Peer Reviewed
Prediction of Intra-abdominal Adhesions and Uterine Scar Grade Based on Abdominal Scar Characteristics in Women With a Previous Cesarean Section: A Diagnostic Accuracy Study
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Background. This study aims to investigate the relationship between cutaneous scar morphology and severe intra-abdominal adhesions and to predict uterine scar grade in repeat cesarean sections. It could be a valuable tool to plan elective repeat cesarean sections in patients with predicted weak uterine scars and also to have an experienced surgeon for repeat cesareans in patients predicted to have dense intra-abdominal adhesions.
Methods. Preoperatively, the external scar was assessed using the Manchester score in 260 women. Intraoperatively, the Knightly score was used for adhesions at 5 different sites. The total adhesion score was categorized into scores ≤5 and >5 (severe adhesions). The uterine scar was graded using the Qureshi method and grouped into intact scar and weak scar (grades 3 and 4). Fischer exact and chi-square tests were used to compare the groups. The receiver operating characteristic curve calculated a cutoff score for predicting severe adhesions and weak scars.
Results. Of the 260 patients, 63.5% had adhesions and 36.5% had no adhesions. The distortion of the skin scar had 71.3% specificity, and the texture had 84.8% sensitivity in predicting severe adhesions. Similarly, the texture had 72.2% sensitivity, and the distortion had 68.3% specificity in predicting weak uterine scar. A Manchester Scar Scale score of 9 includes the area under the curve of 0.72 for predicting severe adhesions and 0.62 for predicting weak uterine scar. A score of 9 was 66.6% sensitive and 66.5% specific, with a negative predictive value (NPV) of 93.2% for predicting severe adhesions. The same score was 55.5% sensitive and 65.1% specific, with an NPV of 90.1% for predicting weak uterine scar.
Conclusions. A Manchester Scar Scale cutoff score of 9 has a high NPV for predicting severe adhesions and weak uterine scar. The texture had high sensitivity, and distortion had high specificity for predicting severe adhesions.
Introduction
Cesarean delivery is a common obstetric surgery worldwide. Repeat cesarean section (CS) is the second most common indication for CS, which has increased in prevalence, especially in developing countries.1,2 Repeat CS can cause difficulty in abdominal entry, reflecting bladder, bleeding, and other intraoperative complications,3 including difficulty in delivering the baby.4
Inflammation during the surgery releases cytokines, chemokines, and growth factors. Inflammation recruits immune cells and activates fibroblasts, causing collagen deposition and scarring. Other factors, such as improper surgical technique, infection, or inadequate blood supply to the wound site, may interfere with routine wound healing. Impaired wound healing mechanisms, such as failure of the resorption of the fibrin clot, contribute to the formation of adhesions.5 Adhesion formation may be predisposed by abnormal scar tissue formation with excessive collagen deposition or inadequate remodelling.6
Skin scar and adhesion formations are wound-healing processes and share biological similarities.7 There may be long-term complications associated with adhesions.8-10 Before planning a repeat CS, it is essential to foresee this issue. This may aid in choosing an experienced surgeon to perform the surgery.
