capsulectomies.
Results. A total of 200 patients who fulfilled the inclusion criteria were identified. Average age was 45.5 (range: 29-73) years and average body mass index was 26.28 (range: 19-36.8), with an average follow-up time of 5 months postoperatively. Of patients with a presentation of BII, 96% reported improved or complete resolution of their systemic symptoms after implant removal and total capsulectomy. A positive microbial culture was found in 68.5% of patients, and all culture-positive patients reported improvement post-treatment. The most common organisms found were Propionibacterium acnes (49.6%). There were no associations between implant characteristics and rate of positive microbiology findings.
Conclusions. Our study shows that implant removal with capsulectomy drastically improves BII symptoms. Further large prospective cohort studies are needed to better understand this entity.
Introduction
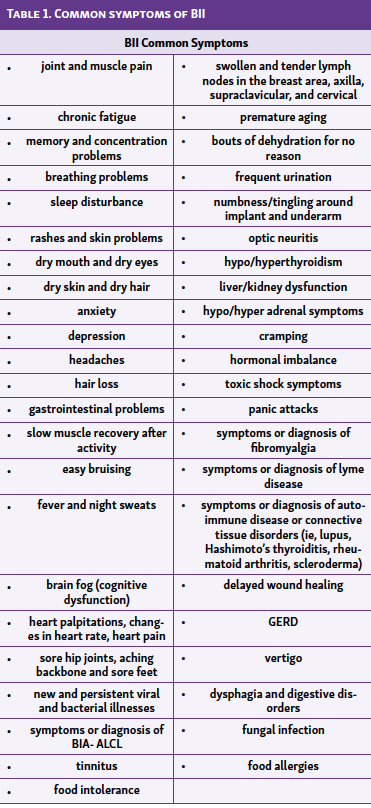
Breast implant illness (BII) refers to symptoms that develop after breast reconstruction or augmentation with any type of breast implants (saline-filled, silicone gel–filled, textured surface, smooth surface, round, or teardrop-shaped). Symptoms of BII first appeared in women in the 1980s, and there were large concerns of connective tissue diseases being linked to newly implanted silicone breast implants. These symptoms were especially prevalent in Japanese women during World War II.1,2 After years of further study, the Food and Drug Administration (FDA) approved modified breast implants to be introduced to the market.3 Unfortunately, BII is still prevalent today and impacts individuals in many unique ways including but not limited to the symptoms shown in Table 1. Symptoms may appear at any time post-breast implant surgery.
Currently, there is a lack of literature on cohort study outcomes after implant removal surgery for BII patients. A study of 100 patients concluded that 89% of patients who had capsulectomy and implant removal had symptom improvement within 3 months of surgery.4 These symptoms included cognitive problems, fatigue, burning pain in the breast and chest wall, dry eyes, anxiety, and joint pain. Researchers in the Netherlands studied 80 women with implants and found that symptoms improved in 69% of patients after surgery.5
Clearly, breast implant removal improves or completely resolves the BII symptoms. However, BII is not accepted as an official medical diagnosis. It is poorly understood, and there are limited studies because it is a unique condition. BII appears to be a cluster of symptoms that do not align with other classic diagnosis. It can worsen over time and is different in its presentation even for patients with similar implants. As of now, the incidence and prevalence of BII is increasing.
To our knowledge, there is a lack of Level I cohort studies of women with breast implants who subsequently develop BII. In our novel retrospective study, we review the outcomes in managing BII using total capsulectomy and breast implant removal. Additionally, we discuss the details of BII and what patients should do if BII is suspected.
Methods and Materials
Preoperative Preparation
From January of 2016 through September of 2020, a total of 200 sets of breast implants were removed from self-reported women with symptoms consistent with BII. Inclusion criteria consisted of all cosmetic patients with history of breast implant placement presenting with mammary symptoms (mastodynia and capsular contracture) and with or without extramammary symptoms (rash, arthralgia, etc) on physical examination. At the initial clinic visit, all patients received a questionnaire gathering information about their symptoms. Data pertaining to implant type and plane of prior implant position (submuscular vs subglandular) were collected. All patients underwent unilateral or bilateral implant removal and total capsulectomies. Specimens were sent for pathology examination and cultures (aerobic, anaerobic, fungal, and acid-fast bacilli). No patients received any previous treatment for BII. The Tulane University School of Medicine Institutional Review Board granted approval for this study.
