


Oncology Pathways Drive Adoption of High-Quality Treatment Regimens and Deliver Drug Cost Savings
Abstract
In an environment of rapid innovation and sharply rising costs, oncology clinical pathways are a solution that can help bridge knowledge gaps for providers and ensure patients get quality, affordable cancer care. Cigna and eviCore Healthcare developed an Oncology Value-based Pathways (VP) program by incorporating several value frameworks and considering the perspectives of multiple stakeholders, including patients, providers, and payers. Starting January 1, 2021, the VP program was implemented for a large commercial population, spanning 51 clinical pathways and covering 50% of cancers. Over an 18-month period, the VP program increased the on-pathway regimen rate by 5.2%, leading to a cost savings of $24 million or $0.13 per member per month in a commercial managed population. Direct peer-to-peer conversations with providers who ordered off-pathway regimens led to updated requests for on-pathway regimens in 18.3% of cases. Additionally, 28.3% of total cases were moved to on-pathway regimens, regardless of whether there was a peer-to-peer discussion with the provider, indicating the VP program’s durable educational impact.
Introduction
Medical knowledge is growing at unprecedented rates and picking up speed every year. In 1950, it took 50 years to double medical knowledge. In 2010, it took 3.5 years. In 2020, it was estimated to be 73 days.1
In oncology, the National Comprehensive Cancer Network (NCCN) made over 150 updates to their published cancer guidelines and compendia in 2018 alone.2 The number of evidence-based medical journals and resources is increasing to a point where, one oncologist wrote, it would take more than 627 hours a month—about 21 hours a day—of reading to keep pace.3
While positive for medical innovation, this information explosion creates challenges for providers. A recent survey found that 95% of physicians want to learn more about new trials, treatments, or procedures that could help improve outcomes for their patients, but more than two-thirds of them, and 80% of oncologists, report feeling overwhelmed by the amount of information they must keep up with.4
As a result of these knowledge gaps, patients do not always receive evidence-based care. Research shows that as many as half of all cancer treatments (47%) do not follow the latest scientific recommendations.5
At the same time, oncology costs are rapidly increasing. Spending for cancer drugs was $185 billion in 2021, which is a 50% increase from 2017, and costs are forecasted to reach $307 billion by 2026. The pipeline for new drugs is also strong, with oncology trials reaching historic highs in 2021, up 56% from 2016.6
Adherence to guidelines, such as those from NCCN, has shown the potential to reduce the oncology costs. However, additional measures are needed to drive high-value cancer care. Clinical pathways are a solution that can help bridge knowledge gaps for providers and ensure patients get quality, affordable cancer care. According to the American Society of Clinical Oncology (ASCO), “High-quality oncology clinical pathways are detailed, evidence-based treatment protocols for delivering cancer care to patients with specific disease types and stages. When properly designed and implemented, oncology pathways can serve as an important tool in improving care quality and reducing costs.”7
ASCO has developed criteria that should be met when creating oncology clinical pathways. They include transparent pathway development with a clear, consistent process and methodology. The pathways should be clinically driven, with established methodology for prioritizing efficacy, safety, and cost. The pathways should also be patient-focused, including alternative evidence-based options to account for differences in patient characteristics or preferences.
Several leading oncology organizations, such as ASCO, NCCN, and the European Society for Medical Oncology (ESMO), have also developed value-based oncology frameworks. For example, the ASCO Value Framework Net Health Benefit score and ESMO Magnitude of Clinical Benefit scale are both intended to be objective measures of the clinical benefits of oncology drug treatments.8 Though these frameworks are similar, some key differences between ASCO and ESMO frameworks include weighting of toxicities and of absolute and relative gains in survival, as well as distinct approaches for rewarding long-term survival benefits. However, a study showed a high correlation between the frameworks in determining the relative value of treatments in the noncurative setting.9
NCCN has also added value-based components to its guidelines, including evidence blocks, which measure five components of value for treatment regimens, as well as development of categories of preference, which consider efficacy, toxicity, and, when appropriate, cost.
eviCore Healthcare (eviCore), an Evernorth Health Services company that manages medical benefits, uses an innovative clinical decision support model to assist providers in selecting the most clinically appropriate, highest-value cancer regimens. eviCore’s standard medical oncology prior authorization program approves any NCCN-approved regimen. To expand on this approach, eviCore’s and Cigna’s clinical teams developed an Oncology Value-based Pathways (VP) program.
