Use of a Novel Adhesive Suture Retention Device in Non-traumatic Diabetic Lower Extremity Amputations: A Multicenter Case Review
© 2023 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Background. Amputations in the diabetic foot are commonly associated with complications, including delayed wound healing, surgical site dehiscence, and the need for additional amputations. Use of a novel adhesive suture retention device (ASRD) has been previously shown to support improved linear closure outcomes. The purpose of this retrospective case review was to determine if the adoption of the ASRD in 5 podiatric surgical practices would reduce postoperative complications in patients with diabetes undergoing foot amputations including surgical site dehiscence and the need for additional amputation.
Methods. A 5-center retrospective chart review was performed to assess the difference in postoperative surgical site dehiscence and reamputation rates for patients with diabetes undergoing minor and major lower extremity amputations before and after adopting the use of the ARSD.
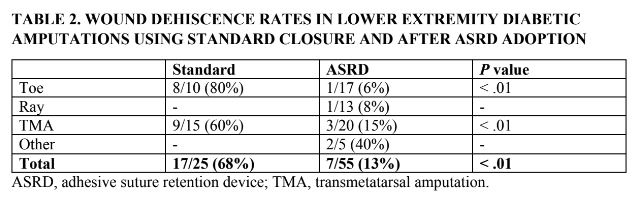
Results. Adoption of the adhesive retention suture device was associated with an overall decrease in wound dehiscence of 81% (P < .01). Additionally, there was an 89% reduction in progression to higher level amputation in the ARSD cohort (P = .015).
Conclusions. Utilization of the ARSD decreased the incidence of postoperative wound dehiscence and reamputation in this patient cohort, thus lessening patient morbidity and decreasing the overall cost of care.
Introduction
The prevalence of diabetic foot–related complications is on the rise worldwide. Diabetes has emerged as one of the most serious and common chronic diseases of our times, causing life-threatening, disabling, and costly complications and reducing life expectancy.1 The global diabetes prevalence in 20- to 79-year-olds in 2021 was estimated to be 10.5% (536.6 million people) and expected to rise to 12.2% (783.2 million) in 2045.1
Complications of diabetic foot disease are the main contributors to lower extremity amputations (LEAs). Published crude estimates show that up to 75% of LEAs are being performed on patients with diabetes.2,3 The development of an infected diabetic foot ulcer leads to amputation in 10% to 30% of cases.4 Additionally, nontraumatic LEAs in patients with diabetes are complicated by wound dehiscence in up to 80% of cases.5
Successful management of diabetic foot disease is complex and remains a challenge for both patients and clinicians alike. Reducing morbidity and mortality and improving quality of life for persons with diabetic foot disease is a critical public health objective. The purpose of this study is to determine if a reduction in incidence of postamputation complications, mainly surgical site dehiscence and regression to higher amputation, would be appreciated after the adoption of a new suture retention device.

