Group A Streptococcal Rapid Antigen Detection Test: A Clinical Study to Evaluate the Reproducibility Using Human Wound Samples
Abstract
Background. The early diagnosis of necrotizing soft tissue infection (NSTI) caused by group A streptococcus (GAS) for performing debridement surgery is key to the patient survival. In 1996, the diversional use of a GAS-rapid antigen detection test (RADT) for pharyngitis was reported, quickly spreading as a clinically useful method. However, no clinical study has evaluated the reliability of RADT by using wound samples. This is the first study using clinical wound samples to examine the reproducibility between GAS-RADT and wound culture.
Methods. Patients in whom wound culture samples were clinically necessary were included in this study. Two samples were obtained simultaneously: one for isolation of bacteria as wound culture and the other for GAS-RADT, with written informed consent. The reproducibility between GAS-RADT and wound culture was statistically evaluated by Cohen’s kappa coefficient.
Results. One hundred samples from 94 patients were collected from 2020 to 2021. Two samples were GAS-positive on wound culture, and both were RADT-positive (positive reproducibility: 100%). Ninety-eight samples were GAS-negative on wound culture; of these, 97 were RADT-negative (negative reproducibility: 99%). Cohen’s kappa coefficient was 0.80, indicating excellent agreement beyond chance. None of the bacteria showed cross-reactional influences. The only discrepant case (RADT-positive and wound culture-negative) was attributed to the administration of antibiotics for 2 days before the sampling.
Conclusions. The reproducibility between GAS-RADT and wound culture was statistically excellent, underscoring the reliability of GAS-RADT for wounds.
Introduction
Necrotizing soft tissue infection (NSTI) caused by group A streptococcus (GAS) is a life-threatening severe disease. In 2008, a large-scale epidemiological study in Europe (Strep-EURO) showed the fatality rate of GAS-NSTI within 7 days of the diagnosis to be 32%.1 NSTI with clinical signs of septic shock and tissue necrosis is easy to diagnose; however, clinical signs of GAS-NSTI can be sometimes absent, ambivalent, and misleading.2 In 1996, the diversional use of a GAS-rapid antigen detection test (RADT) for pharyngitis was reported.3,4 We also reported the utility of RADT for GAS for avoiding overindicated surgery.5 While such a quick diagnostic method is clinically valuable, no study has evaluated the reliability of RADT by using clinical wound samples.
We examined 100 human wound samples using GAS-RADT during wound culture sampling and investigated the reproducibility between the RADT and wound culture.
Methods and Materials
Clinical sampling was performed in Kyoto University Hospital and Ijinkai Takeda General Hospital with the approval of the Kyoto University Medical Ethics Committee (R2417) and Takeda Hospital Group Ethics Committee (20200009), respectively. This study was a nonrandomized study. To examine the reproducibility between the RADT and wound culture, wound samples were collected with or without suspicion of NSTI. The inclusion criteria were adult patients aged ≥20 years who understood the study and consented in writing. Patients for whom wound culture samples were clinically necessary were included; “clinically necessary” was defined as the detection of bacterial species would aid in selecting treatment. Consequently, not only severe inflammation but also animal bite wounds and wounds requiring prolonged healing wounds were represented. Wounds in the oral and nasal cavity were excluded as a diversional use method.
Several wound cultures were obtained during surgery, and the others were collected bedside or during outpatient visits. Two samples were obtained simultaneously using 2 sterile cotton swabs: one for isolation of bacteria as wound culture and the other for GAS-RADT. RADT samples were frozen with anonymized numbering and sent to Sekisui Medical Laboratory (Tsukuba, Japan). GAS-RADTs were performed using RapidTesta StrepA (Sekisui Medical Co, Ltd).
Reproducibility between the GAS-RADT and wound culture was statistically evaluated by Cohen’s kappa coefficient using the valuation of Fleiss: <0.40, poor; 0.40-0.75, fair; >0.75, excellent agreement beyond chance.6
Results
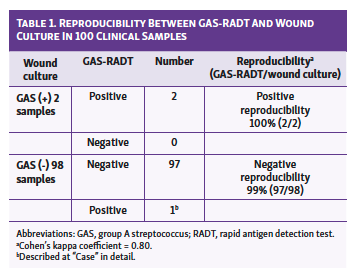 One hundred samples from 94 patients were collected from September 2020 to July 2021. The average patient age was 68 years. Locations of the sampled wounds were head and neck (n = 14), trunk (n = 23), upper limbs (n = 13), and lower limbs (n = 50). None of the 14 samples from head and neck wounds were located in oral and nasal cavities (cheek, n = 3; lower jaw, n = 8; and neck, = 3). Two samples were GAS-positive by wound culture, and both were RADT-positive (positive reproducibility: 100%). Ninety-eight samples were GAS-negative by wound culture, and of these, 97 were RADT-negative (negative reproducibility: 99%). Cohen’s kappa coefficient was 0.80, showing excellent agreement beyond chance (Table 1).