Although clinical and radiological methods for predicting adhesions are described in the literature, this clinical study aims to investigate the potential relationship between cutaneous scar characteristics and underlying severe intra-abdominal adhesions. Very few authors have investigated the relationship between adhesions and the morphology of skin scars. This knowledge can help in counselling the patient regarding added intraoperative morbidity due to adhesions.
With this information, our study will further help to analyse the possibility of predicting uterine scar grade using the abdominal scar characteristics as a screening tool in preoperative assessment. Hence, preoperative prediction can help exclude the trial of labor after CS (TOLAC) if the uterine scar prediction is weak.
Methods and Materials
This diagnostic accuracy study (prospective cohort) was conducted in the Obstetrics and Gynaecology department at the Women and Children Block of the Jawaharlal Institute of Postgraduate Medical Education & Research (JIPMER). JIPMER is a tertiary care teaching hospital in Puducherry, South India. Pregnant women with one previous CS delivery undergoing repeat CS (elective or emergency) at term were included. Our primary objective was to find dense adhesions, and prediction of uterine scar grade was the secondary objective in women undergoing repeat CS. Women with previous classic uterine incision, previous laparotomy/laparoscopy/myomectomy, immunosuppressed individuals, placenta previa, morbidly adherent placenta, known endometriosis, and connective tissue disorders were excluded. We did not exclude women with previous obstructed labor/second-stage CS, previous intrapartum/postpartum sepsis, secondary resuturing of the wound, and wounds healed by secondary intention. In such situations, the cutaneous scar can be thickened due to healing by secondary intention. Therefore, it was necessary to include them in the study of the prediction of intra-abdominal adhesions. We used the Manchester Scar Scale to assess the scar characteristics. The Manchester Scar Scale is a component scoring system used to assess the characteristics of a surgical scar, particularly in the context of CS scars. It considers color, contour, texture, distortion, and whether the scar is matte or shiny (Figure 1). Except for matte/shiny, each parameter is assigned a score ranging from 1 to 4, with higher scores indicating more significant scar abnormalities.11
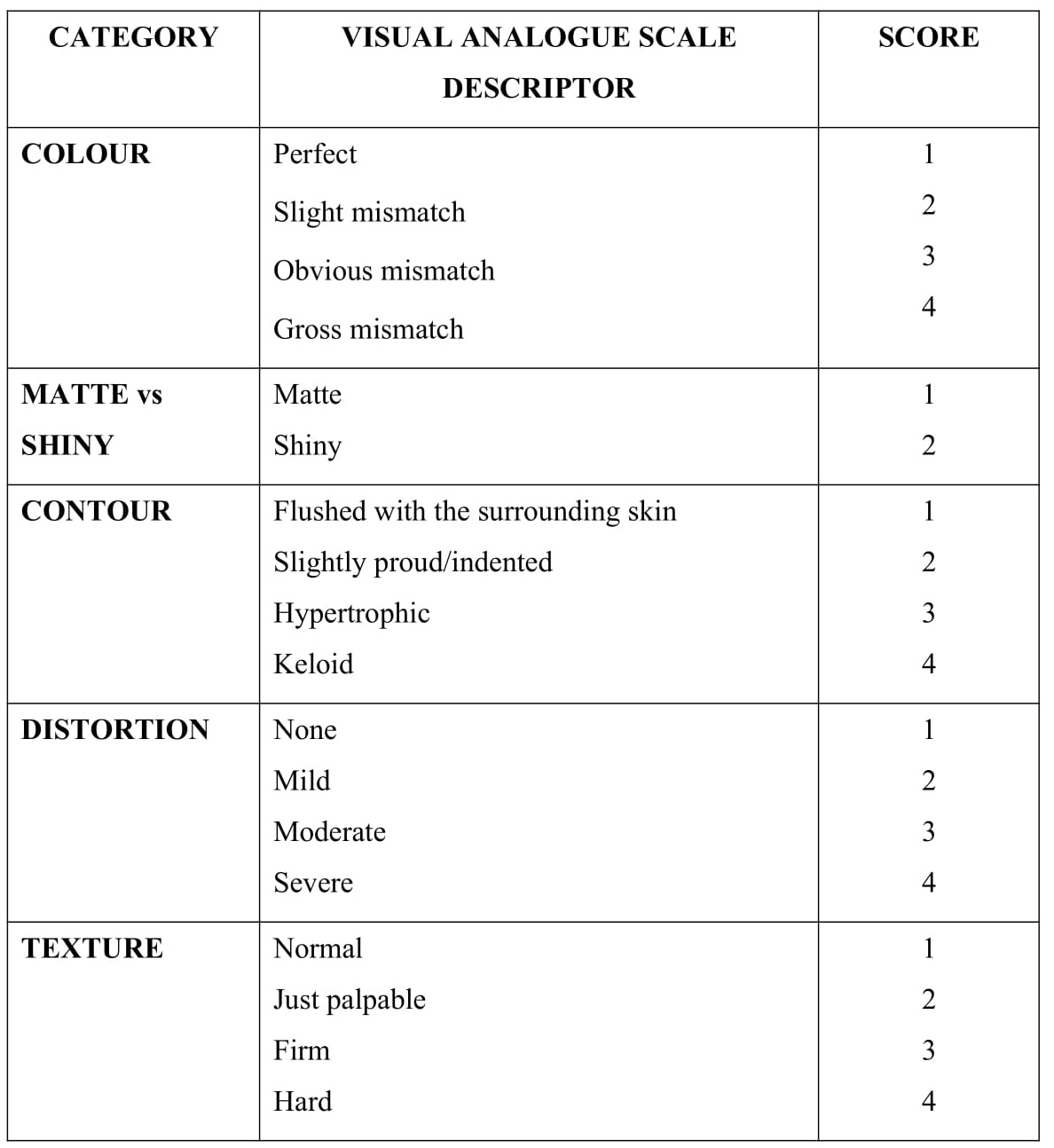
Figure 1. Manchester Scar Scale scoring.
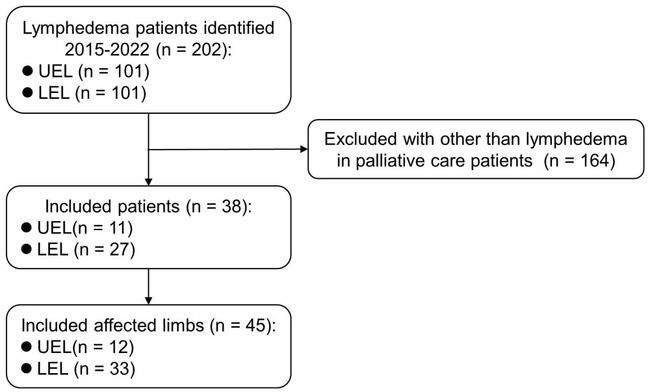
The sample size was calculated for the primary objective of predicting intra-abdominal adhesions. Kahyaoglu et al12 used width and pigmentation of the cutaneous scar characteristics and found that 25% of the study population had severe intra-abdominal adhesions for any area under the curve (AUC) of 0.6 based on skin scar characteristics. Thus, for 80% power and α-error of 5%, 260 patients were required. Institutional ethical committee clearance was obtained, and the participants’ written informed consent was given. The details of the socio-clinical profile of the woman, previous surgery, and postoperative period were collected from the patient or available documents. Figure 2 shows the study flow diagram. Preoperatively, before the CS, the external abdominal scar was scored as per the Manchester Scar Scale, which includes 5 components, and the score ranges from 5 to 18. Intraoperatively, the adhesions were scored based on the Knightly scoring system at 5 different sites: between the abdominal wall and uterus, abdominal wall and omentum, rectus sheath and muscle, uterus and omentum, and the uterus and bladder.
