Results of a Single-Institution Quality Improvement Initiative to Reduce Perioperative Blood Transfusion During Open Complex Cranial Vault Reconstruction
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Background. Craniosynostosis repair via open complex cranial vault remodeling (OCCVR) is a complicated surgical procedure associated with morbidity and blood loss, often requiring blood transfusion. The Pediatric Craniofacial Collaborative group created the Pediatric Craniofacial Surgery Perioperative Registry (PCSPR) to capture data relating to the perioperative management of children undergoing craniofacial surgery. A tertiary pediatric hospital implemented its own quality improvement (QI) initiative with the aim of reducing blood transfusion volumes and exposures in patients undergoing OCCVR. The initiative included preoperative iron supplementation, intraoperative use of cell saver and tranexamic acid, maintenance of normothermia, and restrictive transfusion protocols.
Methods. Patients were included in the study if they had a diagnosis of craniosynostosis, were younger than 18 years, and underwent OCCVR. Patient demographics, comorbidities, and perioperative data were recorded using the PCSPR. Outcomes included blood transfusion volume, number of blood donor exposures, and intra and postoperative complications. Outcomes before and after the initiative were compared.
Results. The median perioperative allogenic blood transfusion volume decreased from 35 mL/kg pre-QI to 24 mL/kg post-QI (P < .001). There was a significant decrease in the number of blood donor exposures, and the number of patients who experienced a transfusion-free perioperative period increased from 10.9% to 19.6% (P = .037). There were no observed differences in perioperative complications, hospital and intensive care unit length of stay, or mortality.
Conclusions. This QI initiative has resulted in reduced blood transfusion volumes and reduced blood donor exposures without an increase in perioperative complications related to blood loss. Further multi-institutional research is necessary to create national standards for the anesthetic care of all patients undergoing OCVR.
Introduction
Blood is considered a therapeutic substance by the World Health Organization (WHO) and should be used judiciously due to its limited availability and potential for associated risks. Discussion of blood management strategies frequently accompanies craniosynostosis literature due to the high risk of hemorrhage during surgery.1 Craniosynostosis results from premature fusion of one or more cranial sutures and occurs in approximately 1 in 2000 live births.1,2 Children with significant deformities often require open complex cranial vault reconstruction (OCCVR), which includes total calvarial reconstruction, fronto-orbital advancement, and posterior cranial vault reconstruction.1 OCCVR is a high-risk procedure that requires intricate anesthetic management and a high degree of multidisciplinary care.3,4 The incidence of major perioperative complications is around 15%.5 Although complication rates have been decreasing, massive hemorrhage remains a serious concern.1
Reports from the Pediatric Perioperative Cardiac Arrest Registry demonstrate that the most common cardiovascular cause of cardiac arrest in children was hypovolemia, often from hemorrhage due to craniotomies.1 The large surgical surface area of the infant head, coupled with the need for multiple osteotomies, often leads to massive blood loss that exceeds the patient’s circulating blood volume.1,3,6 To counteract blood loss, the majority of patients receive allogeneic blood transfusions. Nationally, as many as 91% of pediatric patients younger than 24 months were transfused while undergoing CCVR, but there is variability in transfusion volumes between and within institutions.3 Numerous medical, legal, religious, and socioeconomic factors argue for decreasing or avoiding allogeneic blood transfusions.7,8 Medical complications associated with red blood transfusion are the most concerning, with 37 of every 100 000 infants having an adverse outcome, which is markedly higher than the adult complication rate (ie, 13:100 000).9,10 Efforts to reduce the need and volume of blood transfusions should be a priority of every institution.
Despite numerous efforts to reduce or eliminate the use of allogenic blood transfusions, there is not an evidence-based consensus on which option or combination of options is most effective, leading to variability in practice.11-13 Cell savers, which are used to collect and recycle a patient’s own blood lost during surgery, as well as antifibrinolytics such as tranexamic acid (TXA) have been identified as viable options to reduce perioperative blood transfusions.2,14-17 Various anesthetic management techniques such as controlled hypotension, acute nonmonomeric hemodilution (ANH), and preoperative administration of erythropoietin can also be employed.8,17,18 Active warming techniques to prevent hypothermia-induced coagulopathy are paramount.1 Additionally, the implementation of restrictive transfusion protocols has been shown to be safe and effective.19
Due to the heavy institutional burden of managing life-threatening complications associated with allogenic blood transfusions, we set out to implement a quality improvement (QI) initiative with the aim of reducing blood transfusion volumes and exposures in patients undergoing OCCVR. This QI initiative included preoperative oral iron supplementation, use of cell savers and TXA intraoperatively, maintenance of patient normothermia, and restrictive intraoperative transfusion guides.
