

Threat of Gun Violence Goes Beyond Individual Health
With the rise of gun violence across the United States, health care professionals and stakeholders across the continuum of care are calling out for recognition of gun violence as a public health issue.
Long-fought-for recognition that the ill effects of tobacco use could be prevented to save lives and reduce the extraordinary costs to society led to a full throttle public health campaign that continues to this day.1 It took scientific study, advocacy from health professionals, legislative action against the tobacco industry, and a groundswell of grassroots efforts to turn the perception of tobacco use from its once lauded status as Marlboro “cool” to its now broad acceptance as a public health hazard.
According to many, gun violence requires a similar approach. As the most common cause2,3 of homicide and suicide nationwide—79% of murders and 53% of suicides involve a gun according to 2020 US statistics—gun violence ranks second only to overdose and poisoning as the leading cause of injury deaths in 2020. For children, gun violence ranks as the highest cause of death with more than 10,000 under the age of 25 years killed by guns in 2020. Violence from guns is endemic to many under-resourced areas and has spread to suburban and rural areas with growing devastation.2
Like tobacco use, gun violence is ubiquitous and reaches far beyond the individual victims targeted to entire communities. Mass shootings have begun to highlight this fact weekly, but daily under-the-radar shootings have long taken a toll on communities outside of mainstream media.
The US Centers for Disease Control & Prevention (CDC) estimates3 that 124 people die each day from a firearm-related injury, of which more than half are from suicide and the rest from homicides. Young Black men in particular4 are at high risk and are 20 times more likely to be a victim of gun homicide than young White men.
Unlike tobacco, for which years of research was required to establish the often-fatal connection between smoking and disease, the effects of gun violence are immediate and known. Hospitals and health care providers see the effects daily, and the cost of care of victims of gun violence goes well beyond caring for the physical damage of gunshot wounds to include the long-term care needed to address the trauma of such wounds to the victim, family, and community.
For years, the health care industry and others have pushed for recognition of gun violence as a public health issue in the same vein as tobacco use. In 2016, the American Medical Association5 first declared firearm violence as a public health crisis and over the years, including recently after the Buffalo, Uvalde, and Highland Park mass shootings, other health care organizations are joining in their support.
“When we say gun violence is a public health issue, we mean it in a very concrete way,” said Kyle Fischer, MD, MPH, clinical assistant professor of emergency medicine at the University of Maryland School of Medicine. “That is, we can use principles of public health to make our patients’ lives better.”
Public Health: The Benefits to Better Addressing Gun Violence
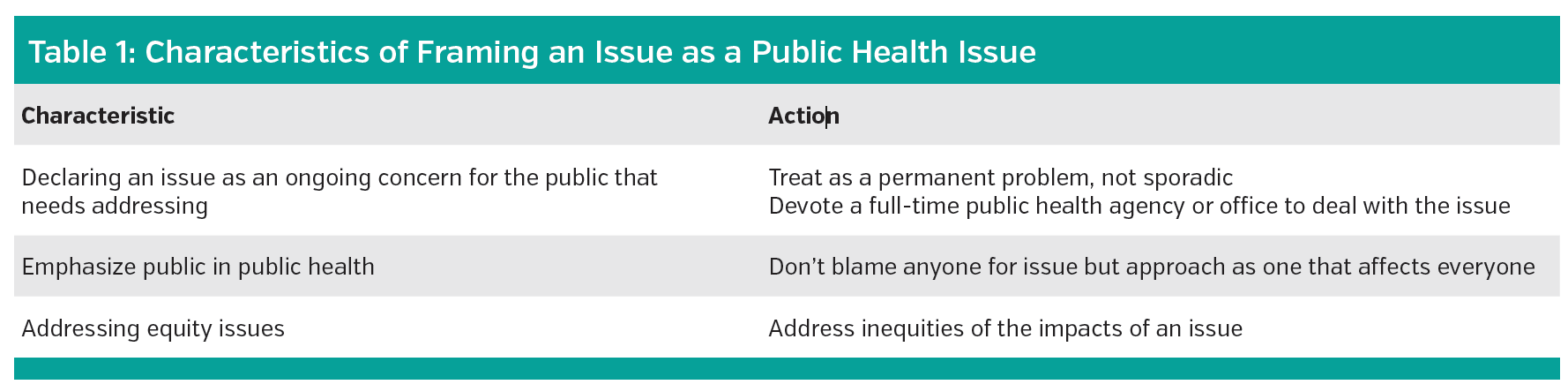
Michael Siegel, MD, MPH, a visiting professor in the department of public health and community medicine at Tufts University School of Medicine, whose research has long focused on tobacco and more currently firearms as public health issues, listed 3 benefits of calling an issue a public health issue (Table 1).
Fleshing these out, Dr Siegel said the first step in declaring something an issue is one that affects the health of the public and one that is currently not being addressed adequately. “The significance of that is it means we are not going to stop until we adequately address the problem.” When it comes to gun violence, he said that currently it is treated as a sporadic problem only and “essentially after each mass shooting.”