Surgical Treatment
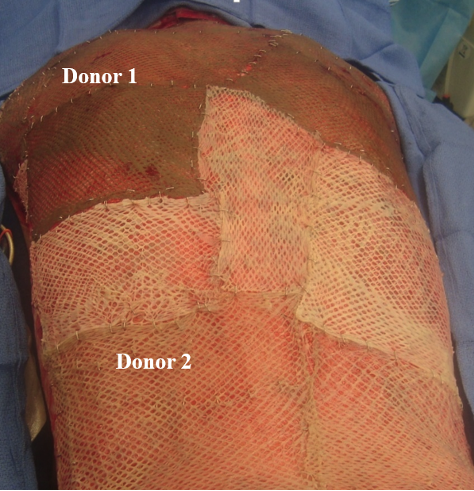
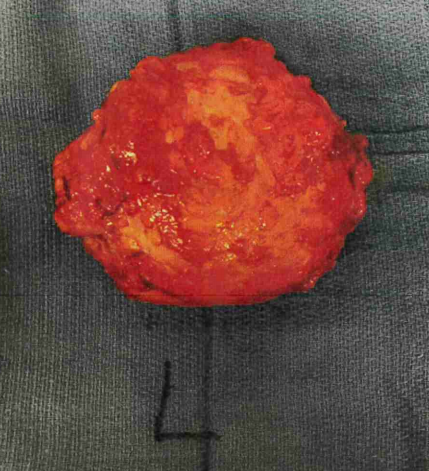
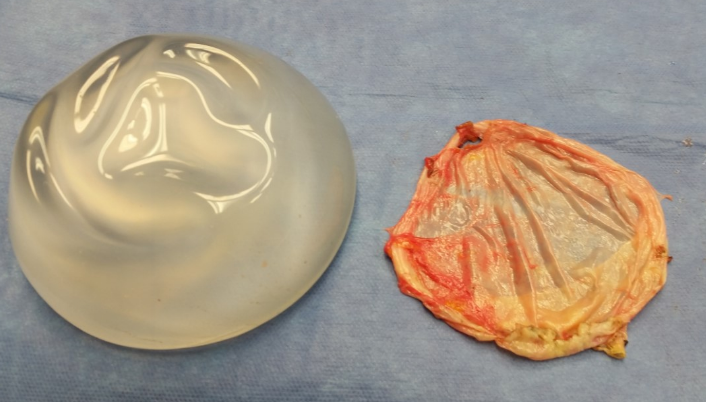
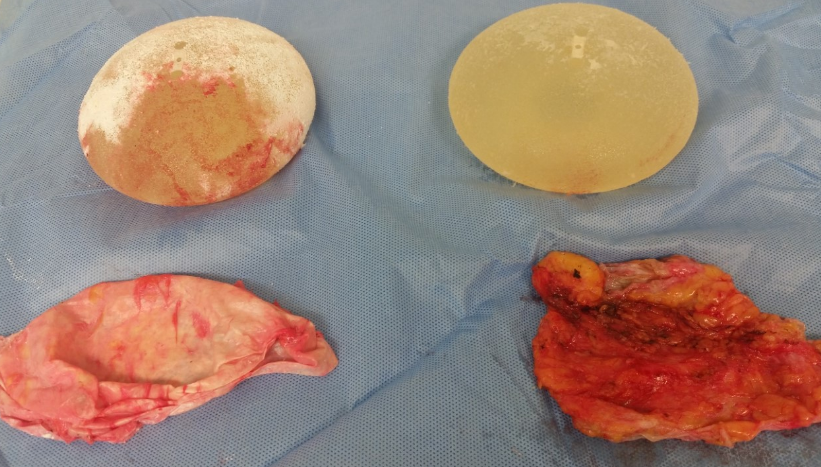
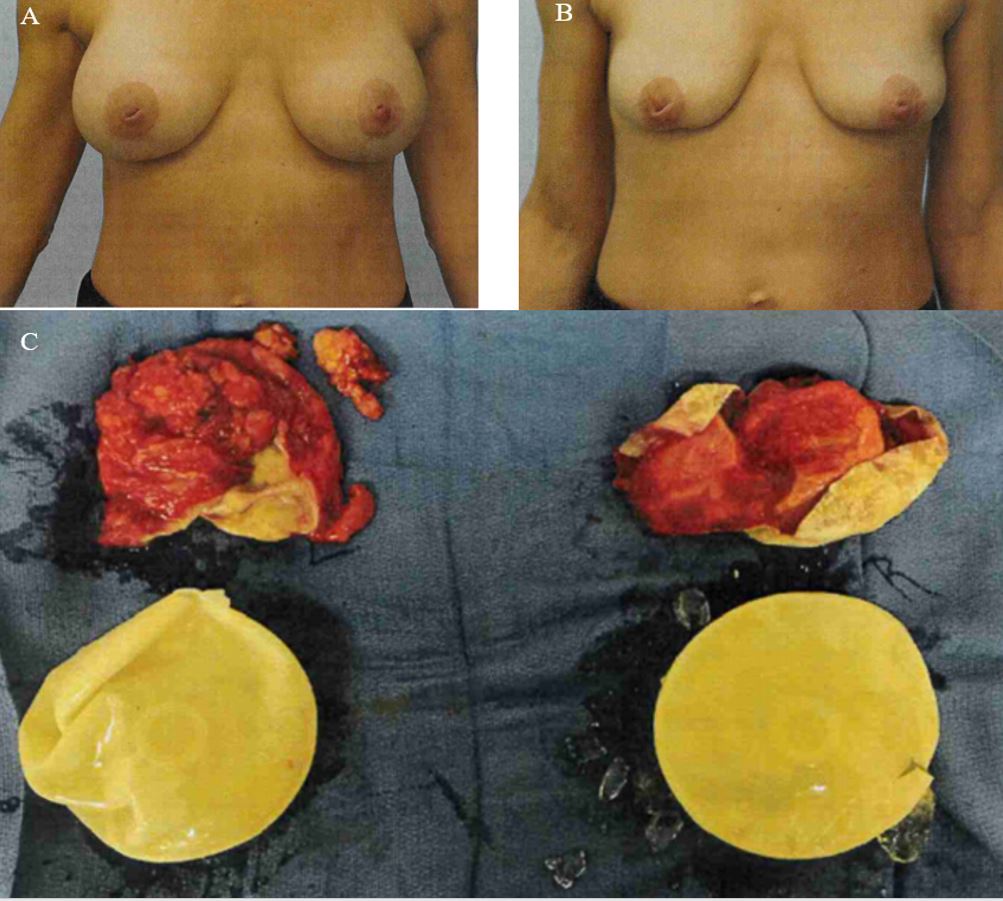
A total resection was done to remove the implants and the capsule in its entirety (Figure 1, Figure 2, and Figure 3). This consisted of removing the implant and capsule in one single piece. The senior author was responsible for all the procedures. All patients underwent standardized total capsulectomy and implant removal using monopolar electrosurgery or blunt dissection through an incision in the inframammary fold with a 6-cm incision. A guarded flat-tipped cautery was used. A bendable extender, periosteal elevator, and lighted breast retractor were used. None of the patients had partial capsulectomy.