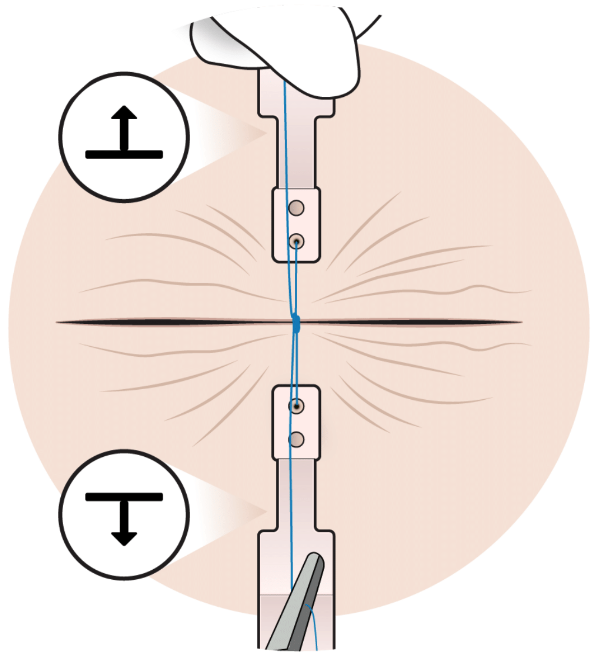
A novel adhesive suture retention device (ASRD) (HEMIGARD ARS device; SUTUREGARD Medical, Inc) has been shown to reduce fragile skin tearing, improve wound edge perfusion, and reduce lower extremity excisional wound dehiscence when compared with standard layered closures (Figure 1).6,7 When properly applied (Figure 2), the ASRD strips prevent skin tearing and improve perfusion compared with sutures alone to aid in the reduction of lower extremity wound dehiscence.6,7
Materials and Methods
This study was designed as a 5-center, retrospective analysis of patient outcomes before and after adopting the ASRD device. A retrospective chart review was performed to identify patients with diabetes who had undergone a nontraumatic foot amputation for a period of 6 months before and after the adoption of the ASRD in these 5 clinical sites. Demographic and site-specific details were recorded without any identifying patient data. The method of closure, the rate of surgical site dehiscence, and the incidence of regression to additional amputation were documented. As per historic literature, wound dehiscence was defined as exposed dermal or deeper tissue in at least 20% of the length of the wound closure.8
All wounds that underwent standard linear closure before ASRD adoption were closed with buried dermal absorbable sutures and percutaneous nonabsorbable sutures. All wounds that underwent linear closure during the period after ASRD adoption were reapproximated according to the ASRD instructions for use. Each ASRD pouch contained 2 adhesive, sterile, single-use disposable strips, each measuring 6 cm × 1.6 cm. As per product instructions, 1 strip was placed perpendicular to the wound edges on each side of a wound so that their leading holes were 10 mm from the wound edges. The ASRD was applied to clean, dry skin with minimal hair before proceeding to the next step. After adhering the ASRD strips, a nylon suture (usually 2-0 or 3-0) was sutured through the holes of the ASRD strips to close the wound. The surgical incision was then covered with a primary nonadherent dressing and secondarily with multiple layers of dry, sterile bandages.
Statistical Methods
The statistical significance between the cohorts in categorical variables was tested using the chi-square test and in continuous variables using t tests. All tests were 2-tailed with a significance level of P < .05.
Results
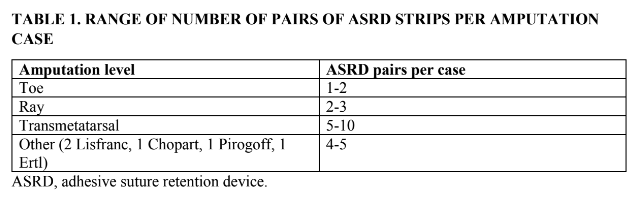
There were 25 patients identified in the pre-ASRD cohort and 55 patients in the post-ASRD cohort. There were no significant differences in baseline patient age or sex. The range of number of ASRD pairs used per case is outlined in Table 1.
An overall decrease in wound dehiscence of 81% (P < .01) was noted in the ASRD cohort (Table 2). Of the 25 patients who had their amputations performed without ASRD, 4 (16%) went on to have complications requiring a higher-level amputation (2 above the knee and 2 below the knee). Of the 55 patients who had their amputations performed with ASRD and minimal or no dermal absorbable sutures, only 1 patient (1.8%) went on to require a higher-level amputation (1 below the knee). This represents an 89% reduction in progression to higher-level amputation (P = .015). No skin tears or other dermal adverse effects were noted in this patient cohort.