If gun violence were treated as a public health issue it would be seen as a permanent issue that requires a dedicated public health agency or office to deal with like the CDC’s Office of Smoking and Health,6 which was established to address tobacco as a public health issue.
Another key characteristic is to view the issue as affecting the public as a whole, which requires not assigning blame to any one individual or entity. “As a public health problem, we don’t blame people for their behaviors if they are doing things that are unhealthy,” said Dr Siegel. “The public is the entire public.” With guns, he added, there is a tendency to vilify gun owners and see them as the problem and the gun culture as the problem.
“Gun owners are members of the public and are served by public health,” he emphasized, stressing that the problem of gun violence is not between gun owners and people who do not own guns but rather between the public and a powerful National Rifle Association (NRA) industry/lobby. “Research shows that gun owners support basic forms of legislation around gun usage,” he said, but, he added, the NRA consistently frames the issue as between gun owners and non-gun owners, which in turn creates animosity and stunted progress.
Dr Siegel, who worked for 2 years within the Office of Smoking and Health, said he has insider knowledge of how the office worked to establish tobacco as a public health issue. He underscored that the same tactics used by the NRA to pit the public against each other (gun owners with rights over non gun owners) was similar to what the tobacco industry did for years in pitting smokers (with rights) over nonsmokers. “Eventually, we in the tobacco movement changed the framing from smokers against nonsmokers to the public vs big tobacco, and that was the beginning of the end to what led to all the interventions that eventually led to the drastic decline in the clout of the tobacco industry and decline in smoking.”
As to equity, Dr Siegel suggested that a public health issue recognizes inequities in the public that places certain communities at higher risk. “For firearms, we have one of the most racial inequities I have ever seen,” explaining there is a 5-fold higher incidence of deaths from firearms among the Black population compared with White people. “The implication is that we can not just be concerned about school shootings [and other places of mass shooting] but also about the daily violence especially as it disproportionately affects the Black community,” which he said should take priority.
Stopping the Cycle of Gun Violence
For Andrew Woods, executive director of the Hartford Communities That Care, Inc, (HCTC) a nonprofit organization that works with hospitals and other partners to coordinate critical services for victims of gun violence to stem its cyclic nature in high-risk communities, calling gun violence a public health issue is about elevating its importance.
“If the issue is considered an individual issue or only a clinical issue, then it is pretty much dealt with that way from a medical and behavioral standpoint,” he said. “But when you elevate it as a public health issue, it is then no longer just about individuals and their families but an issue that impacts everyone.”
Mr Woods sees the impact of gun violence daily in the community he serves. As a former mental health professional working in a local middle school in Hartford, CT, he witnessed the cycle of violence—often gun related—among the youth he counselled and strove to find ways to stop youth from entering that cycle in the first place. In his current role, he has found a way to do just that through HCTC which focuses on breaking the cycle by focusing on the short- and long-term effects of gun violence on victims, their families, and communities.
In 2004, HCTC partnered with a local hospital (Trinity-St. Francis Hospital and Medical Center of Hartford) to address the health and medical needs of victims of gun shot wounds and other violent assaults through the creation of the Hartford Crisis Response Team. The aim of the partnership is to interrupt the cycle that perpetuates gun violence, and other violent assaults, by offering evidence-based practices to reduce future morbidity and mortality in victims, preventing retaliatory violence, and increasing community safety. Evidence-based practices include offering case management to victims, clinical care, safety planning, peer support, information, referrals, and connection to community resources.
Based on this work, HCTC was designated as a Hospital-Linked Violence Intervention Program (HVIP)—the only one in the state of Connecticut.
Dr Fischer, who is the policy director for the Health Alliance for Violence Intervention (HAVI), a nonprofit that helps launch and support new and emerging HVIPs,7 described the programs as a way of engaging with victims of firearm violence in the health care setting over time to ensure patients fully recover physically and psychologically. Saying that patients seen in the hospital for gunshot wounds are at exceedingly high risk (approximately 30%) of returning to the hospital with another gunshot wound, he explained HVIPs offer a golden opportunity to meet patients where they are to help them access services that go well beyond the clinical care for the wound alone and address the cycle of violence that perpetuates further violence. “The old paradigm of treating patients for physical wounds and discharging them doesn’t work,” said Dr Fischer.
Instead, HVIPs involve a team approach in which physicians, nurses, case managers, and violence prevention professionals such as social workers and counselors, address all the needs of the patient over 6 months to 1 year after hospital discharge. The goal is to minimize the risk of the patient from being reinjured, minimize retaliatory behavior, and ensure the patient makes a full recovery, Dr Fischer explained.
The effects of HVIPs speak for themselves. Dr Fischer pointed to observational data8 showing the rates of repeat violent injury after the implementation of an HVIP is less than 5%. Without any intervention program like an HVIP, historical data show rates of repeat violent injury ranging from 8% to 63%.
From a health care perspective, an intervention that resulted in a 5% repeat injury rate would be a “slam dunk for approval as a treatment,” according to Dr Fischer.
“HVIPs are a great example of how the principles of public health work in practice,” Dr Fischer said. “They show that there are ways of taking care of patients to improve and save lives, improve society, and make the world a safer place.”