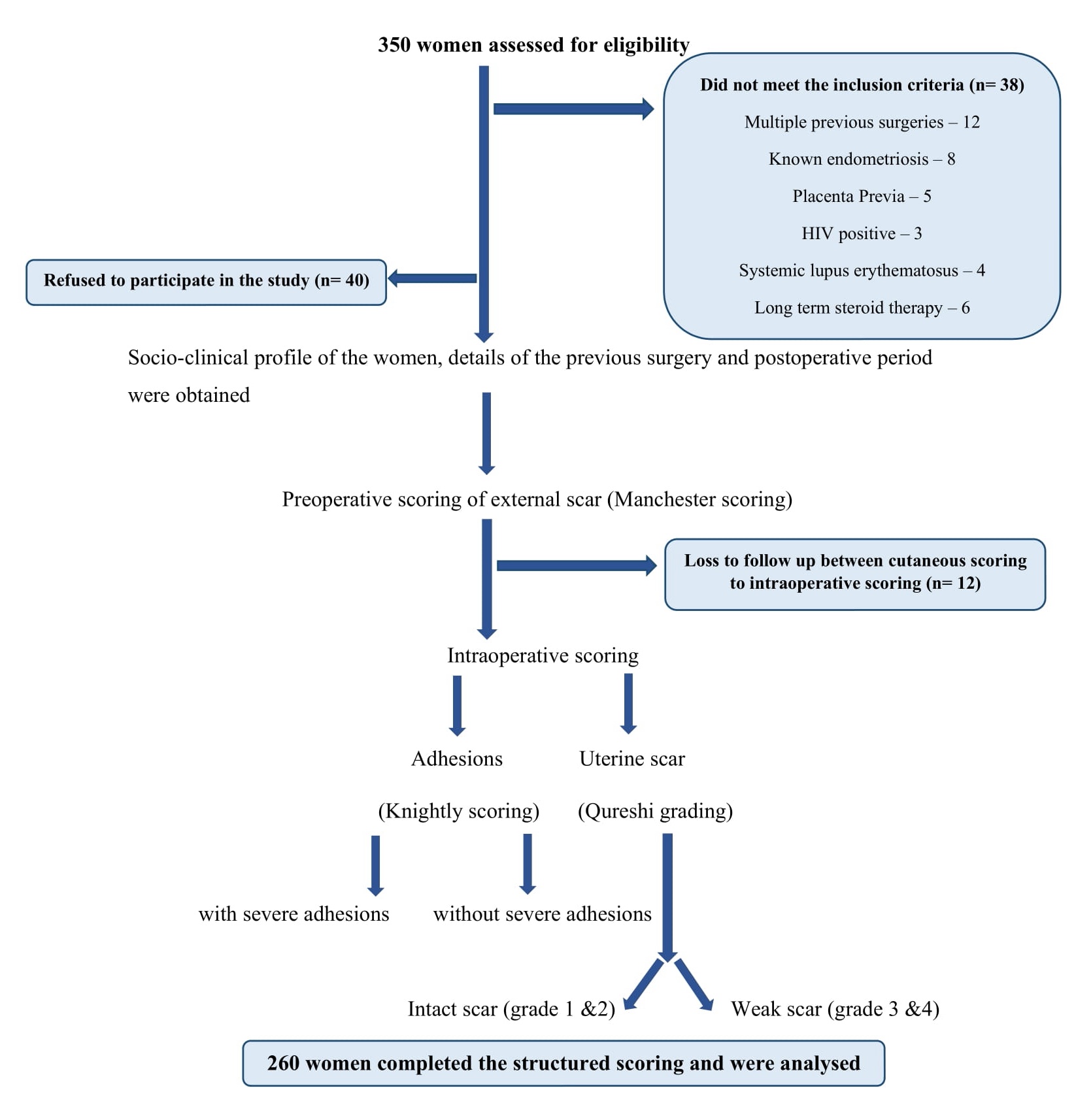
Figure 2. Flow diagram of the study.
The Knightly scoring system is a grading system used to evaluate the severity of intra-abdominal adhesions. The scoring system assigns a score ranging from 0 to 4 based on the extent and difficulty of separating adhesions. A score of 0 indicates no adhesions, while higher scores reflect the increasing severity of adhesions (Figure 3).13 Applying the Knightly score at 5 different sites, the total adhesion score ranges from minimum of 0 and maximum up to 20. We categorized the total adhesion score into a score ≤5 (no or mild adhesions) and a score >5 was considered as severe adhesions (the number and extent of adhesions at the various sites mentioned above).
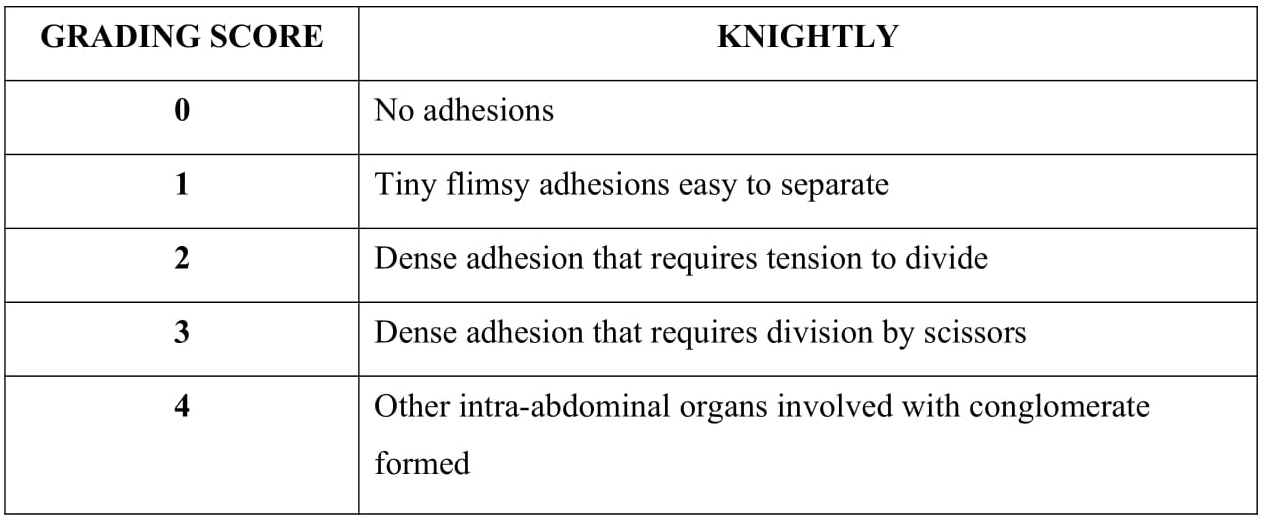
Figure 3. Knightly adhesions grading score.
The nature of the lower uterine segment (LUS) scar was graded according to the Qureshi scoring system14 and grouped into women with intact scars (grades 1 and 2) and women with weak uterine scars (grades 3 and 4). The system assigns a grade between 1 and 4 based on specific criteria concerning the appearance and integrity of scars. Grade 1 LUS is well-formed, while grade 2 LUS is thin and intrauterine contents cannot be seen. A grade 3 scar is paper-thin, with intrauterine contents visible, while a grade 4 scar is dehisced or ruptured. The reference standard in the 3 scoring systems required clinical evaluation and assessment by experienced medical experts familiar with scar characteristics. Despite many scoring systems available in the literature, these 3 were adopted as reference standards because the parameters in these scoring systems are clinical and more accessible to apply. Two different evaluators scored pre- and intraoperatively to avoid bias. Inter-rater reliability ensured scorer agreement. If an index test or reference standard result is indeterminate, the test was repeated to see if a conclusive result could be obtained. This helped reduce uncertainty and improve diagnostic accuracy.