Discussion
The data show that the use of the ASRD was effective in decreasing surgical site dehiscence in patients with diabetes who underwent foot amputations. Surgical wound dehiscence is defined as the separation of the margins of a closed surgical incision that has been made in skin, with or without exposure or protrusion of underlying tissue, organs, or implants.9 Chronic disease states, such as diabetes, can increase a patient’s risk for developing postoperative dehiscence.10 Results of this study demonstrated favorable clinical outcomes in a patient population in which surgical sites have a historically high incidence of postoperative complications. ASRD-treated patients in this retrospective case review showed statistically significantly faster wound healing and a lower frequency of surgical site dehiscence.
There has been considerable interest in the literature in determining markers that are associated with successful operative outcomes in patients with diabetic foot disease. Despite increases in knowledge relative to the process of wound healing, postamputation surgical site dehiscence is still a major contributing factor to increased hospital stays, prolonged healing, and reoperation rates in patients with diabetes.
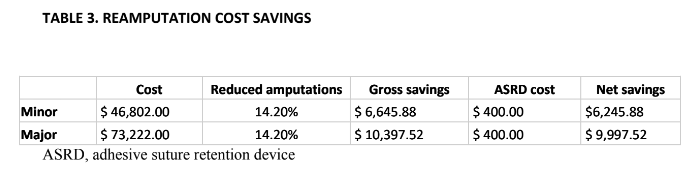
Reducing lower-extremity amputation rates is one of the main objectives for clinicians providing diabetic foot care. In a review article examining the price tag associated with amputations in persons with diabetes, the reported cost of a lower limb amputation ranged from $10,103 to $67,773.11 The mean cost estimate was further segmented into minor amputations ($46,802) and major amputations ($73,222).11 A significant decline in reamputation rates was noted in the ASRD-treated group (1.8%) versus the non–ASRD-treated group (16%). Using the cost data reported in the Nilsson study and segmenting based on the amputation level, the incorporation of the ASRD into the surgical algorithm generated significant overall cost-savings (Table 3).
Patients undergoing a lower-limb amputation have a high risk of death, with perioperative mortality rates ranging from 9% to 16% within the first postoperative year.12 Optimizing patient rehabilitation and function can influence short- and long-term patient survival. Implementing perioperative protocols that include early patient mobilization are shown to produce better patient outcomes.13 Ambulatory status decreases following high-level lower-extremity amputations. Altered biomechanics increase demand for energy, oxygen, and cardiac function.14 Physiologic and psychosomatic factors, including pain, instability, or psychological stress, contribute to the lack of physical activity seen in patients who have undergone amputation.14 Additionally, increased demand on the contralateral limb amplifies the risk of contralateral amputation.14
The incorporation of the ASRD tool improved surgical incision heal rates and decreased surgical site dehiscence rates but also helped to support more distal limb amputations, resulting in better patient postoperative function. Surgeons should choose surgical interventions that salvage as much of the native foot as possible. This cohort study illustrates that augmenting primary closure with ASRD results in a more stable soft tissue envelope. Performing distal foot amputations offers patients the chance for unassisted ambulation on an end-bearing limb, with decreased energy expenditure compared with more proximal amputations. Maintaining quality of life and patient mobility is the hallmark of successful diabetic limb salvage surgery.
Limitations
There are limitations of this study that should be noted. The retrospective design of this study may serve as a limitation. Further prospective evaluations with randomization of the 2 patient groups would be required to definitively establish a relationship between the use of the ASRD and the decrease in postoperative dehiscence and reamputation. This study evaluated a limited number of patients from 5 clinical practices. Randomized studies with larger patient sample sizes are needed to solidify conclusions more robustly, although this study can act as a pilot for further investigation.
Conclusions
In conclusion, to the authors’ knowledge, this is the only patient cohort study that compared an ASRD closure device to standard of care linear incision closure in amputations in the diabetic foot. By curtailing surgical site dehiscence following amputation, the ASRD can potentially decrease the need for higher-level amputations, improve patient function, lessen morbidity, and decrease the overall cost of care in this at-risk patient population.