To date, there are 85 working or emerging HVIPs nationwide, up from 7 in 2009. For a more complete description of how they work, visit www.thehavi.org.
Reimbursement
As with any intervention, reimbursement for services is critical. Dr Fischer described a number of funding streams, including 19 different federal funding streams eligible for community violence intervention. The Victims of Crime Act also provides grant funds, which the governor of New Jersey, for example, tapped into for a $20 million investment for a network of HVIPs across that state.
Medicaid funds are also now available, with 5 states currently taking advantage of these funds for reimbursing their HVIPs. Connecticut is the first state in the nation to pass legislation to permit Medicaid dollars to reimburse services for gun violence protection. Mr Woods, who helped lead the effort to pass the legislation, said it was vitally important to get a consistent revenue stream to reimburse HVIP services. “Medicaid is probably one of the most consistent funding streams,” he said, saying that Medicaid dollars, under the new Connecticut law implemented as of July 1, 2022, can now be used to reimburse trained and certified violence prevention professionals for a wide range of services: patient screening and assessment, development of individualized treatment plans, case management support, mentorship, and crisis intervention for patients referred to violence prevention professionals by a trauma 1 or trauma 2 hospital.
“Under the [Connecticut law], hospitals currently refer a victim of gun violence or violent crime to certified prevention professionals [such as an HVIP] who provide the wrap around service supports that public-private partnerships can provide,” said Mr Woods.
Incorporating an HVIP or other violent prevention program as an intervention for victims of gun violence is predicted to save lives and monies by preventing repeat violence, according to Woods, who cited data from an HCTC assessment9 that looked at the expected value-return on investment (EV-ROI) for 6 outcome categories. The value of follow-up medical care was measured with the following categories: (1) prevents emergency room use; (2) hospital readmission, (3) the value of social-emotional learning that leads to less retaliation, fewer violent crimes, and fewer visits to the emergency department; (4) increased tax revenue; (5) public assistance savings; and (6) shifting of the Medicaid burden to another payer from helping patients embark on a positive life path leading to graduation from high school or vocational training and ultimately a full-time job and career.
The study assessed the EV-ROI of these outcomes on a total of 47 patients with gunshot wounds treated at Trinity-St. Francis hospital and refereed for in-home and outpatient violent prevention treatment. The study showed a combined savings for hospitals, Medicaid, and taxpayers of $4,143,885 at a cost of $290,976, which represents a net gain of $3,952,909 for the 3 entities with a benefit-cost ratio of 14.2 to 1.
“If you can reduce recidivism of gun shot victims or victims of violent crime with the necessary supports than you can accelerate their recovery process, which means speeding up the medical and behavioral health process and accelerating the potential for improved outcomes with subsequent lower cost,” said Mr Woods. “Absent that, you find more victims at increased risk of further injury or diminished of the healing process and that is more costly to patients, hospitals, and taxpayer.”
For health care providers and systems, HVIPs and other violence prevention programs are tangible ways to help interrupt the cycle of violence that characterize gun violence and can have a real and lasting impact on individuals affected by gun violence and the communities in which they live. “Gun violence is not going away,” said Dr Siegel. “We need to treat this as a public health problem, and not just say we need to do something.”
References
1. US Centers for Disease Control and Prevention. Smoking and tobacco use. June 27, 2022. Accessed July 22, 2022. https://www.cdc.gov/tobacco/index.htm
2. Gramlich J. What the data says about gun deaths in the US. Pew Research Center. February 3, 2022. Accessed July 22, 2022. https://www.pewresearch.org/fact-tank/2022/02/03/what-the-data-says-about-gun-deaths-in-the-u-s/
3. US Centers for Disease Control and Prevention. Violence prevention, fast facts. May 4, 2022. Accessed July 22, 2022. https://www.cdc.gov/violenceprevention/firearms/fastfact.html
4. The Johns Hopkins Center for Gun Violence Solutions. A year in review: 2022 gun deaths in the US. April 28, 2022. Accessed July 22, 2022. https://publichealth.jhu.edu/sites/default/files/2022-05/2020-gun-deaths-in-the-us-4-28-2022-b.pdf
6. US Centers for Disease Control and Prevention. Office on Smoking and Health OSH). November 16, 2021. Accessed July 22, 2022. https://www.cdc.gov/tobacco/about/osh/index.htm
7. National Network of Hospital-Based Violence Intervention Programs. NNHVIP Policy White Paper: Hospital-based Violence Intervention: Practices and Policies to End the Cycle of Violence Accessed July 22, 2022. static1.squarespace.com/static/5d6f61730a2b610001135b79/t/5d83c0d9056f4d4cbdb9acd9/1568915699707/NNHV IP+White+Paper.pdf
8. Greene MB. Repeat injuries, variability and recommended research guidelines. Presented at: Healing Justice Alliance National Conference; August 22, 2016; Baltimore, MD.
9. Social Capital Valuations. First Generation EV-ROI Model for Hartford Communities That Care’s Hartford Crisis Response Team/Hospital-Linked Violence Intervention Program. Connecticut General Assembly.