We used both descriptive and analytical statistics to analyze data from participants. Continuous variables (age, body mass index, gestational age, time since last CS) were summarized with mean and standard deviation, while categorical variables (previous postoperative infection, suture material, etc) were expressed as proportions and analyzed with chi-square and Fisher exact test. The Manchester Scar Scale score's performance in predicting intra-abdominal adhesion severity was evaluated using the receiver operating characteristic (ROC) curve and AUC. The diagnostic accuracy was expressed in sensitivity, specificity, positive and negative predictive value, and positive and negative likelihood ratio. Multivariable logistic regression identified factors associated with maximum predictive risk. STATA software version 14.2 was used for analysis.
Results
We screened 350 women undergoing repeat CS at term, and 260 women satisfied the eligibility criteria and were recruited (Figure 2). About 208 women (80%) had emergency CS. Sociodemographic details are presented in Table 1. The distribution of the study population based on the Manchester Scar Scale score of the skin scar is detailed in Table 2.
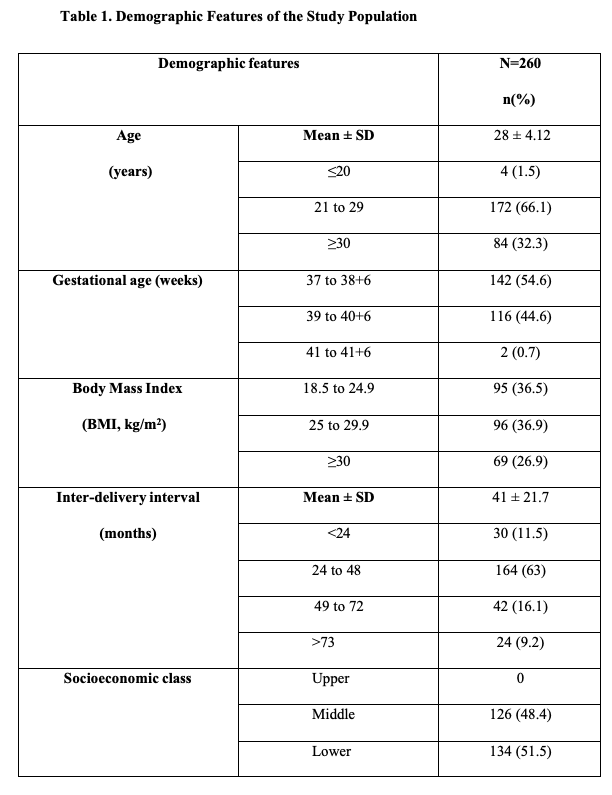
BMI, body mass index.
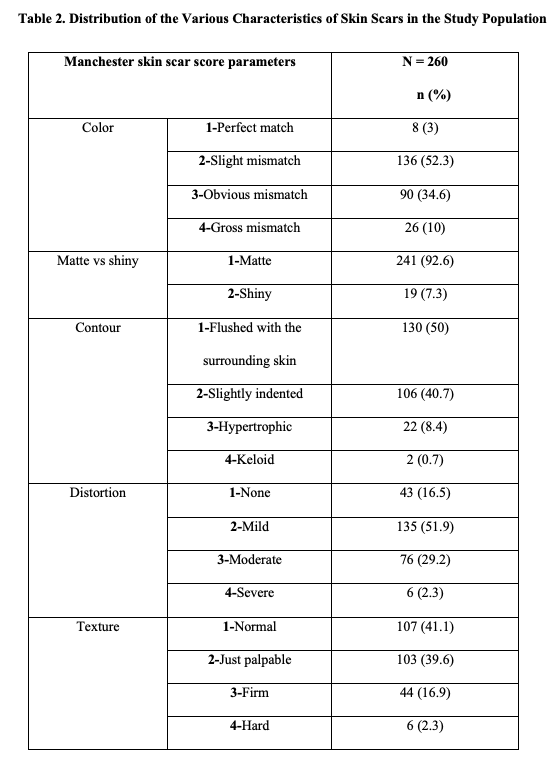
Table 3 represents the distribution of the study group based on adhesions, using the Knightly score, at 5 different sites. The table displays the adhesion grading score for each site, with the number and percentage of participants falling into each score category. Nearly 165 (63.5%) had intra-abdominal adhesions, and 95 (36.5%) did not have adhesions. Among them, 133 (80%) had mild adhesions. The most common adhesion site was between the uterus and bladder, observed in 106 (40.7%) individuals. A weak uterine scar of Qureshi grade 3 and 4 was observed in 36 individuals (13.8%). There were 12 women (4.6%) with scar dehiscence. Among them, 8 were allowed TOLAC, and 4 underwent direct repeat pre-labor CS. The patients who had dehiscence had silent asymptomatic dehiscence with no perinatal mortality or cesarean hysterectomy.
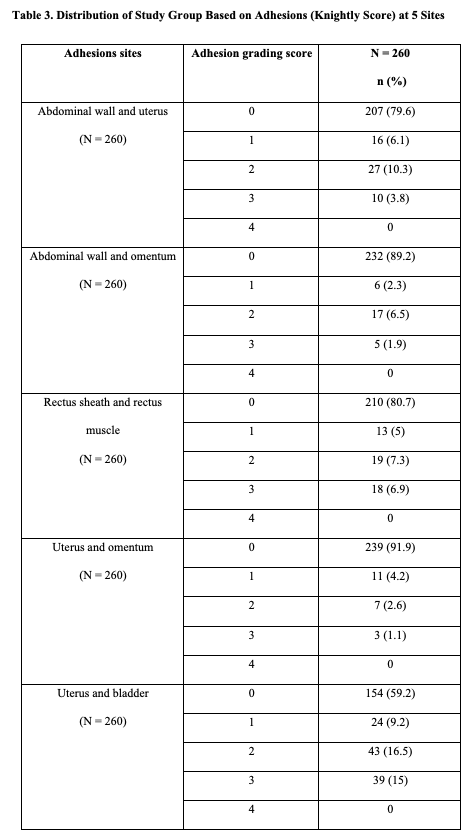
0, no adhesions; 1, tiny, flimsy adhesions that are easy to separate; 2, dense adhesion that requires tension to divide; 3, dense adhesion that requires division by scissors; 4, other intra-abdominal organs involved with conglomerate formed.