One hundred samples from 94 patients were collected from September 2020 to July 2021. The average patient age was 68 years. Locations of the sampled wounds were head and neck (n = 14), trunk (n = 23), upper limbs (n = 13), and lower limbs (n = 50). None of the 14 samples from head and neck wounds were located in oral and nasal cavities (cheek, n = 3; lower jaw, n = 8; and neck, = 3). Two samples were GAS-positive by wound culture, and both were RADT-positive (positive reproducibility: 100%). Ninety-eight samples were GAS-negative by wound culture, and of these, 97 were RADT-negative (negative reproducibility: 99%). Cohen’s kappa coefficient was 0.80, showing excellent agreement beyond chance (Table 1).
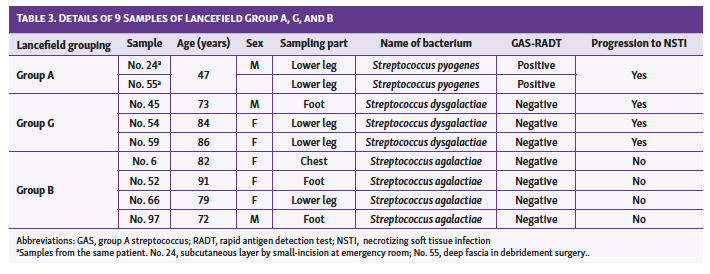
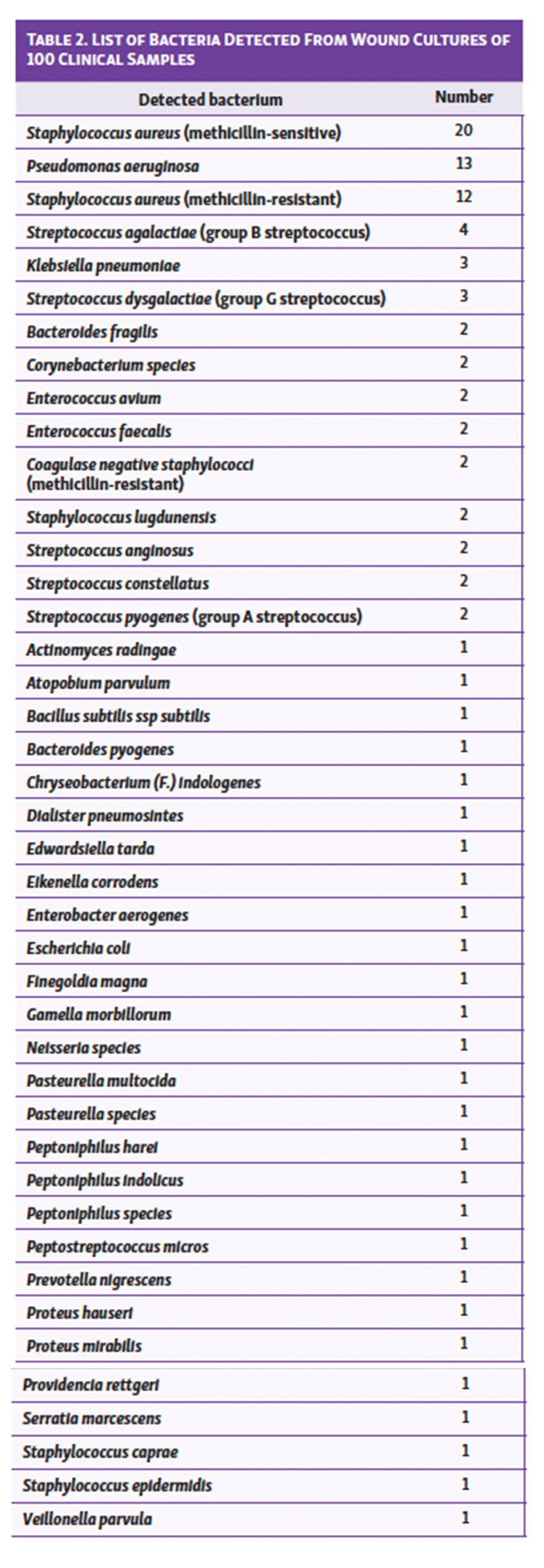 The detected bacteria are shown in Table 2. Staphylococcus aureus and Pseudomonas aeruginosa were frequently isolated, and 3 samples of group G streptococcus (GGS) and 4 samples of group B streptococcus (GBS) were included. None of the samples showed cross-reactions in the GAS-RADT. One patient with GAS and 3 patients with GGS had the onset of severe NSTIs (Table 3), which we reported in detail in our previously published study (Figure 1).7,8 One patient with GGS had diabetes mellitus; however, the other patients with GAS and GGS did not have diabetes or peripheral arterial disease. The patient whose samples showed a discrepancy between RADT and wound culture results (RADT-positive and wound culture-negative) is described below in detail.