We hypothesized that this combination of techniques would be associated with a decrease in allogenic blood transfusion without an increase in complications. Therefore, this QI initiative would improve the quality of care by decreasing the risks of blood transfusions and reducing high institutional costs related to using blood products and managing their complications. To evaluate the effectiveness of this QI initiative, we retrospectively analyzed the perioperative data of all patients undergoing OCCVR at a single institution before and after implementation of the QI initiative using the Pediatric Craniofacial Surgery Perioperative Registry (PCSPR).
Methods and Materials
Setting
This QI initiative was conducted at Johns Hopkins All Children’s Hospital (JHACH) after Institutional Review Board (IRB) approval (IRB00079926). Data from this study was sourced from the PCSPR, a multicenter, observational registry of perioperative data that contains practices and outcomes in children undergoing craniofacial surgery, with the ultimate goal of facilitating quality improvement efforts and optimizing care. The PCSPR is the largest pediatric craniofacial surgery registry worldwide and was developed by the Pediatric Craniofacial Collaborative Group (PCCG), a group of individuals representing 33 institutions interested in the care of children with craniofacial anomalies or defects, particularly craniosynostosis. JHACH is a participating member of the PCCG.
Initiative
At JHACH, a team of pediatric anesthesiologists, neurosurgeons, and plastic surgeons developed a QI initiative through expert opinion and literature review with the aim to reduce blood transfusion volumes and exposures in patients undergoing OCCVR. The QI initiative included preoperative oral iron supplementation, use of cell saver and TXA intraoperatively, maintenance of patient normothermia, and restrictive intraoperative transfusion guides. Preoperative oral iron supplementation, 3 mg/kg administered once daily, was started at each patient’s preoperative visit approximately 4 weeks prior to surgery. Intraoperatively, intravenous TXA was given as a loading dose of 10 mg/kg approximately 15 to 30 minutes before incision, followed by an infusion of 5 mg/kg/h. Intraoperatively, a C.A.T.Splus autotransfusion system (Frenius Kabi) was used. Collected blood was processed by the cell saver system and then infused intraoperatively. Patient temperatures were maintained at 35.5 °C or higher by placing them on a Bair Hugger (3M). Intraoperative transfusions were restricted to patients who had an intraoperative hemoglobin of 8 g/dL or less or were hemodynamically unstable, which was decided by the attending pediatric anesthesiologist and surgeon.
Patient population
Selection criteria included patients 18 years or younger with a diagnosis of craniosynostosis who underwent either a fronto-orbital advancement/anterior vault reconstruction, a mid/posterior vault reconstruction, or a total vault reconstruction at JHACH. Data was extracted from the PCSPR from June 2012 to December 2021. Baseline data from June 2012 to March 2016 (pre-QI) were established when the intraoperative management of OCCVR procedures was at the discretion of the attending anesthesiologist. The QI initiative was implemented from March 2016 to December 2021 (post-QI).
Outcomes
The primary outcome was the change in the total perioperative allogenic blood transfusion volume (mL/kg) intraoperatively and within the first 48 hours postoperatively. The secondary outcome was the change in the total amount of unique blood donor exposures within the same time period.
Statistical analysis
Patient demographics, comorbidities, and perioperative events were described with summary statistics using percentages and frequencies for categorical variables and medians and ranges (min, max) for continuous variables. Characteristics were compared pre- and post-QI initiative with 𝜒2 or Fisher exact tests for categorical variables and Mann-Whitney U tests for continuous variables, as appropriate. Two-sided P values of less than .05 were considered
Results
There were 97 patients included in this study. Forty-six patients underwent OCCVR pre-QI and 51 patients underwent OCCVR post-QI. There was a significant difference between both median age (7 vs 10 months, P = .004) and weight (8.6 vs 9.5 kg, P = .044) at the time of the procedure. Total vault reconstructions were the most common procedure performed pre-QI (n = 19, 41.3%), whereas fronto-orbital advancements were most commonly performed post-QI (n = 25, 49.0%); however, there was not a significant difference (P = .2). Overall, there was a low prevalence of patient comorbidities. Compared with pre-QI patients (n = 0), there was an increased prevalence of a history of prematurity in post-QI patients (n = 6, 11.8%; P = .028), as well as developmental delay/impaired cognitive status (n = 6, 11.8%; P = .028) (Table 1).
Table 1: Characteristics of the Study Cohort
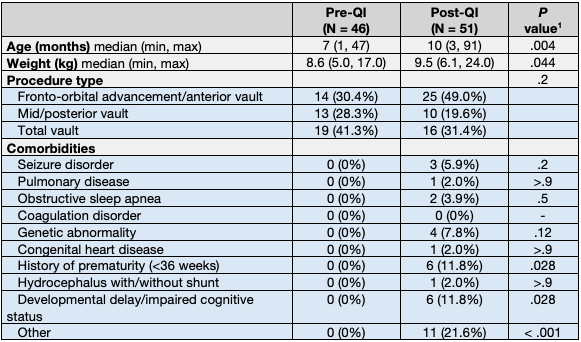
1Wilcoxon rank sum test; Pearson chi-squared test; Fisher exact test. QI, quality improvement.