All capsules were removed and sent for permanent histopathology. Any periprosthetic fluid with a volume of at least 50 cc was sent for cytology and specifically for CD30 to rule out anaplastic large cell lymphoma (ALCL). The pocket was then cultured for aerobic and anaerobic bacteria, acid-fast bacteria (AFB), and fungus. This was done in the following locations: (1) inside the pocket but outside the capsule, (2) inside the capsule next to the implant, and (3) if deflated or ruptured, inside the implant itself. After implant/capsule removal, the pocket was then irrigated with a triple antibiotic solution (50,000 units of Bacitracin in 500 cc of normal saline with 1 gram of Ancef and 80 mg of gentamicin). After the initial rinse, the triple antibiotic solution was mixed “half and half” with full strength betadine, placed in the pocket, and allowed to soak for 2 minutes. The pocket was then rinsed with a third wash of triple antibiotic solution, emphasizing contact time. Finally, normal closure with suture was completed.
Postoperative Management
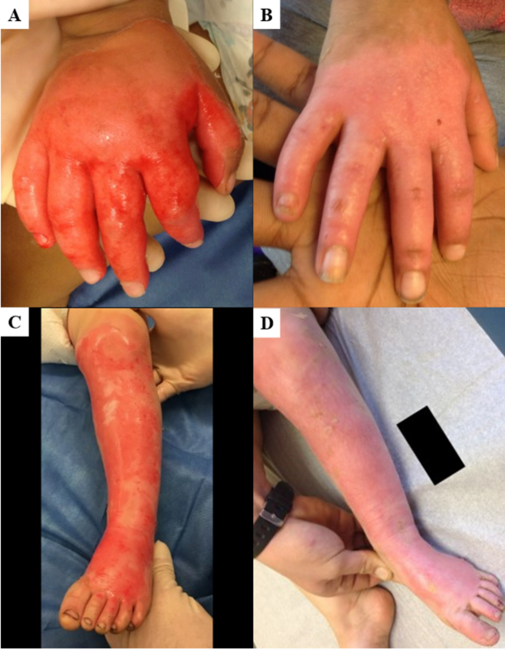
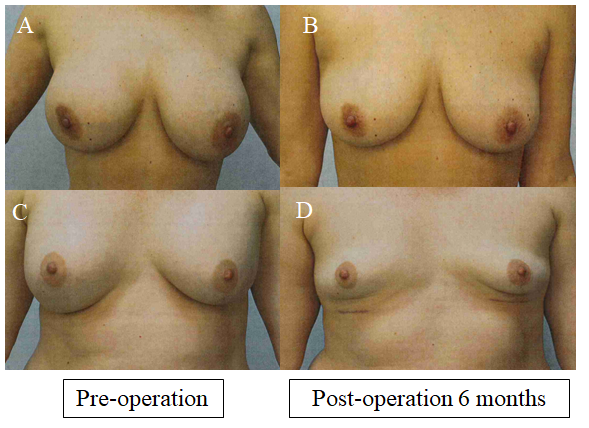
Closed suction drains were placed and left in place until the drainage was less than 25 cc in 24 hours. No reconstruction was done at the initial setting, and our patients were instructed to avoid having breast implants again. Patients were asked to return for follow-up appointments every month for the first 6 months (Figure 4). After 6 months, if the patient desired new breast implants, cosmetic options were discussed. Upon approval by the senior author, these options included mastopexy, breast reduction, fat grafting, and fat grafting with mastopexy. However, most patients did not desire a cosmetic breast reconstruction post total capsulectomy.
