

De-risking Market Launch: Leveraging HEOR Evidence Planning to Support Informed Payer Decisions
Lowering health care costs has become a high priority concern for stakeholders and policymakers at all levels of the US health care system, with particular scrutiny on drug prices.1-4 In the absence of a national arbiter, such as a health technology assessment agency, to determine what drugs are “worth it,” there have been a number of state and nonstate solutions pursued. For example, the Institute for Clinical and Economic Review (ICER) has been conducting economic evaluations of existing and newly marketed drugs using a methodology similar to that of a conventional health technology assessment. Through this approach, ICER estimates the value or cost effectiveness of a drug at a given price point or assigns a value-based price when one is not provided.5
States have also stepped in to fill the gap. Several states have begun to explore the use of prescription drug affordability review boards and drug pricing transparency laws as a means to control drug costs.6 Additionally, private payers evaluate key pharmacoeconomic data when weighing coverage and reimbursement decisions to determine financial impacts to their bottom line.7 All of this has created an environment where a successful drug launch requires not only a robust clinical economic package, but also a clearly articulated economic story with supportive health economics and outcomes research (HEOR) data.
Evidence of clinical benefit generated in a randomized clinical trial (RCT) is still the gold standard for conveying the clinical value of a drug and continues to serve as the primary source of evidence for payers when making access decisions.8 But this data is also inherently limited by the structure of an RCT, which is designed to measure specific health outcomes in a carefully circumscribed patient population for a defined time period.9,10 This means short study durations, limited patient populations, and clinical endpoints that serve as surrogates for outcomes that can only be achieved over longer study periods, inhibiting a payer’s ability to fully assess a drug’s clinical merits.
These limitations can ultimately lead to more restrictive access for drugs at launch until more mature data becomes available. However, the use of HEOR data can help to close knowledge gaps and uncertainties that payers may possess when making decisions involving access and reimbursement.11-13 Health economic studies are a valuable tool for drugs pre- and postlaunch, as they help to fill evidence gaps stemming from RCTs that may involve durability, comparative effectiveness, and long-term safety.8 This article focuses on prelaunch HEOR planning to support a successful market launch (Figure).
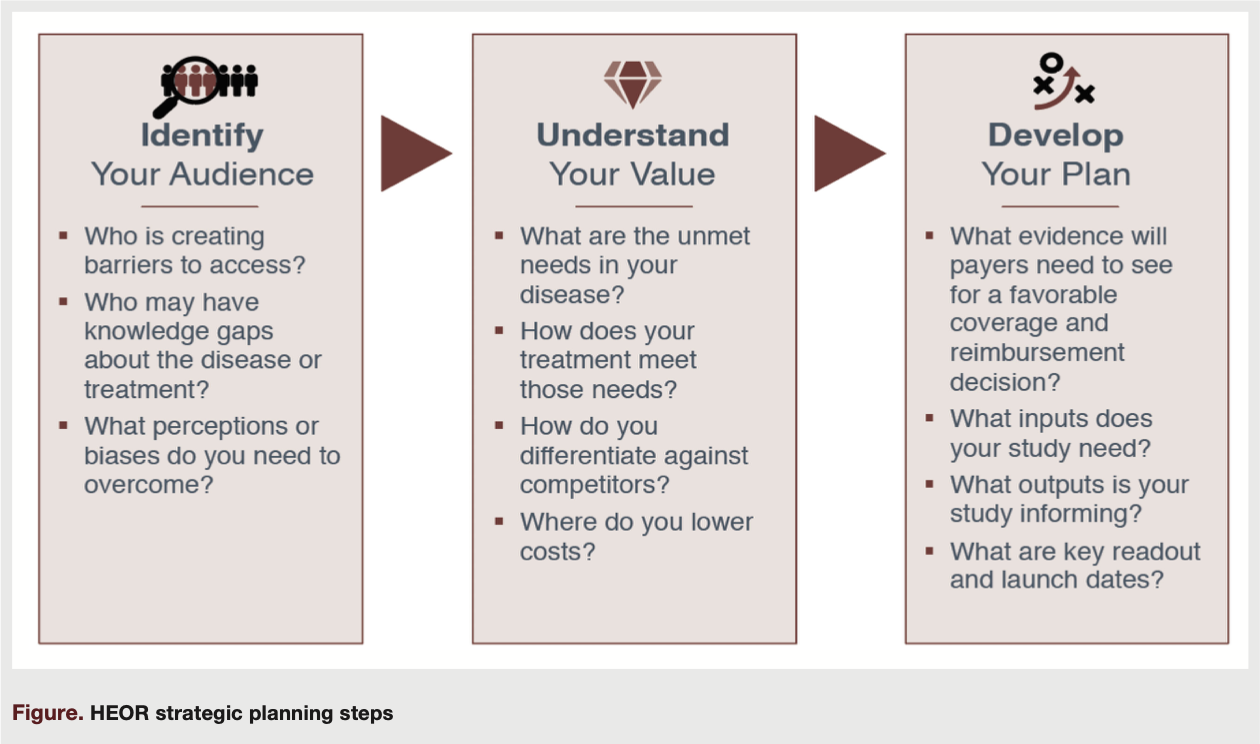
Identify Your Audience
There has been a growing appetite for HEOR in recent years, particularly for evidence generated using real-world data. Furthermore, in recent years, we have witnessed a major growth in data offerings and analytic solutions, reflecting the demand for this type of information.
In a survey of payers, 89% of respondents agreed that organizations should be open to using data from observational studies as well as RCTs in making health care decisions.14 Additionally, the FDA has begun to accept real-world data as part of regulatory submissions.15 The growing demand and utility of real-world data has extended beyond payer and drug agency evaluations into other health care stakeholders. Health care providers are taking efforts to better understand and interpret HEOR studies, and policy makers are now referencing ICER reports in key political discussions.16-19 A broad range of stakeholders are interested in evidence generated by HEOR, but their needs are not all the same. In preparing for a market launch, the payer stakeholder is likely the primary audience of concern.