Pre-QI, no patients were given preoperative iron supplementation (n = 0); post-QI, there was a significant increase in the number of patients who received the supplementation (n = 8, 15.7%; P = .006). Intraoperatively, there was a significant increase in the number of patients who received TXA from 0% to 94.1% (n = 48, P < .001) and in the number of cases in which a cell saver was used from 4.3% (n = 2) to 62.7% (n = 32; P < .001) (Table 2). The cell saver was used in all post-QI cases in which it was available; however, there were instances when a cell saver was not available, which limited its post-QI use to 62.7% (n = 32).
Table 2: Blood Transfusion- and Hospital Stay-Related Factors, Before and After the Initiative
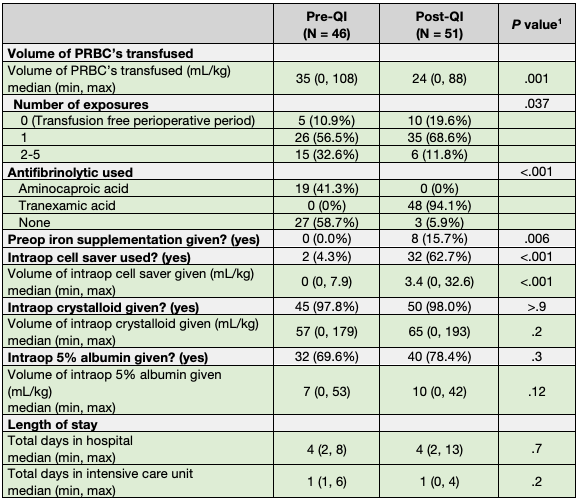
1Wilcoxon rank sum test; Pearson chi-squared test; Fisher exact test. PRBC, packed red blood cells; QI, quality improvement
There was a significant decrease in the number of blood donor exposures during the perioperative period (P = .037) after the initiative was implemented (Table 2, Figure 1). The number of patients who experienced a transfusion-free perioperative period increased from 10.9% (n = 5) to 19.6% (n = 10). Additionally, patients treated post-QI had a significantly lower median volume of packed red blood cells (PRBC) transfused during the perioperative course (35 vs 24 mL/kg, P = .001). The volume of crystalloids transfused intraoperatively increased from 57 to 65 mL/kg (P = .2). Likewise, the volume of 5% albumin transfused intraoperatively increased from 7 to 10 mL/kg, but there was no significant difference in either (Table 2).
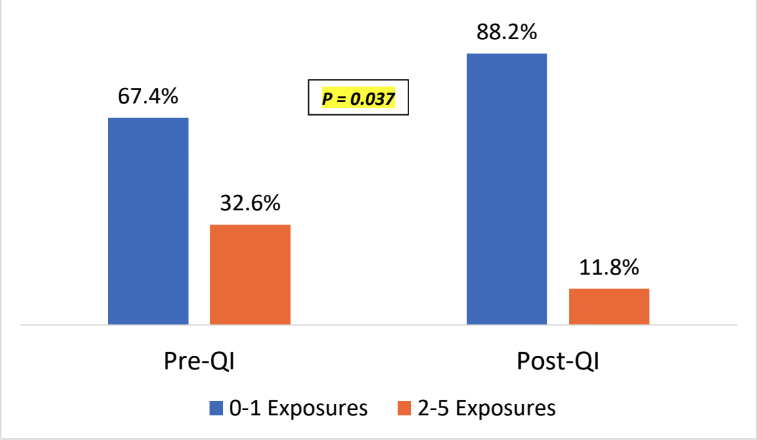
Figure 1: Number of blood donor exposures before and after the implementation of the QI initiative
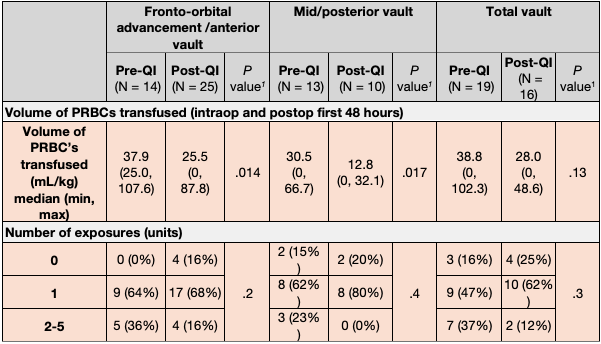
A subgroup analysis was done for each type of procedure. Post-QI, there was a significant decrease in the volumes of PRBCs transfused for both fronto-orbital advancements (37.9 to 25.5 mL/kg, P = .014) and mid/posterior vault reconstructions (30.5 to 12.8 mL/kg, P = .017) (Figure 2). The volume of PRBCs transfused for total vault reconstructions also decreased (38.8 to 28.0 mL/kg, P = .13), but there was not a statistically significant difference. Likewise, there was no difference in the number of exposures within each type of procedure (Table 3).
