Augmenting the Breast Reconstruction: Core Projection With Hybrid Microsurgical Breast Reconstruction With Flap and Stacked Prepectoral Acellular Dermal Matrix
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Background. Many patients who require breast reconstruction prefer a flap-based approach for various reasons, including the permanence and aesthetic benefit of a breast that looks and feels natural. For patients who desire autologous breast reconstruction following mastectomy but lack adequate donor site volume, the authors utilize the novel hybrid flap, prepectoral acellular dermal matrix (HyPAD) approach. In this technique, the deep inferior epigastric perforator (DIEP) flap is augmented with a stacked acellular dermal matrix (ADM). The purpose of this study is to quantify the soft tissue augmentation and core projection achieved with this technique during autologous flap-based breast reconstruction.
Methods. Consecutive patients who underwent the HyPAD technique during the study period (August 2021 to December 2022) were identified. All patients lacked adequate donor site volume and wished to avoid the placement of implants during their reconstruction. Demographic information and outcomes were assessed. Intraoperatively, the weights (g) of the mastectomy specimen, the flap donor site, and the stacked ADM were recorded.
Results. During the study period, 21 patients (n = 21) were identified. The mean age of patients at the time of surgery was 48.9 ± 7.85 years. The mean body mass index was 24.1 kg/m2 ± 3.3 kg/m2. The mean mastectomy specimen weight was 436.35 g, and the mean flap weight was 370.73 g, posing an average discrepancy of 15.04% or 65.62 g. The average weight of the ADM used to augment the flap was 81.76 g. This weight accounted for an average of 18.07% of the total reconstructed breast weight.
Conclusions. The use of ADM during autologous breast reconstruction provides patients with an alternative to implants that allows them to obtain their desired breast volume. Given the aesthetic impact that ADM has on the total amount of flap weight and projection, it is recommended that the HyPAD technique be considered for patients who desire a breast that cannot be restored with their own flap weight and wish to avoid implants.
Introduction
Many patients who undergo mastectomies, for both preventive and curative reasons, choose to undergo breast reconstruction. Breast reconstruction has been shown to greatly improve patient satisfaction and overall well-being following mastectomy.1 Traditionally, the 2 main types of breast reconstruction involve implant-based breast reconstruction or autologous breast reconstruction. Implant-based breast reconstruction is widely used, as it is a relatively straightforward technique.2 However, the use of implants can also lead to many complications such as infection, seroma, and capsular contracture.2 Furthermore, implant-based reconstruction often fails to meet the aesthetic goal of looking and feeling like a natural breast; limitations such as animation deformity, disproportionate upper pole fullness, and unnatural contouring can lead to patient dissatisfaction.3 Additionally, the US Food and Drug Administration (FDA) safety communications regarding breast implant associated-anaplastic large cell lymphoma (BIA-ALCL), as well as the increased awareness of breast implant illness (BII), has led to further controversy regarding implants and has caused confusion and stress for patients.4
Flap-based reconstruction involves using a patient's tissue with its own blood supply to reconstruct the breast. There are multiple types of flap-based reconstruction, which differ in the flap-tissue donor site. The gold standard for flap-based breast reconstruction is the deep inferior epigastric artery perforator (DIEP) flap technique, in which the donor tissue is retrieved from the lower abdomen.2 While microsurgical breast reconstruction requires a longer operative time and recovery, it comes with many benefits to patients. The reconstructed breasts look and feel more natural and also change with a person's body the way that a native breast would.2 Another benefit of autologous flap reconstruction is that the rate of reconstructive failures is lower than that of implant-based reconstruction (0.3%-1.2% vs 1.9%-2.7%, respectively).5 Advancements in the field of microsurgery, the use of alternative flap sites, and patient preferences to avoid implants have widened the scope of autologous breast reconstruction.2,5