Zeroing in on the payer stakeholder, it is important to perform a strategic assessment of key barriers to successful market entry prior to launch. Barriers could include access or coverage policy, but they can also extend into concerns such as high utilization and physician adoption, which are commonly seen when drug innovation occurs in a historically stagnant category or when payers have less education or experience for a new drug technology. If we focus on new drug innovations, where payers have less experience and available data prior to and following launch are limited, it is important to understand the type of HEOR data payers find most useful and how it will resonate depending upon the audience. Using cell and gene therapy as an example of high innovation but limited overall payer experience, payers may look to HEOR studies that support contracting and reimbursement initiatives or how to correlate data within their electronic medical record systems.20
Moreover, the types of evidence generated through HEOR studies will resonate differently depending on the payer type. Payers that carry greater levels of risk—such as those associated with integrated delivery networks, health systems, and regional health plans—tend to embrace HEOR studies that generate proof points for health outcomes improvement or impact to quality performance metrics. Conversely, traditional payer types may look at comparative effectiveness studies as a means for supporting contract negotiations. Ultimately knowing the primary stakeholders and their main drivers of decision-making will help to inform the HEOR evidence-generation strategy.
Understand Your Value
Articulating the value of a drug goes beyond its clinical profile and extends into understanding the disease, the burden it poses to patients, the health care system, and the needs not met by existing treatment options. The burden and unmet need in a disease space serves as the foundation for determining the compelling value of a drug. If an innovation coming to market is presenting a solution for something that is not a problem, key stakeholders will not perceive the value of that solution. In this case, the problem must then be illustrated and demonstrated.
Payers also vary in their perspective and definition of “value,” which will further vary from payer to payer. Ultimately, all payers are looking to optimize allocation of resources. Consider, for example, a drug that is more convenient to administer relative to existing products on market, such as a new oral drug formulation in a self-injectable category. Convenient dosing may not be something valued by all payer types on its face. However, convenient dosing could lead to improved adherence, which would be valuable in a drug category challenged by poor adherence. In this situation, the convenient dosing form could improve adherence and potentially improve downstream health outcomes and health care resource utilization, which would be of great interest to payers. An RCT would not be able to illustrate that information, but HEOR could be leveraged to estimate some of those potential downstream effects and provide additional context at launch.