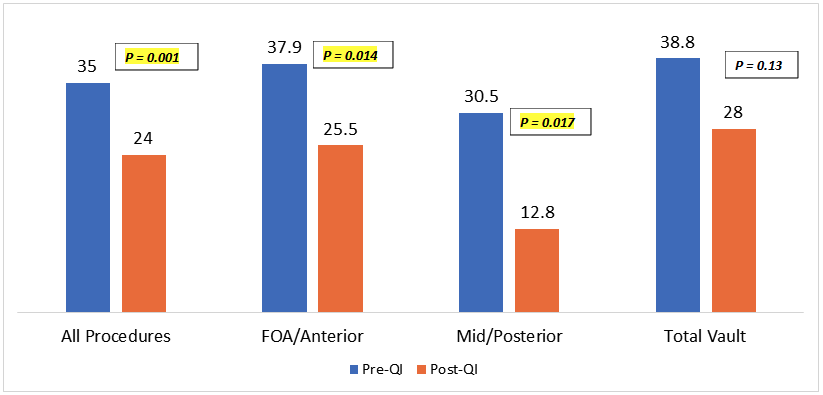
Figure 2: Volume of blood transfused (mL/kg) before and after the implementation of the QI Initiative (intraoperatively and in the first 48-hours postoperatively).
Table 3: Blood Transfusion Volume and Number of Exposures Based on Type of Operation
1Wilcoxon rank sum test; Fisher exact test. PRBC = packed red blood cells; QI, quality improvement.
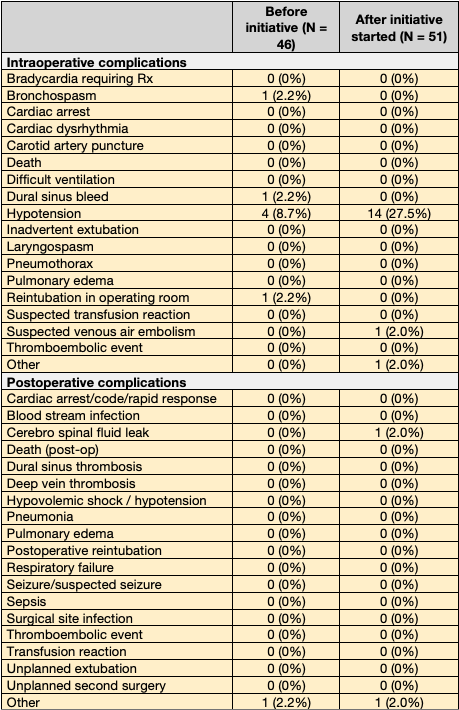
There was no difference in the median length of stay in the intensive care unit (ICU) (1 vs 1 day, P = .2) nor in the hospital (4 vs 4 days, P = .7) (Table 2). Overall, pre- and post-QI, there were low numbers of intra and postoperative complications (Table 4). Of note, there was a significant increase in the number of patients who experienced intraoperative hypotension pre-QI (n = 4, 8.7%) compared with post-QI vs (n = 14, 27.5%; P = .03), but there was no increase in intraoperative mortality (0% vs 0%) nor in intraoperative cardiovascular complications such as bradycardia (0% vs 0%), cardiac arrest (0% vs 0%), or cardiac dysrhythmia (0% vs 0%).
Table 4: Intraoperative and Postoperative Complications
The total perioperative blood transfusion volume decreased from 35 to 24 mL/kg, and the rate of transfusion-free perioperative periods increased from 10.9% to 19.6%, with an overall decrease in the number of exposures (Table 2). The cumulative effect of combining these techniques lies in their ability to offset the individual limitations of each strategy when used in isolation. For instance, while preoperative iron supplementation can optimize hemoglobin levels, it may not prevent intraoperative blood loss on its own. Similarly, intraoperative strategies such as the use of TXA or cell savers are most effective when paired with transfusion guidelines that prevent unnecessary transfusions. Our data demonstrate that implementing this multimodal approach was effective and safe at our institution. Further research is needed to determine its applicability and effectiveness at other institutions.