In building the VP program, the clinical teams sought to create an objective and reproducible methodology, including the ASCO Value Framework Net Health Benefit score, ESMO Magnitude of Clinical Benefit scale, and NCCN guidelines value-based components. Through a proprietary weighted scoring methodology using these frameworks, the clinical teams are able to assign a value-based score for each regimen. That score is based on efficacy, safety, and other outcome components, such as quality of life improvements. Cost is considered only when two or more regimens had a value-based score within 10% of each other. The clinical teams also identified appropriate clinical exceptions for preferred on-pathway regimens, recognizing that patient-specific characteristics impact the value of various treatment options. All on-pathway regimens are a subset of NCCN-recommended regimens.
In settings where the available NCCN-recommended regimens had evidence only from single-arm, nonrandomized trials, the clinical teams were unable to apply a multiframework methodology. Instead, the available literature was reviewed, and a clinical consensus approach was applied to identify on-pathway regimens.
Each pathway underwent extensive clinical validation. Internally, it was evaluated by medical oncologists, pharmacists with extensive oncology experience, and a dedicated enterprise Pharmacy and Therapeutics Committee. External validators included medical oncologists from community-based practices, as well as disease-specific experts from National Cancer Institute–designated centers and NCCN member institutions. All feedback on the pathways were considered prior to finalization.
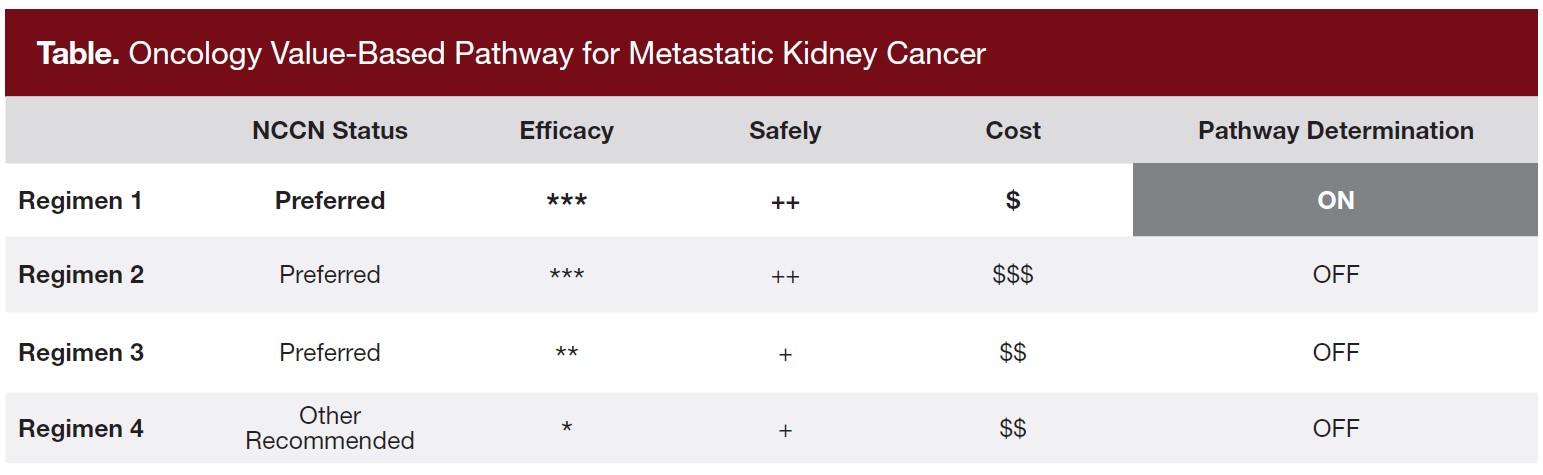
The oncology value pathway for metastatic kidney cancer provides a good example of how the VP program works. For a patient with poor or intermediate risk, NCCN recommends four treatments. When the VP model is applied, the ipilimumab/nivolumab regimen (Table; Regimen 1) is associated with the greatest clinical benefit and cost effectiveness. In addition to highlighting this regimen in its clinical decision support tool, eviCore provides clinical consultation if a provider selects a lower-value treatment regimen. In the consultation process, the provider is sent a brief synopsis highlighting the higher clinical benefit of the preferred option, and proactive peer-to-peer (P2P) outreach is also initiated by an eviCore medical oncologist to review the information together. In addition to better outcomes for patients, the estimated drug-cost savings is up to $170,000 per year per patient over some of the other NCCN-recommended regimens.