Abdominal scar characteristics
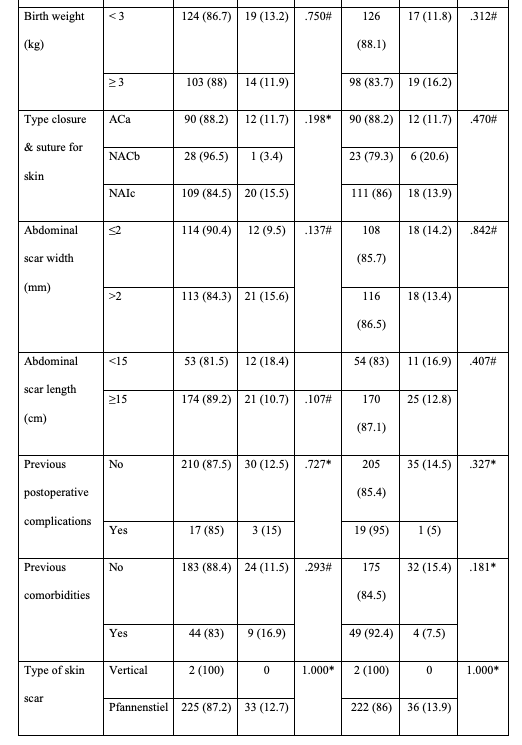
The study found a significant association between color mismatch and higher adhesion severity scores (P = .035). In comparing matte and shiny scars, shiny scars were associated with a higher uterine scar grade (P = .020). Scars with contour abnormalities were significantly associated with higher adhesion severity scores (P < .001). Scars with moderate to severe distortion were likelier to have higher adhesion severity scores (P = .016). The abnormal texture was associated with higher adhesion severity scores (P < .001) and higher uterine scar grades (P = .007).
On univariate analysis, a lower age was significantly associated with a weak uterine scar grade (χ2 = 4.89, Fischer exact P = .042). Table 4 compares previous CS characteristics with the adhesion score and uterine scar grade in the study group. It presents the descriptive statistics of the participants in each category for the Knightly score and Qureshi grade. We found a significant association between postoperative complications such as fever, bowel distension, prolonged catheterization, and the degree of adhesions (χ2 = 17.477, P < .001).
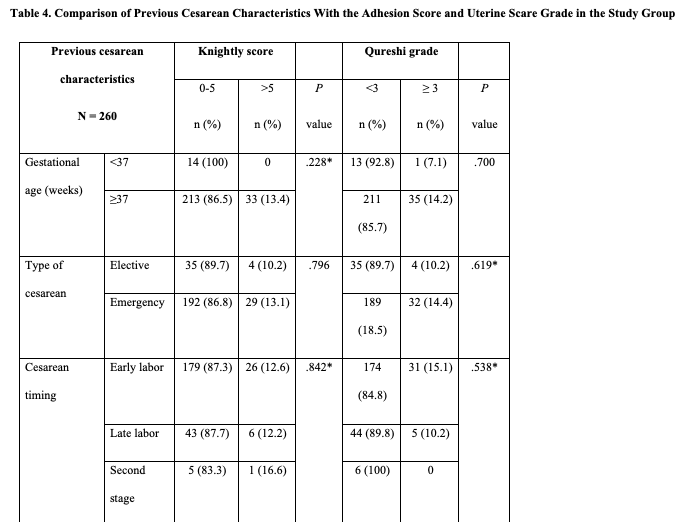
ACa, absorbable continuous; NACb, non-absorbable continuous; NAIc, non-absorbable interrupted
Prediction of adhesions and uterine scar grade
Table 5 compares the Manchester Scar Scale score parameters with the adhesion severity score and uterine scar grade in the study group. Four out of 5 features of the Manchester Scar Scale score had significantly higher scores in women with severe adhesions than women with no or flimsy adhesions. The distortion of the skin scar had the highest specificity (71.3%), and texture had the highest sensitivity (84.8%) in predicting severe intra-abdominal adhesions. Similarly, the texture had the highest sensitivity (72.2%), and the distortion had the highest specificity (68.3%) in predicting weak uterine scar.
N, frequency; *, Fisher’s exact test; #, Pearson chi-squared test
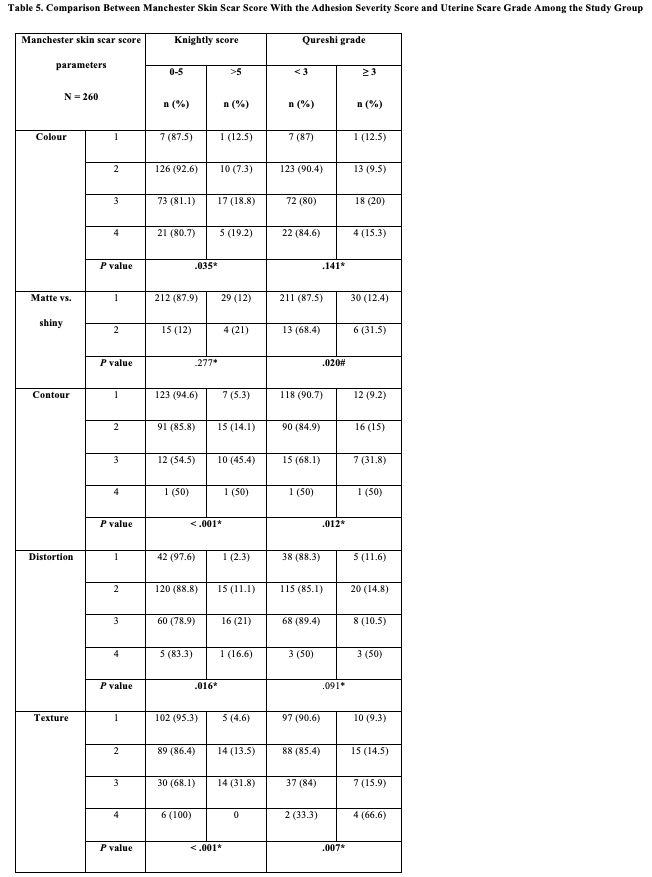
A ROC curve was plotted against the total Manchester Scar Scale score vs adhesion score and uterine scar grade. A cutoff for an abdominal scar of 9 included an AUC of 72% in predicting severe intra-abdominal adhesions (Figure 4) and 60% for weak uterine scar (Figure 5). A cutoff score of 9 was 66.6% sensitive and 66.5% specific, with a negative predictive value (NPV) of 93.2% for predicting severe intra-abdominal adhesions (Table 6). The exact cutoff score was 55.5% sensitive and 65.1% specific, and an NPV of 90.1% in predicting weak uterine scar. Though the sensitivity and specificity of predicting severe adhesions and weak uterine scar are lower, both have a high NPV for a cutoff Manchester Scar Scale score of 9. Positive likelihood ratio values range from 1.534 to 1.999, indicating that a positive total Manchester Scar Scale score does increase the odds of adhesions being present, but the effect is not very strong. In contrast, the negative likelihood ratios are generally close to 1 or even 0. This suggests that a negative total Manchester Scar Scale score does not significantly change the odds of absent adhesions. In other words, a negative test result may need to be more informative in ruling out the presence of adhesions.