Discussion
This QI initiative included a combination of methods to decrease the need for allogeneic blood transfusion for patients undergoing OCCVR. This included the use of preoperative oral iron supplementation, intraoperative cell saver and TXA, and allogenic PRBC transfusion guidelines. The initiative has successfully resulted in a significant decrease in both the volume of allogenic PRBCs transfused and the blood donor exposures, without an increase in severe perioperative complications. The total perioperative blood volume decreased from 35 to 24 mL/kg, and the rate of transfusion-free perioperative periods increased from 10.9% to 19.6%, with an overall decrease in the number of exposures (Table 2). The cumulative effect of combining these techniques lies in their ability to offset the individual limitations of each strategy when used in isolation. For instance, while preoperative iron supplementation can optimize hemoglobin levels, it may not prevent intraoperative blood loss on its own. Similarly, intraoperative strategies such as the use of TXA or cell savers are most effective when paired with transfusion guidelines that prevent unnecessary transfusions. Our data demonstrate that this initiative was effective and safe at our institution. Further research is needed to determine its applicability and effectiveness at other institutions.
TXA has been proven to significantly decrease the volume of perioperative blood transfusions, but its utilization has been met with caution due to reports of thromboembolic events and seizures.6,12 Goobie et al6 found that only 59.5% of CCVR cases nationally used antifibrinolytics, with concerns for side effects being a major determinant. Their study also revealed no significant increase in the incidence of thromboembolic events or seizures in infants treated with TXA. Our study additionally found no incidences of thromboembolic events or seizures (Table 4). TXA is readily available, and Dadure et al2 showed that the use of TXA decreased the median cost of treating blood loss compared with the use of PRBCs ($0.70 vs $240). These findings suggest that TXA is a viable and safe option.
Cell saver allows for an autologous transfusion of the patient’s own blood that was lost during surgery, thereby removing the immunological risks of allogeneic blood. Its use was previously limited to adults because the collection bowls were too large for the proportionately small volumes lost from infants, but it is now a viable option since the introduction of devices with smaller bowls.16,17 In our study, only 62.7% (n = 32) of cases used cell savers (Table 2). Although this was a significant increase from 4.3% (n = 2), the overall utilization was low when compared with other techniques such as TXA (94.1%, n = 48). The Pediatric Craniofacial Collaborative Group analyzed perioperative management, outcomes and complications in 1223 children undergoing complex cranial vault reconstruction across 31 institutions in North America, using data from 2012 to 2015.3 Nationally, cell saver was used in only 14% of cases.3 Lower utilization can be attributed to the need for additional experienced personnel and machinery as well as technical limitations.1,3,12 When using the cell saver, attention is needed to prevent contamination with betadine, hydrogen peroxide, or fibrin glue, which can lead to severe morbidity.8 In cases where blood is salvaged inefficiently, there may be no blood to transfuse after processing.16 Caution is necessary when transfusing blood from the cell saver because it contains no other blood components, which increases the risk of dilutional coagulopathy and continued blood loss.8 Lastly, pediatric patients tend to increase vascular tone to compensate for volume loss, but can decompensate quickly during a processing delay when transfusion is needed.8 These factors emphasize the need for experienced personnel. The need for additional personnel and the cost of the machinery make the use of cell savers financially inviable for some institutions. In addition to the capital cost of the machine, the cost per case is estimated to be $250.16 Nevertheless, our study and others have shown that cell savers decrease the need for allogenic transfusions.16,17 As pediatric collection bowls become more widely available and providers become more comfortable using the cell saver, its popularity is expected to increase.
Restrictive transfusion protocols are safe and effective and should be the cornerstone of any initiative to reduce the rate of transfusions.1,19-21 Despite this, formal transfusion protocols are not used in approximately two-thirds of OCCVR cases nationally.3 Transfusion protocols require a significant commitment from the entire management team, as clinicians may reflexively and excessively transfuse without clinical indications.4,12,19 Studies have shown that infants can tolerate and maintain tissue oxygenation at lower hemoglobin levels than previously thought20,21 and have also established evidence-based transfusion triggers that can be implemented.22 Of note, our study found a significant increase in the incidence of intraoperative hypotension (Table 4). In our study, hypotension was defined as a drop in blood pressure that required administration of a vasopressor. Upon initial assessment, it could be deduced that the use of restrictive transfusion protocols led to the increase in intraoperative hypotension. As previously mentioned, an infant’s cardiovascular system is tenuous and is at risk of decompensation from even mild blood loss.8 Despite this increase in hypotension, there was no increase in other cardiovascular complications such as bradycardia, cardiac arrest, cardiac dysrhythmia, or mortality, nor in postoperative hypotension (Table 4). We can then hypothesize that the hypotensive episodes were likely transient and could be related to normal intraoperative events, and, thus, did not have an impact on overall morbidity. Additionally, these episodes of hypotension could have been opportunities for unnecessary blood transfusion. To compensate for this, we saw a significant increase in the volume of crystalloids transfused (Table 2). Larger scale studies would need to be performed to identify acceptable levels of hypotension in this patient cohort.3
There are numerous other methods to reduce perioperative transfusion. Preoperative erythropoietin (EPO) is often mentioned and is found to reduce the need for transfusions in pediatric craniofacial surgeries .7,16,20,23 Currently, EPO is approved by the FDA to reduce the need for allogenic blood transfusions in adult surgical patients, but it is not explicitly approved for the same indication in pediatric patients.12 Additionally, EPO has been associated with hypertension, thrombocytosis, thrombosis, renal failure, stroke, and death, and has consequently been given a black box warning by the FDA.1,20 Using EPO often requires multiple preoperative visits for subcutaneous administration, as well as follow-up hemoglobin surveillance, which makes it a lengthy and costly process for patients and clinicians.1,7,12,16 These concerns limit its popularity,1 with only 0.2% of cases using it nationally3; therefore, it was not used in this initiative.