Methods
Beginning January 1, 2021, Cigna and eviCore implemented the VP program in a large commercial population. The VP program tiers NCCN-approved regimens into preferred (on-pathway) and nonpreferred (off-pathway) categories for specific clinical cohorts based on patient outcomes, quality of care, and value. Between January 1, 2021, and January 1, 2022, the VP program was developed and implemented in 3 phases, spanning 51 clinical pathways and covering 50% of cancers.
Prior authorization requests made for off-pathway regimens in these clinical cohorts result in a P2P discussion between the requesting physician and an eviCore medical oncologist with the intent of redirecting the requesting physician to an on-pathway selection. As it is designed to provide clinical decision support, there are no denials issued for off-pathway selections, and providers are not required to switch to on-pathway regimens. eviCore tracks the outcomes of these P2P conversations. If the requesting provider chooses to stay with the off-pathway regimen after the P2P, eviCore records whether this was due to patient-specific contraindications to the on-pathway regimens, a continuation of care request, or individual physician preference.
Three metrics evaluate the impact of the VP program: the on-pathway regimen improvement rate, the successful P2P rate, and the opportunity impact rate.
Prior authorization data collected from the 12 months prior to implementation of each phase was used to determine the baseline on-pathway regimen rate by cohort (approved authorizations for on-pathway regimens/approved authorizations for total on-pathway and off-pathway regimens). The on-pathway regimen rate in the baseline period was compared to the rate in the post-implementation period to determine on-pathway regimen rate increase. This first metric does not exclude clinical exceptions, which are defined as patient-specific contraindications and continuation of care, as this information was not being tracked in the baseline data.
The second and third metrics both exclude patients with clinical exceptions from the denominator. The successful P2P rate captures the direct impact of the P2P discussions by tracking how many resulted in an updated request from an off-pathway regimen to an on-pathway regimen.
The opportunity impact rate captures both the direct impact of the P2P discussions and the indirect educational impact of the program. It is calculated by dividing the number of patients impacted by the opportunities for impact. The patients impacted are calculated by multiplying the on-pathway regimen improvement rate by the post-implementation authorization volume. This captures both direct and indirect shifts.
Results
Results are provided for the three core metrics from January 1, 2021, through June 30, 2022. Overall, the VP program has delivered an estimated oncology-related drug savings of $24 million or $0.13 per member per month in a commercial managed population. The savings were calculated based on the average sales price (ASP) of the drugs as published by the Centers for Medicare & Medicaid Services (CMS). There were no drug discounts or rebates included in the VP program.
Metric 1: On-Pathway Regimen Improvement Rate
In the 12 months prior to program implementation, there were 6,218 authorization requests with a combined 71.9% on-pathway regimen rate within the applicable cohorts. In the 18 months post-implementation, there were 7,146 authorization requests, and the on-pathway rate increased to 77.1%, which is an overall improvement of 5.2%.
Metric 2: Successful P2P Rate
In the 18-month program history, there have been 972 P2P conversations between requesting physicians and eviCore medical directors. Of those total P2Ps, 475 did not include clinical exceptions, which are patient-specific contraindications or continuation of care requests. These would not be considered opportunities to shift a patient from an off-pathway regimen to an on-pathway regimen. Of the 475 P2P conversations without clinical exceptions, 18.3% (87) directly resulted in an updated request from an off-pathway regimen to an on-pathway regimen.
Metric 3: Opportunity Impact Rate
There were 417 total patients shifted due to the VP program in the first 18 months, and there were 1,473 opportunities for impact (the sum of all patients shifted plus all cases that ended with an off-pathway regimen selection that do not meet the clinical exception criteria). As a result, the opportunity impact rate is 28.3% (417/1,473).