Payers will continue to have interest in the HEOR that upholds a drug’s clinical profile, but focus may shift more intently toward population dynamics and budget impact at launch. In the absence of real-world data at launch, forecasting models can be used to estimate payer exposure and possible medical cost offsets that could be achieved through the clinical benefits of the drugs. HEOR data in this capacity can help provide context regarding comparative effectiveness in the case of a lack of direct comparative data, potential cost offsets, and the expected size of the eligible population. These pieces all serve as inputs for payers in determining how a new product may affect their budgets.
Develop Your Plan
Once the key audience for your HEOR is identified and your value drivers that will resonate with payers are clearly articulated, the last step is to structure a strategic plan. With the growing demand for HEOR, it may be tempting to dive in and kick off studies as opportunities arise. However, given limited time, resources, and competing demands while preparing for a launch, it is important to prioritize HEOR activities to support optimizing favorable access. Creating a plan ensures that “must-have” evidence is generated in time for launch, and “nice-to-have” evidence has been planned for in future budgets. A strategic plan may sound daunting, but it can be broken down into two main pieces: a prioritization framework and a timeline forecast.
A prioritization framework is centered around understanding how a particular set of data can strengthen a drug’s value proposition and ultimately favorably impact access decision-making. To start, consider how the drug is differentiated within the marketplace and its ability to address unmet needs. Second, review the existing and planned evidence to determine where the value proposition is not ideally supported. Finally, pressure test the identified evidence gaps with a payer audience to determine their evidence preferences to best close the identified gaps and differentiate the drug within the marketplace to create a framework for your plan.
Once the evidence and data needs are set, the next step is to consider implementation and determine the timeline. There are a number of factors to consider when plotting out the evidence-generation timeline. Examples include the length of time to conduct a study, knowing which studies have dependencies on the completion of others, projected interim and final data readouts, and the dissemination plan associated with the product’s launch date. Bringing these two pieces together will provide you with a robust and strategic HEOR evidence-generation plan.
Takeaway
HEOR has emerged as a core source of evidence for new drugs coming to market. It will be increasingly important for payers and health care stakeholders to become more familiarized with HEOR study designs and how to apply data findings in a practical setting. In a world where limited data, small patient populations, and accelerated drug approvals are impacting the amount of clinical evidence available to assess a drug’s clinical merits as it launches, HEOR will be critical to provide additional context and minimize uncertainties posed by data gaps. A strategic HEOR evidence-generation plan that comprehensively communicates the value of a new drug helps to ensure that patients have access to innovative drugs and health care stakeholders have access to data to ensure that safe and efficacious treatments are available.
References
1. NORC at the University of Chicago. Recent trends in hospital drug spending and manufacturer shortages. Accessed August 13, 2022. https://www.aha.org/system/files/2019-01/aha-drug-pricing-study-report-01152019.pdf
2. US House of Representatives. Drug Pricing Investigation: Majority Staff Report. Accessed August 13, 2022. https://oversight.house.gov/sites/democrats.oversight.house.gov/files/DRUG%20PRICING%20REPORT%20WITH%20APPENDIX%20v3.pdf
3. US Department of Health and Human Services, US Department of the Treasury, US Department of Labor. Reforming America’s healthcare system through choice and competition. Accessed August 13, 2022. https://www.hhs.gov/sites/default/files/Reforming-Americas-Healthcare-System-Through-Choice-and-Competition.pdf
4. Waugh L, McCarthy D. How the Massachusetts Health Policy Commission is fostering a statewide commitment to contain health care spending growth. The Commonwealth Fund. Published March 5, 2020. Accessed September 12, 2022. https://www.commonwealthfund.org/publications/case-study/2020/mar/massachusetts-health-policy-commission-spending-growth
5. Angelis A, Kanavos P, Phillips LD. ICER value framework 2020 update: recommendations on the aggregation of benefits and contextual considerations. Value Health. 2020;23(8):1040-1048. doi: 10.1016/j.jval.2020.04.1828.