Various anesthetic techniques have also been employed, one of which is acute preoperative normovolemic hemodilution, which involves exchanging whole blood for colloid/crystalloid and then reinfusing the blood at the end of the procedure.8,20 This technique is usually performed in tandem with other methods and has been shown to reduce the need for allogenic transfusions.8,20 However, there has been limited benefit reported from this technique,1,2 and it therefore has been virtually abandoned in CCVR.3 Another older technique is hypotensive anesthesia/deliberate hypotension, which involves iatrogenically lowering blood pressure to theoretically decrease blood loss.8 Safe limits for hypotension in children are yet unknown,3 and this technique cannot be used in patients with hypovolemia or elevated intracranial pressure. Similarly, there is a lack of evidence to support its efficacy; even so, this technique was used in 4% of cases.3
Other institutions have introduced initiatives to reduce blood transfusions during OCCVR and have found similar results to our study.4,8,9,11,12,16,20 Additionally, most initiatives found limited mortality and morbidity from their interventions. Vega et al20 initiated a protocol that involved the use of preoperative EPO and iron therapy, cell saver, and a transfusion guideline for a hemoglobin level of less than 7 g/dL. They found a significant decrease in the rate but not the volume of transfusion. Notably, the rate of transfusions decreased with time, which was thought to reflect a delay in the adoption of the protocol. Nguyen et al9 implemented a protocol that consisted of using transfusion algorithms alongside blood-sparing surgical techniques, and they found a significant decrease in transfusion rates and volumes. Velardi et al8 used a protocol that involved EPO, preoperative autologous blood donation, preoperative normovolemic hemodilution, and cell saver. They tested their protocol on 13 consecutive patients and were able to avoid allogeneic blood transfusion in 11 of them. Krajewski et al16 studied the use of preoperative iron, EPO, and intraoperative cell saver and found significantly lower transfusion rates and volumes. They commented that only 80% of their study patients received cell saver blood due to low blood volumes salvaged but stated that, of those, 31% would have needed transfusion if the cell saver blood was not available. Two studies implemented interventions sequentially to see the individual effect of each parameter. Muhly et al4 initially implemented a protocol of transfusing reconstituted blood instead of PRBCs alone; they then sequentially implemented postoperative transfusion guidelines and intraoperative antifibrinolytics, and finally used fresh whole blood instead of reconstituted blood. The use of reconstituted blood and whole blood was used to replenish loss coagulation factors in an attempt to reduce blood loss. They found that each group was able to have sustained reduction in exposures, but only the addition of whole blood was able to produce a significant reduction in volume of blood lost. Kurlander et al12 initially implemented aminocaproic acid (ACA) and then implemented a protocol of EPO, ACA, and perioperative resuscitation and transfusion thresholds. In both instances, they were able to significantly decrease transfusion volumes but were not able to identify a significant difference between the interventions. This group also aimed to use cell saver but was limited by a lack of compliance.
Limitations
Our study was not without limitations. Ensuring each aspect of the protocol was implemented was difficult. Preoperative outpatient interventions, such as iron supplementation, are unpredictable due to varying patient compliance. Additionally, specific aspects of the protocol were more applicable to some patients than others based on the clinical scenario. As seen in our study and others,12,16 using the cell saver may not be applicable in all patients; therefore, the net benefit from this intervention may be limited. Only 94.1% (n = 48) of our patients received TXA, 15.7% (n = 8) received iron, and 62.7% (n = 32) received cell saver, which shows a lack of homogeneity in intervention utilization and would therefore underrepresent the potential of the protocol. Additionally, since our study did not test for each intervention in isolation, no comment can be made on the individual benefit of each. Our study did not test for perioperative hemoglobin levels or perform intraoperative tests of coagulation parameters and fibrinogen and platelet levels. This approach has been used by other teams9,12,19 and allows for a tailored approach to resuscitation instead of reflexive PRBC transfusion.