Results
From January 2016 through September 2020, 200 self-reported female patients with symptoms consistent with BII underwent bilateral implant removal and total capsulectomies, with specimens sent for pathology examination and cultures (Figure 5). The patients’ characteristics are summarized in Table 2. The average age was 45.5 years (range 29-73 years) and the average BMI was 26.3 (range 19-36.8). The majority of the patients (80%) had a smooth implant removed. For all patients, 59% of the implants were placed in the subpectoral plane and 41% of the implants were placed in the subglandular plane. The average follow-up time post-surgery was 5 months (range 3-46 months). Only 2 patients had postoperative complications (1.0%). One patient had wound dehiscence, and the other patient had a hematoma. Both patients recovered unremarkably.
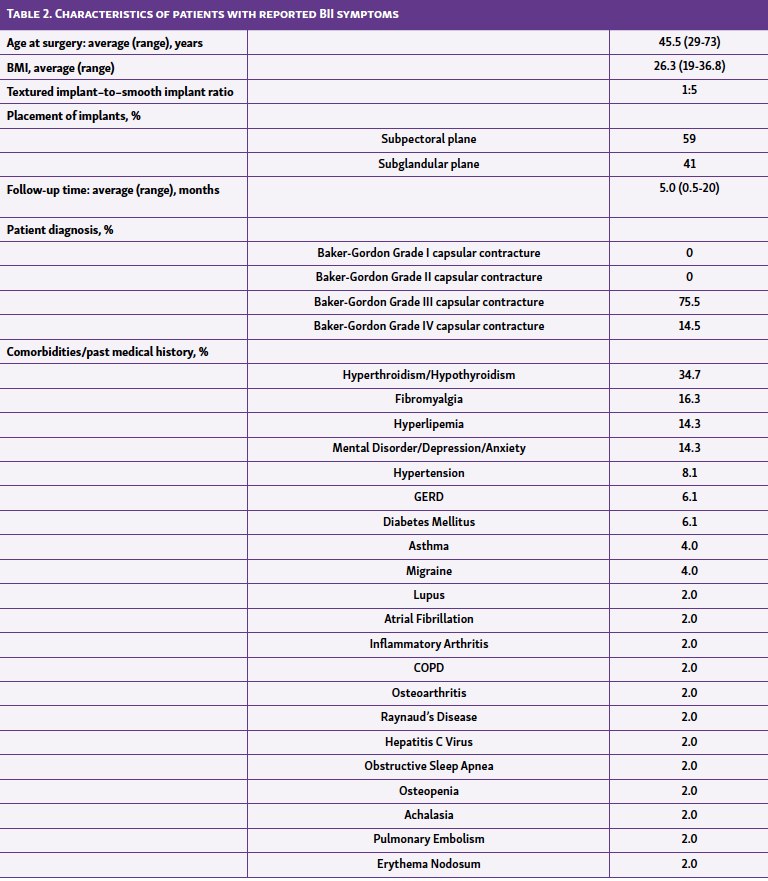
All patients (n = 200) were diagnosed with capsular contracture with the majority being Baker-Gordon Grade III (75.5%) followed by Grade IV (14.5%) in at least one breast. In addition, a high percentage of patients presented with hyperthyroidism or hypothyroidism prior to removal of the implants (34.7%; Table 2).
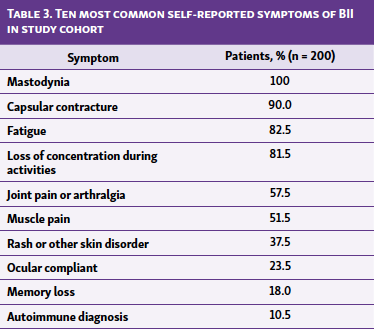
Some form of mastodynia was noted by 100% of the patients (n = 200; Table 3). At least two other BII symptoms were reported by 98% of patients, most commonly fatigue (82.5%), loss of concentration during activities (81.5%), joint pain (57.5%), muscle pain (51.5%), rash or other skin disorder (37.5%), ocular complaint (23.5%), memory loss (18.0%), and autoimmune diagnosis (10.5%).
After surgery 96% of patients reported a significant decrease in their symptoms, whereas 90.5% of patients reported a complete disappearance of symptoms after implant removal and capsulectomy. The 4% of patients (n = 8) who reported no improvement initially after surgery had negative histopathology, negative cultures, and no periprosthetic fluid.
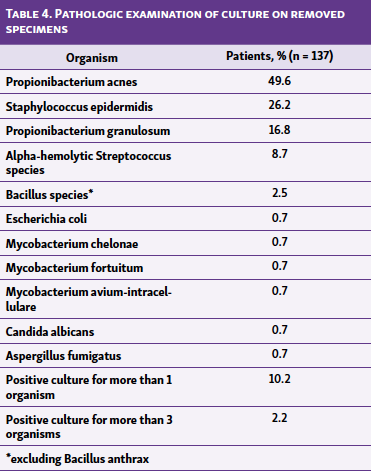
In pathologic examination of the specimens removed, 68.5% (137/200) of patients had at least 1 positive bacterial culture (Table 4). The most common organisms found were Propionibacterium acnes (49.6%) followed by Staphylococcus epidermidis (26.2%), Propionibacterium granulosum (16.8%), alpha-hemolytic streptococcus species (8.7%), and bacillus species excluding bacillus anthrax (2.5%). There was 1 positive bacterial culture of Mycobacterium Chelonae (0.7%), Mycobacterium fortuitum (0.7%), and Mycobacterium Avium-intracellulare (0.7%) and 2 positive fungi cultures of Candida albicans (1.5%) and Aspergillus fumigatus (1.5%). Extracted specimens from 14 patients grew more than 1 organism (10.2%), including 3 organisms found in 3 patients (2.2%). All patients with fungal or mycobacterial infections were sent to infectious disease specialists, and patients with other positive culture were treated with culture-specific antibiotics. All culture-positive patients reported improvement after treatment. There were no cases of breast implant associated anaplastic large cell lymphoma (BIA-ALCL), although 12 specimens were sent to cytology containing periprosthetic fluid.