Despite increased support for autologous breast reconstruction, including better long-term patient satisfaction and improved quality of life, flap reconstruction is limited to select circumstances.6 Some patients are not ideal candidates for autologous breast reconstruction, as there is a discordance between donor site flap volume and desired breast reconstruction volume.7 In recent years, hybrid breast reconstruction, which involves the use of a flap and alloplastic or biosynthetic materials, has developed as an innovative solution to the problem of inadequate donor site volume.2 The authors have pioneered 2 of these techniques, hybrid flap, implant, lipofilling (HyFIL) and hybrid flap, pre-pectoral acellular dermal matrix (HyPAD), both of which maximize the benefits of autologous reconstruction while also providing additional projection and volume to satisfy the patient's aesthetic goals.2
The HyFIL technique is a form of hybrid breast reconstruction that uses a flap, a pre-pectoral implant, and lipofilling to provide an optimal aesthetic outcome. This technique takes advantage of both autologous and prosthetic breast reconstruction. The HyFIL technique provides an outcome more like a cosmetic breast augmentation, as the implant is covered by the body's natural tissue. However, this technique comes with the limitations of both a flap and an implant, including flap loss, infection, implant rupture, rippling, malposition, and capsular contracture.8
For the patients who are not willing to accept an implant or have a small volume discrepancy between the flap donor and recipient site, the HyPAD technique may be a viable option. In place of an implant, the HyPAD technique uses the DIEP flap with a combination of stacked pre-pectoral acellular dermal matrix (ADM), allowing for additional core projection without any implant-associated risks (Figure 1).2 ADMs are biologic matrices that are derived from either cadaver, bovine, or porcine tissue and have been used for implant stabilization, reduction in capsular contracture, and enhancement of soft tissue coverage.9-11

Figure 1. The hybrid flap, pre-pectoral acellular dermal matrix (HyPAD) technique uses the deep inferior epigastric perforator flap (A) with a combination of stacked pre-pectoral acellular dermal matrix instead of an implant, (B) allowing for additional core projection without any implant-associated risks.
The senior authors hypothesized that stacked ADM itself has a weight and volume and can be used to enhance core projection and soft tissue augmentation of a flap reconstruction. The weight of ADM has not yet been quantified in the setting of breast reconstruction. In this study, the authors aimed to quantify the benefit that ADM provides in HyPAD breast reconstruction cases.
Methods
Institutional review board approval was obtained to perform a review of all patients who underwent microsurgical breast reconstruction. From this cohort of patients, during a defined study period (August 2021 to December 2022), those who underwent breast reconstruction with a HyPAD technique were selected. All patients lacked adequate donor site volume and wished to avoid the placement of implants during their reconstruction. The HyPAD technique was performed as previously reported.2 A single cadaveric ADM was used per breast, with the thickness of the ADM selected based on the volume necessary. The ADM was sterilely removed from its box and rinsed with antibiotic solution. The ADM was cut into 2 pieces, a square piece and a thin rectangular piece. The thin rectangular piece was then folded onto itself, resulting in a smaller square ADM construct. This smaller ADM square construct was then placed in the middle of the larger square of ADM. Opposite corners of the larger square were then sutured to each other and the smaller square, creating a square-shaped ADM construct in which the larger ADM square completely enveloped the smaller ADM square. All sutures were placed with a monofilament 3-0 polydioxanonesuture (PDS) suture. The resulting ADM construct was then placed in the pre-pectoral plane, posterior to the flap.
Demographic information and outcomes were assessed. Intraoperatively, the weight (g) of the mastectomy specimen, flap donor site, and stacked ADM were recorded. Complications were also reviewed for study subjects. Follow-up was at least 1 year for all patients. Statistical analysis was performed using the Data Analysis ToolPak in Excel (Microsoft).
Results
Twenty-one patients who underwent the HyPAD technique during the study period were identified. The mean age of patients at the time of surgery was 48.9 ± 7.85 years (range, 42-57 years). The mean body mass index was 24.1 kg/m2 ± 3.3 kg/m2.
The mean mastectomy specimen weight was 436.35 g, and the mean flap weight was 370.73 g, posing an average discrepancy of 15.04%. The average weight of the ADM used to augment the flap was 81.76 g. This weight accounted for an average of 18.07% of the total reconstructed breast weight. There were no complications, including infection, seroma, mastectomy skin flap necrosis, red breast syndrome, and/or need for ADM removal.