6. Shahriar AA, Vazquez Benitez G, Pawloski PA, Dehmer SP, Alpern JD. Characteristics of state legislation addressing prescription drug price increases in the United States, 2020. J Gen Inter Med. 2022;37(6):1554-1557. doi:10.1007/s11606-021-06838-x
7. Brogan AP, Hogue SL, Vekaria RM, Reynolds I, Coukell A. Understanding payer perspectives on value in the use of pharmaceuticals in the United States. J Manag Care Spec Pharm. 2019;25(12):1319-1327. doi: 10.18553/jmcp.2019.25.12.1319
8. Roberts MH, Ferguson GT. Real-world evidence: bridging gaps in evidence to guide payer decisions. Pharmacoecon Open. 2021;5(1):3-11. doi: 10.1007/s41669-020-00221-y
9. Frieden TR. Evidence for health decision making — beyond randomized, controlled trials. N Eng J Med. 2017;377(5):465-475. doi:10.1056/NEJMra1614394
10. Bothwell LE, Greene JA, Podolsky SH, Jones DS. Assessing the gold standard—lessons from the history of RCTs. N Engl J Med. 2016;374(22):2175-2181. doi: 10.1056/NEJMms1604593
11. Briggs AH, Weinstein MC, Fenwick EA, et al; ISPOR-SMDM Modeling Good Research Practices Task Force. Model parameter estimation and uncertainty: a report of the ISPOR-SMDM Modeling Good Research Practices Task Force-6. Med Decis Making. 2012;32(5):722-732. doi: 10.1177/0272989X12458348
12. Holtorf A-P, Brixner D, Bellows B, Keskinaslan A, Dye J, Oderda G. Current and future use of HEOR data in healthcare decision-making in the United States and in emerging markets. Am Health Drug Benefits. 2012;5(7):428-38.
13. Solà-Morales O, Volmer T, Mantovani L. Perspectives to mitigate payer uncertainty in health technology assessment of novel oncology drugs. J Mark Access Health Policy. 2019;7(1):1562861. doi:10.1080/20016689.2018.1562861
14. Malone DC, Brown M, Hurwitz JT, Peters L, Graff JS. Real-world evidence: useful in the real world of US payer decision making? How? When? And what studies? Value Health. 2018;21(3):326-333. doi: 10.1016/j.jval.2017.08.3013
15. Concato J, ElZarrad MK. FDA issues draft guidances on real-world evidence, prepare to publish more in future. Accessed August 13, 2022. https://www.fda.gov/drugs/news-events-human-drugs/fda-issues-draft-guidances-real-world-evidence-prepares-publish-more-future
16. Cohen DJ, Reynolds MR. Interpreting the results of cost-effectiveness studies. J Am Coll Cardiol. 2008;52(25):2119-2126. doi:10.1016/j.jacc.2008.09.018
17. Young KC, Kelly AG, Holloway RG. Reading a cost-effectiveness or decision analysis study: Five things to consider. Neurol Clin Pract. 2013;3(5):413-420. doi:10.1212/CPJ.0b013e3182a78fd8
18. Yan A, Loos A. ICER’s growing influence on payer decision making: the impact of ICER assessments on market dynamics and patient access. HTA Quarterly. 2020;(Winter)
19. ICON. ICER’s impact on payer decision making. Accessed August 13, 2022. https://www.iconplc.com/insights/value-based-healthcare/icers-impact-on-payer-decision-making/
20. Deverka PA, Douglas MP, Phillips KA. Use of real-world evidence in US payer coverage decision-making for next-generation sequencing-based tests: challenges, opportunities, and potential solutions. Value Health. 2020;23(5):540-550. doi:10.1016/j.jval.2020.02.001