Furthermore, there was no significant difference among patients in percentage of positive cultures in the implant when placed in the subglandular plane (55%, P = 0.23) and subpectoral plane (34.5%, P = 0.25). Also, there was no significant difference among patients in percentage of positive cultures bacterial cultures in textured implants (37.5%, P = 0.44) and smooth implants (43.9%, P = 0.11).
Discussion
Our study reports that 96% of patients who underwent bilateral implant removal and total capsulectomies for BII-related symptoms reported improved or complete resolution of symptoms. The advantage of a total capsulectomy is that it prevents substances within the capsule such as silicone or biofilm from escaping into the body. By removing the scar tissue capsules and using drains, the risk that fluid will collect in the surgical site is reduced. Additionally, the implant should not be allowed to come into contact with normal tissue because it is still within the capsule during total capsulectomy. This prevents the recurrence of BII or other infection.
In our study the reconstruction was staged, allowing the breast to rest and contract and also allowing time for the return of culture results to institute appropriate treatment. Additionally, this gives patients more time to make an informed decision on reconstructive options. As the breast contracts and the inflammation decreases, the reconstruction becomes easier. On the other hand, some patients choose to undergo no further surgery. Nonetheless, there are reconstructive options such as mastopexy, breast reduction, fat grafting, or even a combination of fat grafting and mastopexy.
After surgical treatment, some of our BII patients wanted to replace their implants with new implants of a different type. This approach may improve BII symptoms but carries a greater risk that symptoms will return. This may be due to these patients being predisposed to reacting to breast implants and/or the biofilm. Both silicone and saline breast implant types are made from similar materials, and any foreign body can attract a biofilm or be contaminated. Biofilm formation around an implant can cause infections, capsular contracture, and other systemic symptoms.
A possible solution for future prevention of biofilms is to use multipurpose disinfection solution (MPS), similarly to the way contact lenses are cleaned. Fears et al. found that their novel MPS was rapid and effective at killing Acanthamoeba species in contact lens disinfection systems.6 Additionally, implant pocket irrigation seems to be an ideal way to prevent biofilms. In a survey assessing practices at preventing breast implant contamination, it was found that plastic surgeons used betadine (44%) and clorpactin (14%) to irrigate the breast pocket prior to inserting the implant.7 Another possible solution for biofilm prevention is to use antimicrobial solutions such as 10% povidone-iodine instead of saline.8,9 Jewell et al. found that povidone-iodine was effective in killing gram-negative and gram-positive bacteria associated with biofilms that have been linked to capsular contracture.8,9 Saline was not effective and may only be used for removing nonbacterial components such as fluids or blood.8,9
Use of a Keller funnel is suggestd to decrease the rate of capsular contracture. The Keller funnel is used to mechanically decrease bacterial contamination by limiting the implant’s contact with the skin and ducts.10 In the same survey that was sent in Gowda et al.’s study, 69% of surgeons reported using a Keller funnel during breast reconstruction with breast implants.7 In a study conducted by Newman et al., when a Keller funnel was used, there was an 87% rate reduction in capsular contracture in patients having periareolar breast augmentation.10
Propionibacterium acnes was the most common organism in our pathologic reports on patients’ specimens. It is currently being studied to be associated with “rheumatological disorders, thyroid disease, sarcoidosis, endophthalmitis, and prostate disease.”11-13 Propionibacterium acnes has been found in the lymph nodes of patients suffering atherosclerosis, sarcoidosis, and discitis associated with sciatica. It is shown in both SAPHO (synovitis, acne, pustulosis, hyperostosis, and osteitis) syndrome and CREST (calcinosis, Raynaud's phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia) disease.12 Per-oral clarithromycin treatment of P. acnes in the lymph nodes of a sarcoidosis patient yielded disease resolution.14 This study raises the exciting prospect of possibly antibiotic treatment of BII or prevention with altered antibiotic prophylaxis regimes.14
Earlier studies for infective etiology explored the possibility of commensal contaminants being a cause for disease.15-17 Agents including anaerobic bacteria, fungi, and atypical organisms such as acid-fast bacilli were explored. These studies demonstrated colonization of implants and capsular tissue with S. epidermidis. Other organisms, such as Escherichia coli and P. acnes, were also noted.15,17 The development of bacterial infection in the setting of the implant capsule may be supported by the finding that natural killer cell function is suppressed in the presence of a breast implant but is then reversed upon explantation.18
How do we diagnose BII and who may be at risk?