Lastly, the heterogeneity of patients, pathologies, and management practices among both surgeons and anesthesiologists within every institution would naturally result in varying levels of blood loss and would confound the results. Therefore, the patient, anesthesiologist, and surgeon may be important causal variables in the decision to transfuse.8 Nguyen et al9 attempted to control for this with standardized surgical techniques, but total standardization in management practices is not possible. Despite this natural variability in patient management and being unable to enforce the protocol in all patients, we were still able to witness a reduction in blood transfusion volumes and exposures.
Currently, there is not enough evidence to identify which method or combination of methods are most effective. We have successfully identified that implementation of a combination of parameters can reduce PRBC transfusion requirements at our institution without an increase in morbidity, and the next step is to perform multi-institutional randomized prospective studies in order to justify large-scale implementation of national standards. Increased standardization of the parameters and management of the practices would be needed to provide stronger evidence of the efficacy of this initiative. Additionally, multidisciplinary input in the creation and implementation of protocols would improve management outcomes and increase compliance with protocols.12 Importantly, a cost-benefit analysis is needed to evaluate both the financial costs and the practicability of implementing such initiatives in other settings. The costs of additional lab work, medication, personnel, and risks of cardiovascular decompensation need to be weighed against the costs, scarcity, and morbidity of blood products. As mentioned, appropriate resources may not be available and multiple visits for preoperative treatment may not be practical for some patients. A one-size-fits-all approach may not be appropriate for each patient or institution and a more tailored approach with evidence-based practice methods should be used.
Conclusions
The JHACH perioperative blood transfusion QI initiative for patients undergoing OCCVR has resulted in reduced blood transfusion volumes and reduced blood donor exposures without an increase in perioperative complications related to blood loss. This was achieved through preoperative iron supplementation, the intraoperative use of a cell saver and TXA, and the use of intraoperative transfusion guidelines. Further multi-institutional research is necessary to create national standards for the anesthetic care of all patients undergoing OCCVR.
Acknowledgments
Authors: Joshua M. Wright, MBBS1; Molly F. MacIsaac, BS1; S. Alex Rottgers, MD1; Alexandra Miller, MPH, CPH2; Jamie Fierstein, PhD2; Lillian Zamora, MD3; Allison Fernandez, MD, MBA3
Affiliations: 1Division of Plastic and Reconstructive Surgery, Department of Surgery, Johns Hopkins All Children’s Hospital; St. Petersburg, Florida; 2Epidemiology and Biostatistics Shared Resource, Institute for Clinical and Translational Research, Johns Hopkins All Children’s Hospital, St Petersburg, Florida; 3Department of Anesthesiology and Pain Medicine, Johns Hopkins All Children’s Hospital; St. Petersburg, Florida
The authors acknowledge Dominique Tran, Dr. Cassandra Josephson, and The Pediatric Craniofacial Collaborative Group.
Correspondence: Allison Fernandez, MD, MBA; aferna27@jhmi.edu
Ethics: IRB00079926: Pediatric Craniofacial Surgery Perioperative Registry (PCSPR)
Disclosures: The authors disclose no financial or other conflicts of interest.
References
1. Stricker PA, Fiadjoe JE. Anesthesia for craniofacial surgery in infancy. Anesthesiol Clin. 2014;32(1):215-235. doi: 10.1016/j.anclin.2013.10.007
2. Dadure C, Sauter M, Bringuier S, et al. Intraoperative tranexamic acid reduces blood transfusion in children undergoing craniosynostosis surgery: a randomized double-blind study. Anesthesiology. 2011;114(4):856-861. doi: 10.1097/ALN.0b013e318210f9e3
3. Stricker PA, Goobie SM, Cladis FP, et al; Pediatric Craniofacial Collaborative Group. Perioperative outcomes and management in pediatric complex cranial vault reconstruction: a multicenter study from the Pediatric Craniofacial Collaborative Group. Anesthesiology. 2017;126(2):276-287. doi: 10.1097/ALN.0000000000001481
4. Muhly WT, Tan JM, Hsu G, et al. Care standardization reduces blood donor exposures and transfusion in complex cranial vault reconstruction. Hosp Pediatr. 2018;8(10):595-603. doi: 10.1542/hpeds.2018-0027