Discussion
One of the main measures of successful breast reconstruction is the ability to achieve the patient's desired goals without sacrificing their safety or comfort.12 DIEP flap breast reconstruction is the gold standard in microsurgical breast reconstruction. However, it may not be suitable for all patients, especially those lacking adequate flap volume. The combined use of ADM with autologous flap breast reconstruction provides patients with an alternative to implants or fat grafting that allows them to obtain their desired breast volume. Based on these results, we suggest that plastic surgeons should view stacked ADM as a helpful adjunct in flap breast reconstruction cases. In some patients, it is possible to augment the flap reconstruction, as the ADM can provide around 18% of additional weight to the breast on average (Figure 2, Video).

Figure 2. Acellular dermal matrix comes in various thickness and sizes, yielding varying weights.
Video. Acellular dermal matrix can be designed in stacked fashion to augment the breast reconstruction and enhance core projection.
Providing options and alternatives in breast reconstruction is paramount to optimizing patient experience. There are patients who choose microsurgical breast reconstruction because it allows them to avoid an implant without sacrificing their desired breast reconstruction volume. Recent media coverage and social media awareness regarding BIA-ALCL and BII have led to concerns and misconceptions regarding breast implants.13,14 In fact, current trends show that individuals are less likely to recommend breast implants to a friend out of fear of BII.15 Despite the gap in public knowledge regarding implants, these findings stress the importance of alternative options for achieving adequate core projection and soft tissue augmentation without the use of an implant.
Limitations
Objective data in this study included mastectomy specimen weight, flap weight, and ADM weight. The authors acknowledge that weight is not an exact proxy for volume. The density of tissue varies per person; therefore, 2 women with similar mastectomy volumes may have differing mastectomy masses due to the inherent differences in their breast tissue.16 In addition, the density of ADM is different from the density of natural breast tissue.17 Also, 2 patients had delayed reconstruction, so their mastectomy weights consisted of their previous implants. However, the restoration of lost volume was still achieved using ADM. Another limitation is the small sample size of 21 patients, which yielded results that are less generalizable to the population. Nevertheless, this study is the first of its kind and successfully quantified the weights of ADM, which have not previously been reported. With a small sample size, the authors cannot know the effect of radiation, chemotherapy, and obesity on complications related to stacked ADM placement.
A major weakness of the study is the lack of evidence of the long-term behavior of stacked ADM in the breast reconstruction. Conventional single-layer ADM incorporates into a well-vascularized enviornment.9 The authors believe that stacked ADM does not fully incorporate with the inner layers remaining inert. However, it is the authors' belief that a capsule forms in response to the construct, similar to any foreign body. Unfortunately, like any foreign body, there is risk of infection or extrusion. Finally, the cost of ADM is high. This study did not examine the financial implications or conduct a cost-benefit analysis of this technique. The use of stacked ADM in plastic surgery is an evolving field, and the authors believe that it has a role beyond hybrid microsurgical breast reconstruction. It may have applicability in breast augmentation, mastopexy, and/or breast explant surgery.
Given the benefits of flap-based breast reconstruction, including increased patient satisfaction with the operation and cosmetic outcome, an increasing number of women will likely undergo this operation in the coming years.18-20 It has been found that women who received a DIEP flap had better social relationships following the surgery compared with women who had implant-based breast reconstruction.21 Women who choose to undergo DIEP flap breast reconstruction are motivated by the natural look and feel of the reconstructed breasts.22 For those who desire autologous flap reconstruction but do not have adequate donor site volume to benefit from a flap reconstruction alone, hybrid breast reconstruction using stacked ADM is a viable option.
Conclusions
The use of ADM in breast reconstruction is becoming widely recognized because it provides structural support and volume. Stacked ADM can measurably benefit hybrid breast reconstruction by increasing reconstructive volume.