There are no diagnostic tests or criteria for BII. Elevation in sedimentation rate and C-reactive protein are nonspecific markers found in some cases. Plastic surgeons who treat BII patients remark that it is common for those who seek treatment to have multiple symptoms that are interfering with their ability to function.5,19-21 The common BII symptoms seen in this study were also seen in other similar studies. These symptoms included fatigue, cognitive problems, arthralgia, and ocular problems.5,22 Many have gone to a number of other doctors before realizing that their symptoms may be connected to their implants. Alternative medicine physicians are treating an increasing number of these patients with nontraditional methods. Unfortunately, there is some charlatanism encountered by these patients.
We recommend that plastic surgeons rule out other causes of BII symptoms that are not related to the breast implants. This involves looking at test results (for inflammatory conditions) and determining whether any symptoms improved when the patient received treatment for other conditions. A patient may have BII and a diagnosed autoimmune disease. It is important to remember there is also a psychological component to this disease as well as a psychosocial aspect.5,19-21
Additionally, it can be particularly helpful after implant removal surgery for BII patients to eat a healthy diet, participate in regular exercise, and decrease stress. These steps will promote healing and decrease the inflammation in the body that can be associated with BII.20,21
BII may be caused by family genetics as well. For example, patients who have a personal or family history of autoimmune conditions, allergies, and irritable bowel syndrome may be susceptible to BII.16,23 More importantly, there is no evidence that having a history of breast cancer or any other cancer makes a patient more likely to develop BII.16,23-26 These findings tend to support these conclusions.
What causes BII?
There is a lack of research on why some women with breast implants develop BII. One leading theory is that some people are predisposed to having an immune reaction to the breast implant material. This inflammation leads to symptoms such as joint and muscle pain, rashes, and gastrointestinal problems. Studies have shown that substances from breast implants (such as very small amounts of silicone and platinum) can “bleed” through an intact shell and into the surrounding tissue.5,19-21 Substances from an implant can also spread within the capsule of scar tissue surrounding the implant or to other parts of the body due to a ruptured implant. There is a direct correlation between the duration of a breast implant in place and the likelihood of rupturing.
All women with breast implants are exposed to silicone due to the silicone shell. Based on our findings, biofilm contamination also plays a major role and may even be more prevalent than silicone sickness. It is possible that both contamination and silicone exposure in some people cause symptoms and disease.5,21
Studies have shown that BII symptoms may be secondary to chemical toxicity associated with implant materials and catalysts. Assertions have been raised about purported heavy metals, pathological organic compounds, and toxicity associated with industrial silicone in poly implant prothese devices.12,27 Platinum is used as a cross-linking catalyst of silicone elastomers and present in silicone implant shells in microgram quantities.28 Neurotoxicity is not demonstrated in elemental platinum but rather in platinum-based chemotherapeutic agents. Lykissa et al27 claimed that the compound hexachloroplatinate was found in implants; however, repeated studies have failed to replicate this. Brook29 found that the quantity of platinum in implants is in the parts-per-million range, in the unoxidized form, making biologically reactivity unlikely. At the FDA’s General and Plastic Surgery Devices Advisory Panel public meeting on breast implants in March 2019, an overview was given of scientific evidence that the silicone in breast implants can activate the immune system, resulting in inflammation and autoimmune problems.5,20 Currently, the idea that the silicone in medical devices can affect the immune system is not widely accepted in medicine. The FDA announced in March 2019 that it is undertaking new efforts to evaluate the safety of medical device materials, including silicone.19 Other implants that are coated with silicone, such as pacemakers, may also develop biofilms. Further studies should be conducted to elicit the outcomes of silicone-containing implants and medical devices implanted in humans.
Emerging research on BII
For the most part, the existing scientific literature does not show a definite connection between breast implants and autoimmune or connective tissue diseases and does not show that breast implants cause these conditions. A study conducted at University of Texas MD Anderson Cancer Center analyzed medical records of 100,000 women who had implants and were enrolled in long-term safety studies required by the FDA.20 The researchers found that women with silicone gel–filled implants were 6 to 8 times more likely to be diagnosed with Sjögren syndrome, scleroderma, and rheumatoid arthritis.20 However, there were some limitations in the study where some of the diseases were reported by patients. Outcomes were collected under more than 1 protocol, and a significant number of patients dropped out before the studies ended.20
In addition, a team of researchers examined the electronic health records of 123,255 Israeli women (24,651 had silicone gel–filled breast implants and the rest did not have breast implants).21 The records contained up to 20 years of data. The researchers found that the women with silicone gel–filled breast implants were significantly more likely to be diagnosed with autoimmune or rheumatic disorders, such as Sjögren syndrome, systemic sclerosis, and sarcoidosis, compared with women without breast implants of a similar age and socioeconomic status.21
Finally, there have been studies that show a substantial number of BII patients do not experience symptom improvement after explantation.30 More studies are needed to prove these associated theories.
What should patients do if they think they have BII?
- A patient that is considering getting breast implants for the first time or replacing ones that they already have should discuss with their plastic surgeon the possibility of having a potential risk factor for BII. Prior to every breast implant placed, patients should have a thorough informed consent discussion with the plastic surgeon.31 An autologous reconstruction is recommended for patients who have risk factors.