5. Goobie SM, Zurakowski D, Isaac KV, et al; Pediatric Craniofacial Collaborative Group. Predictors of perioperative complications in paediatric cranial vault reconstruction surgery: a multicentre observational study from the Pediatric Craniofacial Collaborative Group. Br J Anaesth. 2019;122(2):215-223. doi: 10.1016/j.bja.2018.10.061
6. Goobie SM, Cladis FP, Glover CD, et al; Pediatric Craniofacial Collaborative Group. Safety of antifibrinolytics in cranial vault reconstructive surgery: a report from the pediatric craniofacial collaborative group. Paediatr Anaesth. 2017;27(3):271-281. doi: 10.1111/pan.13076
7. Helfaer MA, Carson BS, James CS, Gates J, Della-Lana D, Vander Kolk C. Increased hematocrit and decreased transfusion requirements in children given erythropoietin before undergoing craniofacial surgery. J Neurosurg. 1998;88(4):704-708. doi: 10.3171/jns.1998.88.4.0704
8. Velardi F, Di Chirico A, Di Rocco C, et al. "No allogeneic blood transfusion" protocol for the surgical correction of craniosynostoses. I. Rationale. Childs Nerv Syst. 1998;14(12):722-731; discussion 740-741. doi: 10.1007/s003810050305
9. Nguyen TT, Hill S, Austin TM, Whitney GM, Wellons JC III, Lam HV. Use of blood-sparing surgical techniques and transfusion algorithms: association with decreased blood administration in children undergoing primary open craniosynostosis repair. J Neurosurg Pediatr. 2015;16(5):556-563. doi: 10.3171/2015.3.PEDS14663
10. Lavoie J. Blood transfusion risks and alternative strategies in pediatric patients. Paediatr Anaesth. 2011;21(1):14-24. doi: 10.1111/j.1460-9592.2010.03470.x
11. White N, Bayliss S, Moore D. Systematic review of interventions for minimizing perioperative blood transfusion for surgery for craniosynostosis. J Craniofac Surg. 2015;26(1):26-36. doi: 10.1097/SCS.0000000000001108
12. Kurlander DE, Ascha M, Marshall DC, et al. Impact of multidisciplinary engagement in a quality improvement blood conservation protocol for craniosynostosis. J Neurosurg Pediatr. 2020;26(4):406-414. doi: 10.3171/2020.4.PEDS19633
13. Jalali A, Lonsdale H, Zamora LV, et al; Pediatric Craniofacial Collaborative Group. Machine learning applied to registry data: development of a patient-specific prediction model for blood transfusion requirements during craniofacial surgery using the Pediatric Craniofacial Perioperative Registry dataset. Anesth Analg. 2021;132(1):160-171. doi: 10.1213/ANE.0000000000004988
14. Goobie SM, Meier PM, Pereira LM, et al. Efficacy of tranexamic acid in pediatric craniosynostosis surgery: a double-blind, placebo-controlled trial. Anesthesiology. 2011;114(4):862-871. doi: 10.1097/ALN.0b013e318210fd8f
15. Lu VM, Goyal A, Daniels DJ. Tranexamic acid decreases blood transfusion burden in open craniosynostosis surgery without operative compromise. J Craniofac Surg. 2019;30(1):120-126. doi: 10.1097/SCS.0000000000004875
16. Krajewski K, Ashley RK, Pung N, et al. Successful blood conservation during craniosynostotic correction with dual therapy using procrit and cell saver. J Craniofac Surg. 2008;19(1):101-105. doi: 10.1097/scs.0b013e3180f6112f
17. Dahmani S, Orliaguet GA, Meyer PG, Blanot S, Renier D, Carli PA. Perioperative blood salvage during surgical correction of craniosynostosis in infants. Br J Anaesth. 2000;85(4):550-555. doi: 10.1093/bja/85.4.550
18. Moradi Farsani D, Mazaheri Z, Shafa A. The effect of tranexamic acid and controlled hypotension on perioperative blood loss in craniosynostosis surgery. Anesth Pain Med. 2023;13(1):e130462. doi: 10.5812/aapm-130462
19. Stricker PA, Fiadjoe JE, Kilbaugh TJ, et al. Effect of transfusion guidelines on postoperative transfusion in children undergoing craniofacial reconstruction surgery. Pediatr Crit Care Med. 2012;13(6):e357-e362. doi: 10.1097/PCC.0b013e31825b561b
20. Vega RA, Lyon C, Kierce JF, Tye GW, Ritter AM, Rhodes JL. Minimizing transfusion requirements for children undergoing craniosynostosis repair: the CHoR protocol. J Neurosurg Pediatr. 2014;14(2):190-195. doi: 10.3171/2014.4.PEDS13449
21. Rouette J, Trottier H, Ducruet T, Beaunoyer M, Lacroix J, Tucci M; Canadian Critical Care Trials Group; PALISI Network. Red blood cell transfusion threshold in postsurgical pediatric intensive care patients: a randomized clinical trial. Ann Surg. 2010;251(3):421-427. doi: 10.1097/SLA.0b013e3181c5dc2e
22. Morley SL. Red blood cell transfusions in acute paediatrics. Arch Dis Child Educ Pract Ed. 2009;94(3):65-73. doi: 10.1136/adc.2007.135731
23. Fearon JA, Weinthal J. The use of recombinant erythropoietin in the reduction of blood transfusion rates in craniosynostosis repair in infants and children. Plast Reconstr Surg. 2002;109(7):2190-2196. doi: 10.1097/00006534-200206000-00002