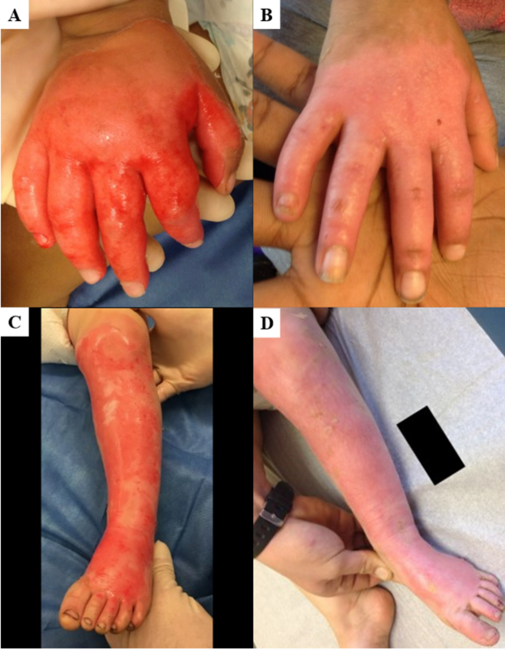
Figure 3. Frontal views are shown (A) before and (B) after deep inferior epigastric perforator flap breast reconstruction with prepectoral stacked acellular dermal matrix.
Acknowledgments
Authors: Anna E. Daytz, BS1; Julia B. Silverman, BS1; Raquel A. Minasian, MD2; Susana Benitez Sanchez, MD2; Jina Yom, BA1; Christopher Aiello, BS2; Emma Robinson, BS1; Mark L. Smith, MD1,2; Neil Tanna, MD, MBA1,2
Affiliations: 1Donald & Barbara Zucker School of Medicine at Hofstra/Northwell, Hempstead, New York; 2Division of Plastic and Reconstructive Surgery, Northwell Health, Great Neck, New York
Correspondence: Neil Tanna, MD; ntanna@northwell.edu
Ethics: Name: Human Research Protection Program Institutional Review Board. Approval Code: IRB #: 23-0398. Approval date: June 8, 2023. Helsinki Statement: All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study. Written consent was received from all patients who appear in identifying photographs and videos.
Disclosures: The authors disclose no relevant financial or nonfinancial interests.
References
1. Yueh JH, Slavin SA, Adesiyun T, et al. Patient satisfaction in postmastectomy breast reconstruction: a comparative evaluation of DIEP, TRAM, latissimus flap, and implant techniques. Plast Reconstr Surg. 2010;125(6):1585-1595. doi:10.1097/PRS.0b013e3181cb6351
2. Tanna N, Barnett SL, Robinson EL, Smith ML. Hybrid microsurgical breast reconstruction: HyFIL & HyPAD techniques. Clin Plast Surg. 2023;50(2):337-346. doi:10.1016/j.cps.2022.10.006
3. Stillaert FBJL, Lannau B, Van Landuyt K, Blondeel PN. The prepectoral, hybrid breast reconstruction: the synergy of lipofilling and breast implants. Plast Reconstr Surg Glob Open. 2020;8(7):e2966. doi: 10.1097/GOX.000000000000296
4. McGuire PA, Glicksman C, McCarthy C, Spiegel A. Separating myth from reality in breast implants: an overview of 30 years of experience. Plast Reconstr Surg. 2023;152(5):801e-807e. doi: 10.1097/PRS.0000000000010488
5. Chu MW, Samra F, Kanchwala SK, Momeni A. Treatment options for bilateral autologous breast reconstruction in patients with inadequate donor-site volume. J Reconstr Microsurg. 2017;33(5):305-311. doi:10.1055/s-0037-1599074
6. Panchal H, Matros E. Current trends in post-mastectomy breast reconstruction. Plast Reconstr Surg. 2017;140(5S Advances in Breast Reconstruction):7S-13S. doi: 10.1097/PRS.0000000000003941
7. Kanchwala S, Momeni A. Hybrid breast reconstruction-the best of both worlds. Gland Surg. 2019;8(1):82-89. doi:10.21037/gs.2018.11.01
8. Handel N, Cordray T, Gutierrez J, Jensen JA. A long-term study of outcomes, complications, and patient satisfaction with breast implants. Plast Reconstr Surg. 2006;117(3):757-767; discussion 768-772. doi:10.1097/01.PRS.0000201457.00772.1D
9. Margulies IG, Salzberg CA. The use of acellular dermal matrix in breast reconstruction: evolution of techniques over 2 decades. Gland Surg. 2019;8(1):3-10. doi:10.21037/gs.2018.10.05