To note an important difference between the second and third metrics, the successful P2P rate captures the direct impact of the P2P discussions following a nonpreferred regimen selection. The opportunity impact rate captures the direct and indirect impacts of the program, as it includes patients shifted to an on-pathway regimen whose physician did not have a direct P2P conversation. Indirect impacts are likely the result of the clinical decision support system notifying the ordering providers that on-pathway regimens are higher value and have better outcomes. The difference between the opportunity impact rate and the successful P2P rate captures the durable educational impact of the program.
Discussion
Oncology pathways have the potential to support clinical decision making by highlighting the treatment regimens associated with the best efficacy or safety profile. If those factors are equal, pathways also allow consideration of the relative cost-effectiveness of available treatment options. This research offers promising evidence that effective pathways based on high-quality evidence and applied accurately to individual patient regimen decisions can lead to better adoption of on-pathway regimens and lower costs.
Limitations and Opportunities
To date, objective studies demonstrating that oncology pathways positively impact costs and patient outcomes have been limited. The VP program shows that an educational steerage model can be effective at increasing pathway adoption with substantial demonstrable savings. However, eviCore’s ability to currently document improved patient outcomes is limited due to insufficient access to longitudinal clinical record data in this cohort to identify statistically significant differences. As these data become more mature, eviCore is planning to share information such as overall disease-free survival rates, as well as other important quality of life measures. Further analysis is also possible to evaluate progression and toxicity data.
Another consideration is that these data do not incorporate the total cost of care. The focus is solely on drug costs because those costs are easily obtainable through claims. However, if oncology pathways are developed, maintained, and applied correctly, they should not only reduce drug costs but also improve patient disease outcomes, which should lower the total cost of care.
For example, a study compared quality-of-care outcomes for patients with breast cancer who received an on-pathway regimen versus those who did not. It found that the average post–6-month cost of care was $16,176 lower in the on-pathway cohort.10 Future research that considers pathways’ effects on total cost of care would contribute to understanding the extent to which they can be impactful beyond drug costs.
VP Model Benefits and Possible Applications
The VP program represents a significant improvement over traditional models for medical oncology decision support. By incorporating several value frameworks in its pathway development process, the clinical teams were able to consider the perspectives of multiple stakeholders, including patients, providers, and payers. It is also important to note that the pathway development methodology was supported by extensive clinical review and encompasses analytic validity, clinical validity, and clinical utility. Due to its unique approach, eviCore was approved for a patent for the VP model.11
Provider-friendly approaches like the VP model, which account for clinical efficacy, safety, quality of evidence, and affordability, are likely to have increasing applications, particularly in alternative payment models. For example, CMS recently announced its Enhancing Oncology Model (EOM), which went live in July 2023.12 Unlike its predecessor, the Oncology Care Model, the EOM will require participants to accept downside risk.13 As providers consider joining these types of models, they are likely to seek highly effective tools like the VP program that can help them lower drug costs relative to the baseline while maintaining positive patient outcomes.
Additionally, the results of this study suggest the viability of an educational P2P approach for pathways programs. The VP program was able to achieve a rate of on-pathway regimen adoption to similar studies without the use of financial incentives or prior authorization denials.14
Future Role for Pathways
Innovation in oncology is growing at unprecedented rates, which are expected to continue to increase. These advancements are good for patients if they can be accurately incorporated into care regimens. The challenge is that medical knowledge is advancing at a pace that is difficult for providers to keep up with. At the same time, rising oncology costs are putting significant strain on patients, payers, and the health care system. This study demonstrates the role innovative new approaches like the VP model can play in ensuring the adoption of quality treatment regimens for patients and lowering oncology drug costs.
At the same time, an opportunity exists for expanding oncology clinical pathways to become more comprehensive in scope, which may help close gaps in patient care. Winston Wong, PharmD, recently suggested transforming current clinical pathways into broader “care pathways.” He wrote, “In a care pathway, the clinical pathway becomes a component, along with pathways for diagnostics, social determinants of health and patient preference, patient engagement/navigation, and payer/employer interfaces. These pathways would be supported by the backbone of real-world data from existing disconnected data elements integrated into a single data set.”15
Moving toward more comprehensive, patient-centric care pathways may further support quality care amid the rapid pace of innovation in oncology care.