Acknowledgments
Affiliations: 1Kent State University College of Podiatric Medicine, Kent, Ohio; 2Advanced Orthopedics, Avon, Connecticut; 3Agility Orthopedics, Stoneham, Massachusetts; 4Ocean State Foot and Ankle Specialists, Woonsocket, Rhode Island; 5Northwest University Feinberg School of Medicine, Chicago, Illinois; 6Itasca Foot and Ankle, Itasca, Illinois
Correspondence: Windy Cole, DPM; wcole4@kent.edu
Disclosures: Authors WC and EH are medical advisors for Suturegard. The authors declare no other conflicts of interest or financial disclosures.
References
1. Sun H, Saeedi P, Karuranga S, Pinkepank M, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
2. Trautner C, Haastert B, Spraul M, Giani G, Berger M. Unchanged incidence of lower-limb amputations in a German City, 1990–1998. Diabetes Care. 2001;24(5):855-859. doi:10.2337/diacare.24.5.855
3. Almaraz MC, Gonzalez-Romero S, Bravo M, et al. Incidence of lower limb amputations in individuals with and without diabetes mellitus in Andalusia (Spain) from 1998 to 2006. Diabetes Res Clin Pract. 2012; 95(3):399-405. doi:10.1016/j.diabres.2011.10.035
4. Berendt AR, Peters EJ, Bakker K, et al. Diabetic foot osteomyelitis: a progress report on diagnosis and a systematic review of treatment. Diabetes Metab Res Rev. 2008 May-Jun;24 Suppl 1:S145-S161. doi:10.1002/dmrr.836
5. Vassalo IM, Gatt A, Cassar K, Papanas N, Formosa C. Healing and mortality rates following toe amputation in type II diabetes mellitus. Exp Clin Endocrinol Diabetes. 2021;129(6):438-442. doi:10.1055/a-0942-1789
6. Stoecker A, Lear W, Johnson K, Bahm J, Kruzic JJ. Enhanced perfusion of elliptical wound closures using a novel adhesive suture retention device. Health Sci Rep. 2021;4(3):e364. doi:10.1002/hsr2.364
7. Cole W, Fancher W, Stoecker A, Howerter S, Lear W. Use of a novel adhesive suture retention device in lower leg excisional closure: a retrospective review. Wounds. 2021;33(9):222-225.
8. Oganesyan G, Jarell AD, Srivastava M, Jiang SIB. Efficacy and complication rates of full-thickness skin graft repair of lower extremity wounds after Mohs micrographic surgery. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. 2013;39(9):1334-1339. doi:10.1111/dsu.12254
9. Dowsett C, Ferreira F, Ousey K, et al. World Union of Wound Healing Societies consensus document. Surgical wound dehiscence: improving prevention and outcomes. Wounds International. February 20, 2018. Accessed August 14, 2023. https://woundsinternational.com/wp-content/uploads/sites/8/2023/02/3bc56168ce170d2745c58ebf922a75e1.pdf
10. Chun JC, Yoon SM, Song WJ, Jeong HG, Choi CY, Wee SY. Causes of surgical wound dehiscence: a multicenter study. J Wound Manag Res. 2018;14(2):74-79. doi:10.22467/jwmr.2018.00374
11. Nilsson A, Willis M, Neslusan C. A review of the costs of lower limb amputations in patients with diabetes in the US. Value in Health. 2018 May;21(Suppl 1):S73. doi:10.1016/j.jval.2018.04.492
12. Lim TS, Finlayson A, Thorpe JM, et al. Outcomes of a contemporary amputation series. ANZ J Surg. 2006 May;76(5):300-305. doi:10.1111/j.1445-2197.2006.03715
13. Kehlet H, Wilmore DW. Evidence-based surgical care and the evolution of fast-track surgery. Ann Surg. 2008 Aug;248(2):189-198. doi:10.1097/SLA.0b013e31817f2c1a
14. Ward KH, Meyers MC. Exercise performance of lower-extremity amputees. Sports Med. 1995;20:207-214. doi:10.2165/00007256-199520040-00001