10. Breuing KH, Colwell AS. Inferolateral AlloDerm hammock for implant coverage in breast reconstruction. Ann Plast Surg. 2007;59(3):250-255. doi:10.1097/SAP.0b013e31802f8426
11. Colwell AS, Breuing KH. Improving shape and symmetry in mastopexy with autologous or cadaveric dermal slings. Ann Plast Surg. 2008;61(2):138-142. doi:10.1097/SAP.0b013e31815bfe7c
12. Nahabedian MY. Achieving ideal breast aesthetics with autologous reconstruction. Gland Surg. 2015;4(2):134-144. doi:10.3978/j.issn.2227-684X.2015.03.03
13. Alothman SA, Alghannam AF, Almasud AA, Altalhi AS, Al-Hazzaa HM. Lifestyle behaviors trend and their relationship with fear level of COVID-19: cross-sectional study in Saudi Arabia. PloS One. 2021;16(10):e0257904. doi:10.1371/journal.pone.0257904
14. Bouhadana G, Chocron Y, Azzi AJ, Davison PG. Perception of implants among breast reconstruction patients in Montreal. Plast Reconstr Surg Glob Open. 2020;8(9):e3116. doi:10.1097/GOX.0000000000003116
15. Azzi AJ, Almadani Y, Davison P. A national survey to assess the population's perception of breast implant-associated anaplastic large cell lymphoma and breast implant illness. Plast Reconstr Surg. 2021;147(4):795-803. doi:10.1097/PRS.0000000000007700
16. Bodewes FTH, van Asselt AA, Dorrius MD, Greuter MJW, de Bock GH. Mammographic breast density and the risk of breast cancer: a systematic review and meta-analysis. Breast. 2022;66:62-68. doi:10.1016/j.breast.2022.09.007
17. Kim JYS, Davila A, Fine N. Breast reconstruction with acellular dermis. Medscape. May 3, 2023. Updated February 20, 2024. Accessed May 21, 2023. https://emedicine.medscape.com/article/1851090-overview
18. Bresser PJC, Seynaeve C, Van Gool AR, et al. Satisfaction with prophylactic mastectomy and breast reconstruction in genetically predisposed women. Plast Reconstr Surg. 2006;117(6):1675-1682. doi:10.1097/01.prs.0000217383.99038.f5
19. Visser NJ, Damen THC, Timman R, Hofer SOP, Mureau MAM. Surgical results, aesthetic outcome, and patient satisfaction after microsurgical autologous breast reconstruction following failed implant reconstruction. Plast Reconstr Surg. 2010;126(1):26-36. doi:10.1097/PRS.0b013e3181da87a6
20. Damen THC, Timman R, Kunst EH, et al. High satisfaction rates in women after DIEP flap breast reconstruction. J Plast Reconstr Aesthet Surg. 2010;63(1):93-100. doi:10.1016/j.bjps.2008.08.019
21. Tønseth KA, Hokland BM, Tindholdt TT, Abyholm FE, Stavem K. Quality of life, patient satisfaction and cosmetic outcome after breast reconstruction using DIEP flap or expandable breast implant. J Plast Reconstr Aesthet Surg. 2008;61(10):1188-1194. doi:10.1016/j.bjps.2007.05.006
22. Gopie JP, Hilhorst MT, Kleijne A, et al. Women's motives to opt for either implant or DIEP-flap breast reconstruction. J Plast Reconstr Aesthet Surg. 2011;64(8):1062-1067. doi:10.1016/j.bjps.2011.03.030