- Patients should consider replacing breast implants every 10-15 years; if patients start to develop symptoms of BII, they should not have implants replaced once the old implants are removed.
- If a patient thinks they have BII, they should seek out a board-certified plastic surgeon who has experience treating BII patients and is not dismissive about the symptoms the patient is experiencing. It should not be assumed that the surgeon who placed the implants is the surgeon that should remove them.
- Private health insurance plans cover surgery to remove breast implants in women who have had a mastectomy and breast reconstruction. Because BII has no diagnosis code, plastic surgeons should record patient symptoms such as breast pain, rupture of implant, and shortness of breath to show the insurance company that surgery is necessary. This prevents paying out of pocket for implant removal.
- Although this study adds some validity to the concept of BII, further studies should be conducted through the Plastic Surgery Foundation’s National Breast Implant Registry (NBIR).32
Limitations
The results of this study have several limitations. Due to the retrospective nature of our study, data collection bias may occur in which symptoms reported may not represent all symptoms associated with BII. Sampling bias may be possible because patients who had their implants removed were not representative of the overall breast reconstruction patient population. Although comorbidities are presented in this study, it does not take these into account in the data analysis. Additionally, although a questionnaire was provided to each subject, a BREAST-Q evaluation of outcomes33 for these women would provide a more accurate subjective assessment of their mammary, extra-mammary, and other systemic symptoms. Further prospective studies taking into account of comorbidities would be beneficial to understanding BII more in depth.
Conclusions
After bilateral implant removal and capsulectomy, 96% of patients with a presentation of BII reported improved or complete resolution of symptoms. The method of total capsulectomy presented in this study was shown to be effective in treating BII patients, but future research efforts including long-term prospective studies are warranted to further understand BII.
Acknowledgments
Affiliations: 1Division of Plastic and Reconstructive Surgery, Tulane University School of Medicine, New Orleans, LA; 2Aesthetic Surgical Associates, Metairie, LA; 3Division of Plastic and Reconstructive Surgery, Tufts Medical Center, Boston, MA; 4Department of Ophthalmology, Tulane University School of Medicine, New Orleans, LA
Correspondence: Stephen E. Metzinger, MD, MSPH, FACS; drmetzinger@aestheticsurgical.com
Disclosure: The authors have no financial disclosures. No funding was received for this article.
References
1. Duffy MJ, Woods JE. Health risks of failed silicone gel breast implants: a 30-year clinical experience. Plast Reconstr Surg. 1994;94(2):295-299. doi:10.1097/00006534-199408000-00012
2. Watanabe K. Subpectoral breast augmentation in the Japanese. Ann Plast Surg. 1980;5(1):24-30. doi:10.1097/00000637-198007000-00005
3. Van Zele D, Heymans O. Breast implants. A review. Acta Chir Belg. 2004;104(2):158-165. doi:10.1080/00015458.2004.11679528
4. What Is Breast Implant Illness? Breastcancer.org. Updated October 29, 2020. Accessed August 15, 2020. https://www.breastcancer.org/treatment/surgery/reconstruction/types/implants/special-report/breast-implant-illness
5. Maijers MC, de Blok CJ, Niessen FB, et al. Women with silicone breast implants and unexplained systemic symptoms: a descriptive cohort study. Neth J Med. 2013;71(10):534-40.
6. Fears AC, Metzinger RC, Killeen SZ, Reimers RS, Roy CJ. Comparative in vitro effectiveness of a novel contact lens multipurpose solution on Acanthamoeba castellanii. J Ophthalmic Inflamm Infect. 2018;8(1):19. doi:10.1186/s12348-018-0161-8
7. Gowda AU, Chopra K, Brown EN, Slezak S, Rasko Y. Preventing Breast Implant Contamination in Breast Reconstruction: A National Survey of Current Practice. Ann Plast Surg. 2017;78(2):153-156. doi:10.1097/SAP.0000000000000822
8. Jewell ML, Hariri S, Lantz EE, Jewell HL, Strickland AD, Leung BK. In Vitro Evaluation of Common Antimicrobial Solutions Used for Breast Implant Soaking and Breast Pocket Irrigation-Part 1: Efficacy Against Planktonic Bacteria. Aesthet Surg J. 2021;41(11):1242-1251. doi:10.1093/asj/sjaa309
9. Jewell ML and Adams Jr WP. Betadine and Breast Implants. Aesthet Surg J. 38(6):623-626. doi:10.1093/asj/sjy044