Figure 4. The ROC curve of Manchester Scar Scale score versus total adhesion score.
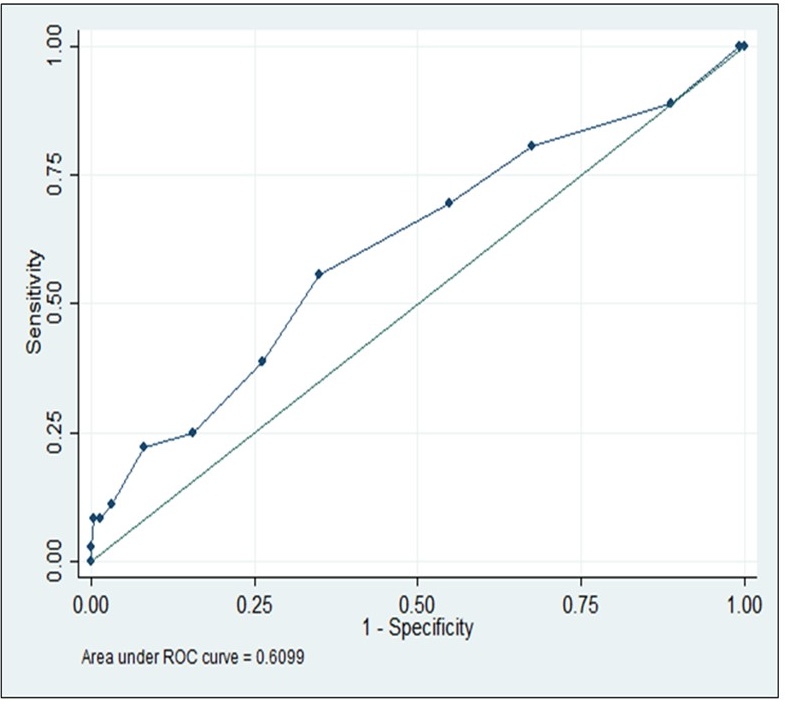
Figure 5. The ROC curve of Manchester Scar Scale score versus Qureshi uterine scar grade.
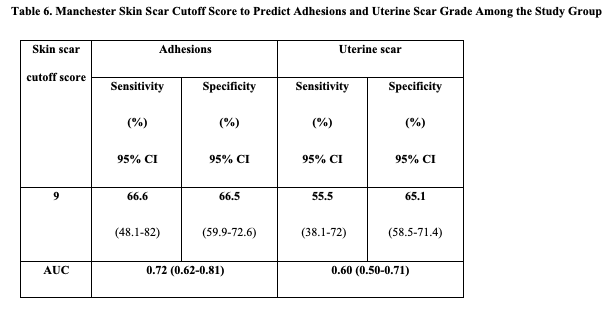
AUC, area under the curve; CI, confidence interval.
Discussion
This prospective cohort study assessed the ability of external skin scar features to predict intra-abdominal adhesions and uterine scar grade. We observed adhesions in 165 (64%) of our cases. We found that 106 participants (64%) had adhesions between the uterus and bladder. A relatively similar observation was seen by Kokanali et al,15 where 79.3% of the adhesions were in the upper aspect of the bladder, followed by 73.2% over the anterior uterine surface. We did not find any association of previous CS variables with intra-abdominal adhesions. Similar to our study, other authors found no significant association between previous CS details and intra-abdominal adhesions.16-19 We found a significantly higher risk of weak uterine scar in young women <20 years of age (χ2 = P < .042). This could be because women <20 years would have a short interpregnancy interval. No other demographic factor or previous CS characteristic was found to be associated with a weak uterine scar.
Various classifications of the abdominal scar have been proposed. The simplest has been flat and non-flat skin scars.20 The Vancouver Scar Scale scoring includes pliability, vascularity, pigmentation, and height. Some studies also considered the length and width of the scar.15,21 We applied the Manchester Scar Scale scoring system. Many authors have used this scoring method, including Enes Taylan,22 Stocker,23 and Kokanali.15
There were 3 bladder injuries due to severe adhesions in our study. A 4 times higher risk of bladder injury has been reported in repeat CS, mainly while reflecting the bladder flap in 95%.3 Our study found a significant association between adhesion-related postoperative complications such as fever, bowel distension, prolonged urinary catheterization, and the degree of adhesions. Yadav et al made a similar observation.24
Few authors have explored the predictability of intra-abdominal adhesions based on the scar characteristics of the abdominal skin. We observed that a cutoff Manchester Scar Scale score for an abdominal scar of 9 included an AUC of 72%, predicting severe intra-abdominal adhesions, and 60% in the weak uterine scar. A cutoff skin score of 9 had an NPV of 93.2% in predicting severe intra-abdominal adhesions and an NPV of 90.1% in predicting weak uterine scar. We observed a significant association of color, contour, texture, and distortion of the scar with adhesions. Enes Taylan et al22 made a similar observation and concluded that the color of the scar was the most significant component of the score. A few studies have shown a positive correlation between depressed scars and adhesions.24,25 A meta-analysis showed that a depressed scar was positively associated with adhesions, and an elevated or pigmented scar could not significantly predict adhesions.10 We considered a depressed scar a distortion component and scored it as such.