The detected bacteria are shown in Table 2. Staphylococcus aureus and Pseudomonas aeruginosa were frequently isolated, and 3 samples of group G streptococcus (GGS) and 4 samples of group B streptococcus (GBS) were included. None of the samples showed cross-reactions in the GAS-RADT. One patient with GAS and 3 patients with GGS had the onset of severe NSTIs (Table 3), which we reported in detail in our previously published study (Figure 1).7,8 One patient with GGS had diabetes mellitus; however, the other patients with GAS and GGS did not have diabetes or peripheral arterial disease. The patient whose samples showed a discrepancy between RADT and wound culture results (RADT-positive and wound culture-negative) is described below in detail.

Case Description

A 58-year-old man was admitted to our hospital on a Saturday night because of high fever and edema of the right lower leg. The patient had no history of diabetes or peripheral arterial disease. On physical examination, temperature was 101.3 °F (38.5 °C), pulse was 95/min, blood pressure was 122/83 mm Hg, and oxygen saturation was 99% on room air. The right dorsum and around the lateral malleolus area showed erythema, fever, and tenderness. The verbal rating scale for pain was 3 (severe pain). No traumatic wound or episode was found at the right leg. The doctor on duty diagnosed cellulitis, and the on-call surgical wound care team was not consulted. Laboratory testing including complete blood count showed hemoglobin of 14.2 g/dL, platelet count of 161,100/µL, leukocyte count of 27,000/µL, plasma= glucose of 163 mg/dL, serum sodium of 132 mEq/L, serum creatinine of 1.36 mg/dL, serum C-reactive protein of 43.3 mg/dL, and serum creatine kinase of 4692 IU/L. Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score was 10. The surgical wound care team was not contacted. To manage the cellulitis, ceftriaxone, 2 g once daily, was begun. Acetaminophen was administered intravenously for controlling severe pain.

Two days later (the following Monday), the patient’s severe pain and fever persisted, and the surgical wound team was consulted. The right ankle was incised to obtain samples from the subcutaneous layer for a GAS-RADT and wound culture (Figure 2). Results of the GAS-RADT were positive; however, the wound culture did not detect any bacteria. Four sets of blood cultures showed GAS positivity.
The incised wound was washed by saline once or twice daily, and sulfadiazine silver cream was used externally. Antibiotics treatment was changed to Meropenem (0.5 g, 3 times/day) and Clindamycin (600mg, 2 times/day). Fortunately, his life was saved, but gait disturbance persisted because of severe contracture and fixation of the ankle joint (Figure 3).
Discussion
A recent meta-analysis on GAS pharyngitis indicated the high diagnostic accuracy of the GAS-RADT (sensitivity, 86%; specificity, 96%).9 NSTI progresses very rapidly and is life-threatening. While a pharyngeal kit can reportedly be used for wounds to aid in the diagnosis in the early phase, no reports have determined its accuracy. This study is the first to examine wounds from clinical samples in a large number of cases. The reproducibility between the GAS-RADT and wound culture showed statistically excellent agreement beyond chance.
None of the bacteria from the sampled wounds showed cross-reactional influences. Furthermore, other streptococci, including group B (agalactiae), group G (dysgalactiae), anginosus, and constellatus, were all GAS-RADT–negative. These results indicated the reliability of the GAS-RADT for managing wounds. The only case of discrepancy between RADT and wound culture occurred in a sample from a patient who had received ceftriaxone for 2 days. We suspected that the RADT detected the bacterial residue of destroyed GAS, while the wound culture failed to grow bacteria because the GAS had been inactivated by antibiotic therapy. This was also a novel finding and a pitfall to be recognized.