10. Newman AN, Davison SP. Effect of Keller Funnel on the Rate of Capsular Contracture in Periareolar Breast Augmentation. Plast Reconstr Surg Glob Open. 2018;6(6):e1834. Published 2018 Jun 18. doi:10.1097/GOX.0000000000001834
11. Portillo ME, Corvec S, Borens O, Trampuz A. Propionibacterium acnes: an underestimated pathogen in implant-associated infections. Biomed Res Int. 2013;2013:804391. doi:10.1155/2013/804391
12. Aubin GG, Portillo ME, Trampuz A, Corvec S. Propionibacterium acnes, an emerging pathogen: from acne to implant-infections, from phylotype to resistance. Med Mal Infect. 2014;44(6):241-250. doi:10.1016/j.medmal.2014.02.004
13. Jacobs AM, Van Hooff ML, Meis JF, Vos F, Goosen JH. Treatment of prosthetic joint infections due to Propionibacterium. Similar results in 60 patients treated with and without rifampicin. Acta Orthop. 2016;87(1):60-66. doi:10.3109/17453674.2015.1094613
14. Takemori N,Nakamura M, Kojima M, Eishi Y. Successful treatment in a case of Propionibacterium acnes-associated sarcoidosis with clarithromycin administration: a case report. J Med Case Rep. 2014;8:15. doi: 10.1186/1752-1947-8-15
15. Dobke MK, Svahn JK, Vastine VL, Landon BN, Stein PC, Parsons CL. Characterization of microbial presence at the surface of silicone mammary implants. Ann Plast Surg. 1995;34(6):563-571. doi:10.1097/00000637-199506000-00001
16. Ahn CY, Ko CY, Wagar EA, Wong RS, Shaw WW. Microbial evaluation: 139 implants removed from symptomatic patients. Plast Reconstr Surg. 1996;98(7):1225-1229. doi:10.1097/00006534-199612000-00016
17. Dowden RV. Periprosthetic bacteria and the breast implant patient with systemic symptoms. Plast Reconstr Surg. 1994;94(2):300-305. doi:10.1097/00006534-199408000-00013
18. Campbell A, Brautbar N, Vojdani A. Suppressed natural killer cell activity in patients with silicone breast implants: reversal upon explantation. Toxicol Ind Health. 1994;10(3):149-154. doi:10.1177/074823379401000304
19. Breast Implant Illness - Frequently Asked Questions/Talking Points. The Aesthetic Society. 2009. Accessed August 1, 2020. https://www.surgery.org/sites/default/files/downloads/BII-Talking-Points-FINAL-1.15.19.pdf
20. Coroneos CJ, Selber JC, Offodile AC 2nd, Butler CE, Clemens MW. US FDA Breast Implant Postapproval Studies: Long-term Outcomes in 99,993 Patients. Ann Surg. 2019;269(1):30-36. doi:10.1097/SLA.0000000000002990
21. Watad A, Rosenberg V, Tiosano S, et al. Silicone breast implants and the risk of autoimmune/rheumatic disorders: a real-world analysis. Int J Epidemiol. 2018;47(6):1846-1854. doi:10.1093/ije/dyy217
22. Fryzek JP, Signorello LB, Hakelius L, et al. Self-reported symptoms among women after cosmetic breast implant and breast reduction surgery. Plast Reconstr Surg. 2001;107(1):206-213. doi:10.1097/00006534-200101000-00034
23. Arthur EB. Amelioration of systemic disease after removal of silicone gel-filled breast implants. J Nutr Environ Med 2009;10(2).
24. Brawer AE. Chronology of systemic disease development in 300 symptomatic recipients of silicone gel-filled breast implants. J Clean Technol Environ Toxicol Occup Med. 1996;5(223-233).
25. de Boer M, Colaris M, van der Hulst RRWJ, Cohen Tervaert JW. Is explantation of silicone breast implants useful in patients with complaints?. Immunol Res. 2017;65(1):25-36. doi:10.1007/s12026-016-8813-y
26. Blackburn WD Jr, Grotting JC, Everson MP. Lack of evidence of systemic inflammatory rheumatic disorders in symptomatic women with breast implants. Plast Reconstr Surg. 1997;99(4):1054-1060. doi:10.1097/00006534-199704000-00020
27. Lykissa ED, Kala SV, Hurley JB, Lebovitz RM. Release of low molecular weight silicones and platinum from silicone breast implants. Anal Chem. 1997;69(23):4912-4916. doi:10.1021/ac970710w
28. Lee M, Ponraja G, McLeod K, Chong S. Breast Implant Illness: A Biofilm Hypothesis. Plast Reconstr Surg Glob Open. 2020;8(4):e2755. Published 2020 Apr 30. doi:10.1097/GOX.0000000000002755
29. Brook MA. Platinum in silicone breast implants. Biomaterials. 2006;27(17):3274-3286. doi:10.1016/j.biomaterials.2006.01.027
30. Tang SYQ, Israel JS, Afifi AM. Breast Implant Illness: Symptoms, Patient Concerns, and the Power of Social Media. Plast Reconstr Surg. 2017;140(5):765e-766e. doi:10.1097/PRS.0000000000003785
31. S. Metzinger. Breast Augmentation Risks and Informed Consent. Aesthetic Surgical Associates. 2016.
32. National Breast Implant Registry. The Plastic Surgery Foundation. Accessed 2021. https://www.thepsf.org/research/registries/nbir
33. Pusic AL, Klassen AF, Scott AM, Klok JA, Cordeiro PG, Cano SJ. Development of a new patient-reported outcome measure for breast surgery: the BREAST-Q. Plast Reconstr Surg. 2009;124(2):345-353. doi:10.1097/PRS.0b013e3181aee807