Stocker et al23 observed that 33% of women had significant adhesions when the scar length was more than 5 cm, but in our study, 195 (75%) women had scar length ≥15 cm and had no association with adhesions. Kahyaoglu et al12 observed a scar width of 2.5 mm as a predictor of adhesions. However, our study had 134 (51.5%) women with scar width >2 mm, and adhesions were not associated. A study reported that a wider scar width could predict intra-abdominal adhesions, but the sensitivity and specificity were 49% and 81%, respectively.26 Similar to our research, Salim et al16 also found no association between the length of skin scar with intra-abdominal adhesions. The myometrium is a 3-layer structure containing smooth muscles arranged as outer longitudinal, middle criss-cross pattern arrangement, and inner circular fibers.27 Thus, the healing occurs at 3 levels following an approximation of the wound. The literature on predicting uterine scars based on skin scar features is limited. A study by Al Naimi et al28 compared the external skin scar, scored by the Manchester Scar Scale, and the uterine scar thickness (residual myometrial thickness) measured by transvaginal ultrasound after 12 to 24 months post-cesarean. Their median residual myometrial thickness was 55.8%, and they found that the Asian ethnic origin had a significantly higher Manchester Scar Scale score but did not substantially affect the residual myometrial ratio. In our study, the matte, contour, and texture of the skin scar had considerably higher predictability in women with a weaker uterine scar.
There is a lack of literature correlating the skin scar characteristics with the uterine scar grade and predicting weak uterine scar based on external scar features; however, this needs further exploration. Our study had the strengths of adequate sample size, a homogenous population of women with previous one CS at term, excluding women who had prior surgeries or medical conditions, single observer scoring of the skin scar, and adhesions at various essential sites relevant during the repeat CS were studied. The limitations of our study are that almost all the cases were with previous CS, and the upper-abdomen adhesions could have been missed. Therefore, many cases of Knightly grade 4 could not be assessed. Many of our previous CS details were based on recall by the patients. We did not study the symptomatology of the patients as a possible predictor for adhesions. Hence, we recommend more extensive studies on the same topic to overcome these limitations.
The distortion component of the Manchester Scar Scale score had 71% sensitivity and 85% specificity for predicting severe intra-abdominal adhesions. The Manchester Scar Scale cutoff score had an AUC of 0.7 and had an NPV of 93.2% for abdominal adhesions. A cutoff score of 9 has an AUC of 0.72 in predicting intra-abdominal adhesions. Study findings suggest that these scores can be valuable in clinical practice for assessing abdominal scar characteristics and predicting intra-abdominal adhesions and uterine scar grade among women undergoing repeat CSs. We studied a homogenous population of women with one previous CS, and component scoring for the external scar was used, which helped to assess the predictive value of each component of the score.
Limitations
The collection of socio-clinical profiles, details of previous surgery, and postoperative period relied on participant recall or available documents, which may introduce recall bias or incomplete information. Information about the technique, type of suture material used for uterine closure, or use of anti-adhesion barriers at first CS is needed. Most cases were with previous CS, and the upper-abdomen adhesions could have been missed. Therefore, many cases of Knightly grade 4 could not be assessed, and we did not study the symptomatology of patients as a possible predictor of adhesions. The study included 260 participants, which may limit the precision and generalizability of the results. The accuracy of these assessments depends on the skill and experience of the assessors, which may introduce inter-rater or intra-rater variability and potential bias.
Conclusions
The Manchester Scar Scale cutoff score of 9 has a high NPV of 93.2% for abdominal adhesions and a high NPV of 90.1% for weak uterine scar. The texture had 85% sensitivity, and distortion had 71% specificity for predicting severe intra-abdominal adhesions. Calculating a cutoff score for the Manchester Scar Scale scoring system to predict adhesions improves preoperative planning, individualized patient counseling regarding complications, and shared decision-making, ultimately leading to enhanced patient care and outcomes.
Acknowledgments
Authors: Vignesh Durai, MS; Gowri Dorairajan, MD, DNB
Affiliation: Department of Obstetrics and Gynaecology, Jawaharlal Institute of Postgraduate Medical Education & Research (JIPMER), Puducherry, India
Correspondence: Gowri Dorairajan, MD, DNB; gowridorai@hotmail.com
The authors want to thank Dr Karthik Rajan from the Department of Preventive and Social Medicine, JIPMER, for helping in the statistical analysis of our study.
Ethics: Institutional ethical committee clearance was obtained, and the participants’ written informed consent was given.
Disclosures: The authors disclose no relevant financial or nonfinancial interests.
References
- Maskey S, Bajracharya M, Bhandari S. Prevalence of cesarean section and its indications in a tertiary care hospital. JNMA J Nepal Med Assoc. 2019;57:70-73. doi:10.31729/jnma.4282
- Dhakal Rai S, van Teijlingen E, Regmi PR, Wood J, Dangal G, Dhakal KB. Factors contributing to rising cesarean section rates in South Asian countries: a systematic review. Asian J Med Sci. 2022;13:143-174.
- Lyell DJ. Adhesions and perioperative complications of repeat cesarean delivery. Am J Obstet Gynecol. 2011;205:S11-S18. doi:10.1016/j.ajog.2011.09.029
- Tulandi T, Lyell DJ. Classification of intra-abdominal adhesions after cesarean delivery. Gynecol Surg. 2013;10:25-29.