GAS is not always the causative organism in NSTI. Therefore, having a negative test does not mean that the patient will not require emergency surgery. Also, diagnoses for immediate debridement should be made based on comprehensive physical and laboratory findings, including the LRINEC score. However, GAS-NSTI is sometimes quite difficult to diagnose because the physical signs in the initial stage of infection can be nonspecific, limited to tenderness, erythema, and a fever.10 The RADT for GAS is effective in helping to determine the need for careful observation and possible debridement surgery even if there are few clinical signs. In this study, we diagnosed 5 cases of non-GAS NSTIs, including 3 cases of GGS-induced NSTI8 and 2 cases of non-clostridial gas gangrene induced by anaerobic bacteria. The advent of GGA- and GGS-RADT may improve outcomes in patients with GGA- and GGS-related NSTIs through more efficient diagnostics and better targeted therapies.
Limitations
This study was limited by a relatively small number of wound samples. Multiple GAS-NSTI cases are needed for a future study to elucidate the sensitivity and specificity of GAS-RADT.
Conclusions
To our knowledge, this is the first study to evaluate the reliability of GAS-RADT by comparing the reproducibility of its results versus wound culture. The GAS-RADT of wounds can be used with a reliability similar to that seen with RADT use in diagnosing bacterial pharyngitis.
Acknowledgments
Affiliations: 1Department of Plastic and Reconstructive Surgery, Graduate School of Medicine, Kyoto University, Kyoto, Japan; 2Department of Dermatology, Ijinkai Takeda General Hospital, Kyoto, Japan; 3Tsukuba Research Institute, Research and Development, Sekisui Medical Co., Ltd., Ibaraki, Japan
Correspondence: Itaru Tsuge, MD, PhD; itsuge@kuhp.kyoto-u.ac.jp
Funding: This work was funded by Sekisui Medical Co, Ltd. (Tokyo, Japan).
Ethics: The study involving human participants were reviewed and approved by the Kyoto University Medical Ethics Committee (R2417) and Takeda Hospital Group Ethics Committee (20200009). The patients provided their written informed consent to participate in this study.
Disclosures: The authors signed a joint research agreement with Sekisui Medical Co, Ltd.
References
1. Lamagni TL, Darenberg J, Luca-Harari B, et al. Epidemiology of severe streptococcus pyogenes disease in Europe. J Clin Microbiol. 2008;46;2359-2367. doi:10.1128/JCM.00422-08
2. Hietbrink F, Bode LG, Riddez L, et al. Triple diagnostics for early detection of ambivalent necrotizing fasciitis. World J Emerg Surg. 2016;11:51. doi:10.1186/s13017-016-0108-z.
3. Ault MJ, Geiderman J, Sokolov R. Rapid identification of group A streptococcus as the cause of necrotizing fasciitis. Ann Emerg Med. 1996;28;227-230. doi:10.1016/s0196-0644(96)70065-3
4. Bourgeois SD, Bourgeois MH. Use of the rapid streptococcus test in extrapharyngeal sites. Am Fam Physician. 1996;54;1634-1636.
5. Tsuge I, Yamanaka H, Katsube M, et al. Avoiding over-indication for surgical debridement using a rapid antigen detection test of group A streptococcus. Plast Reconstr Surg Glob Open. 2021;9;e3548. doi:10.1097/GOX.0000000000003548
6. Fleiss JL. Statistical Methods for Rates and Proportions. 2nd ed. John Wiley and Sons; 1981:218.
7. Tsuge I, Matsui M, Takeda T, et al. Less-invasive treatment for group A streptococcal fasciitis with rapid antigen detection test and collagen/gelatin sponge. Plast Reconstr Surg Glob Open. 2021;9;e3793. doi:10.1097/GOX.0000000000003793
8. Tsuge I, Matsui M, Yamanaka H, et al. Group G streptococcal necrotizing soft tissue infection: A pitfall of using a rapid antigen detection test for group A streptococcus. Eplasty. 2022;22:e7.
9. Lean WL, Arnup S, Danchin M, Steer AC. Rapid diagnostic tests for group A streptococcal pharyngitis: a meta-analysis. Pediatrics. 2014;134;771-781.
10. Rausch J, Foca M. Necrotizing fasciitis in a pediatric patient caused by Lancefield group G streptococcus: case report and brief review of the literature. Case Rep Med. 2011;2011;671365. doi:10.1155/2011/671365