Author Information
Authors: Kathryn Christensen, MS; Timothy Dollear, MS; Rama Al Ghannam, PharmD; Eric Gratias, MD; Robinson Ortiz, MD; and Stephen Hamilton, MD
Affiliations: Cigna Healthcare, Bloomfield, CT; eviCore, Bluffton Healthcare, SC.
Address correspondence to:
Stephen Hamilton, MD
400 Buckwalter Place Blvd.
Bluffton, SC 29910
Email: stephen.hamilton@eviCore.com
Disclosures: K.C., T.D., and R.A.G. reported employment and stock ownership with Cigna. E.G. reported employment with eviCore; stock ownership with Cigna; and holding a related patent through Cigna. S.H. reported employment and stock ownership with Cigna; and holding a related patent. R.O. reported employment with Cigna.
References
1. Densen P. Challenges and opportunities facing medical education. Trans Am Clin Climatol Assoc. 2011;122:48-58.
2. Rausa M, Spangler D, Hamilton S, Gratias E. Use of clinical decision support and peer review to increase NCCN guideline adherence. J Clin Pathw. 2020;6(1):54-56. doi:10.25270/jcp.2020.2.00111
3. Healthcare: the big data problem of medical knowledge. Medium. Published October 22, 2014. Accessed October 12, 2022. https://medium.com/@cancergeek/ healthcare-the-big-data-problem-of-medical-knowledge-5c1e526b2cfe
4. Physician Learning Preferences. Doximity. October 2022. Accessed November 16, 2022. https://c8y.doxcdn.com/image/upload/Press%20Blog/Research%20Reports/Doximity-Physician-Learning-Report-2022.pdf
5. Ramsey SD, Fedorenko C, Chauhan R, et al. Baseline estimates of adherence to American Society of Clinical Oncology/American Board of Internal Medicine choosing wisely initiative among patients with cancer enrolled with a large regional commercial health insurer. J Oncol Pract. 2015;11(4):338-43. doi:10.1200/JOP.2014.002717
6. Global Oncology Trends 2022. IQVIA. Published May 26, 2022. Accessed November 16, 2022. https://www.iqvia.com/insights/the-iqvia-institute/reports/global-oncology-trends-2022
7. Clinical Pathways. American Society of Clinical Oncology. Accessed October 12, 2022. https://www.asco.org/news-initiatives/current-initiatives/cancer-care-initiatives/clinical-pathways
8. ASCO, ESMO publish joint assessment of their value frameworks. American Society of Clinical Oncology. Published December 17, 2018. Accessed November 16, 2022. https://old-prod.asco.org/practice-policy/policy-issues-statements/asco-in-action/ asco-esmo-publish-joint-assessment-their
9. Cherny NI, de Vries EGE, Dafni U, et al. Comparative assessment of clinical benefit using the ESMO-Magnitude of Clinical Benefit Scale version 1.1 and the ASCO Value Framework Net Health Benefit Score. J Clin Oncol. 2019;37(4):336-349. doi:10.1200/ JCO.18.00729
10. Gautam S, Sylwestrzak G, Barron J, et al. Results from a health insurer’s clinical pathway program in breast cancer. JCO Oncol Pract. 2018;14(11):e711-e721. doi:10.1200/JOP.18.00157
11. Ortiz R, Karvetski CH, Murray L, Hamilton SA, Gratias EJ, inventors; eviCore Healthcare MSI, LLC, assignee. Database framework model transformation for pathway identification. US patent 11,481,235. October 25, 2022.
12. Enhancing Oncology Model. Centers for Medicare and Medicaid Services. Accessed November 17, 2022. https://innovation.cms.gov/innovation-models/enhancing-oncology-model
13. Devino M. How does the EOM compare to the OCM? Association of Community Cancer Centers. Published July 20, 2022. Accessed November 17, 2022. https:// www.accc-cancer.org/acccbuzz/blog-post-template/accc-buzz/2022/07/20/how-does-the-eom-compare-to-the-ocm
14. Malin JL. Charting the course: use of clinical pathways to improve value in cancer care. J Clin Oncol. 2020;38(4):367-371. doi:10.1200/JCO.19.01482
15. Wong W. The future of pathways. J Clin Pathw. 2022;8(8):8.