- Ten Broek RPG, Stommel MWJ, Strik C, van Laarhoven CJHM, Keus F, van Goor H. Benefits and harms of adhesion barriers for abdominal surgery: a systematic review and meta-analysis. Lancet. 2014;383(9911):48-59. doi:10.1016/S0140-6736(13)61687-6
- Arung W, Meurisse M, Detry O. Pathophysiology and prevention of postoperative peritoneal adhesions. World J Gastroenterol. 2011;17(41):4545-4553. doi:10.3748/wjg.v17.i41.4545
- Linden J. Stocker, Jane E. Glazebrook, Ying C. Cheong, Are skin scar characteristics associated with the degree of pelvic adhesions at laparoscopy? Fertil Steril. 2014;101(2):501-505. doi:10.1016/j.fertnstert.2013.10.026
- Al-Took S, Platt R, Tulandi T. Adhesion related small bowel obstruction after gynecologic operations. Am J Obstet. 1999;180:313-315. doi:10.1016/s0002-9378(99)70205-x
- Hemminki E. Impact of cesarean section on future pregnancy: a review of cohort studies. Paediatr Perinat Epidemiol. 1996 Oct;10(4):366-379. doi:10.1111/j.1365-3016.1996.tb00062.x
- Murphy DJ, Stirrat GM, Heron J, ALSPAC Study Team. The relationship between caesarean section and subfertility in a population-based sample of 14 541 pregnancies. Hum Reprod. 2002 Jul;17(7):1914-1917. doi:10.1093/humrep/17.7.1914
- Beausang E, Floyd H, Dunn KW, Orton CI, Ferguson MWJ. A new quantitative scale for clinical scar assessment. Plast Reconstr Surg. 1998;102(6):1954-1961. doi:10.1097/00006534-199811000-00022
- Kahyaoglu I, Kayikcioglu F, Kinay T, Mollamahmutoglu L. Abdominal scar characteristics: do they predict intra-abdominal adhesions with repeat cesarean deliveries? Scar characteristics and adhesions. J Obstet Gynaecol Res. 2014;40:1643-1648. doi:10.1111/jog.12429
- Knightly JJ, Agostino D, Cliffton EE. The effect of fibrinolysin and heparin on the formation of peritoneal adhesions. Surgery. 1962;52:250-258.
- Qureshi B, Inafuku K, Oshima K, Masamoto H, Kanazawa K. Ultrasonographic evaluation of lower uterine segment to predict the integrity and quality of cesarean scar during pregnancy: a prospective study. Tohoku J Exp Med. 1997;183:55-65. doi:10.1620/tjem.183.55
- Kokanalı D, Kokanalı MK, Topcu HO, Ersak B, Tascı Y. Are the cesarean section skin scar characteristics associated with intra-abdominal adhesions located at surgical and nonsurgical sites? J Gynecol Obstet Hum Reprod. 2019;48(10):839-843. doi:10.1016/j.jogoh.2019.03.026
- Salim R, Kadan Y, Nachum Z, Edelstein S, Shalev E. Abdominal scar characteristics as a predictor of intra-abdominal adhesions at repeat cesarean delivery. Fertil Steril. 2008;90:2324-2327. doi:10.1016/j.fertnstert.2007.10.037
- Sham AA, Eskander M, Mubasher H. Cesarean section scar characteristics as a preoperative predictor of intra-abdominal adhesions. Med J Cairo Univ. 2015;83:167-171.
- Çim N, Elçi E, Güneş Elçi G, Almalı N, Yıldızhan R. Are the skin scar characteristics and closure of the parietal peritoneum associated with pelvic adhesions? Turk J Obstet Gynecol. 2018;15:28-32. doi: 10.4274/tjod.55491
- Kavya B, Manjulatha B. Prediction and correlation of presence and severity of intra-abdominal adhesions before caesarean delivery, a prospective study. IOSR J Dent Med Sci. 2020;19(3):40-43. doi:10.9790/0853-1903084043
- Elprince M, Taha OT, Ibrahim ZM, et al. Prediction of intraperitoneal adhesions using striae gravidarum and scar characteristics in women undergoing repeated cesarean sections. BMC Pregnancy Childbirth. 2021;21(1):286. doi:10.1186/s12884-021-03763-z
- Khalaf M, Abdel-Reheem F, El-Nashar I, Abbas AM, Khalifa MA. Cesarean skin scar characteristics for preoperative prediction of intra-abdominal adhesions at repeat cesarean delivery: a prospective cohort study. Annal Gynecol Obstet. 2020;4(1):72-76. doi:10.36959/468/469
- Taylan E, Akdemir A, Ergenoglu AM, Yeniel AO, Tekindal MA. Can we predict the presence and severity of intra-abdominal adhesions before cesarean delivery? Gynecol Obstet Invest. 2017;82:521-526. doi:10.1159/000454767
- Stocker LJ, Glazebrook JE, Cheong YC. Are skin scar characteristics associated with the degree of pelvic adhesions at laparoscopy? Fertil Steril. 2014;101(2):501-505. doi:10.1016/j.fertnstert.2013.10.026
- Yadav S, Kaur S, Yadav S, Thakur B. Analysis of cesarean rate, indications, and complications. Int J Reprod Contracept Obstet Gynecol. 2016;3326-3329.
- Pergialiotis V, Frountzas M, Siotos C, Karampetsou N, Perrea DN, Efthymios Vlachos D. Cesarean wound scar characteristics for the prediction of pelvic adhesions: a meta-analysis of observational studies. J Matern Fetal Neonatal Med. 2017;30:486-491. doi:10.1080/14767058.2016.1176135
- Jaafar ZAA, Obeid RZ, Salman DA. Skin markers and the prediction of intra-abdominal adhesion during second Cesarean delivery. Ginekol Pol. 2019;90(6):325-330. doi:10.5603/GP.2019.0059
- Myometrium - eAnatomy. IMAIOS. Accessed February 3, 2004. https://www.imaios.com/en/e-Anatomy/Anatomical-Parts/Myometrium
- Al Naimi A, Mouzakiti N, Eißmann C, Louwen F, Bahlmann F. Does the appearance of the cutaneous scar after cesarean section reflect the residual myometrial thickness? Arch Gynecol Obstet. 2021;303:847-851. doi:10.1007/s00404-020-05943-2