

The Economic Impact of Treatment Sequences for Chronic Lymphocytic Leukemia in the United States: A Cost of Care and Budget Impact Model of Venetoclax Plus Obinutuzumab Sequences
J Clin Pathways. 2022;8(5):36-46. doi:10.25270/jcp.2022.06.1
Corrected November 1, 2023.
Abstract: We estimated the total cumulative costs per patient of treatment sequences for adults with chronic lymphocytic leukemia (CLL), with and without deletion 17p, as well as the budget impact of introducing sequences with first-line (1L) venetoclax + obinutuzumab (V+O) from a US payer perspective. Efficacy, treatment-related costs, and epidemiological inputs were informed by clinical trial publications and public data sources. Cumulative costs per patient (2020 US $) were estimated over 10 years. The results indicated that among adults with CLL with deletion 17p, the 10-year cumulative costs of sequences starting with fixed-duration V+O were lower ($935,781-$1,345,96) than those starting with ibrutinib or acalabrutinib ($1,426,924-$1,906,544); similar results were estimated in adults without deletion 17p (V+O: $690,346- $951,633; ibrutinib or acalabrutinib: $1,720,745-$1,976,767). Retreatment with a venetoclax-based regimen after 1L also resulted in treatment sequences with low costs. In a hypothetical 1-million-member health plan, the total budget impact of introducing sequences with 1L fixed-duration V+O led to cost savings of $12.5 and $56.4 million over 5 and 10 years, respectively.
Introduction
Chronic lymphocytic leukemia (CLL) is the most common type of leukemia among adults across Western nations1-3 and accounts for approximately one-quarter of new leukemia cases in the United States.4 In 2021, there were an estimated 21,250 new cases of CLL and 4320 estimated deaths from CLL in the United States.5 In 2018, there were an estimated 195,129 people living with CLL in the United States.5 CLL is more commonly diagnosed in older adults, with the median age of diagnosis at 70 years.4,5 CLL has a long disease course, with historical 5-and 10-year survival rates of 82.4% and 64.7%, respectively in the United States, with potential improvement in these numbers going forward in the setting of recent improvements in therapy.6
CLL is a heterogeneous disease and some patients harbor mutations which impact their response to therapy and subsequent clinical outcomes.7,8 Specifically, chromosome deletion 17p (5%-8% of patients) and mutations of the TP53 gene (5% in previously untreated to 37% in relapsed/refractory patients) are high-risk features in CLL because they negatively impact treatment response and confer a poor prognosis with historical therapies (ie, chemoimmunotherapy, purine analogues, and alkylating agents).8,9 Recently, therapies such as B-cell receptor pathway inhibitors including idelalisib and ibrutinib in 2014, duvelisib in 2018, and acalabrutinib in 201910-13 have improved outcomes substantially for these patients.14,15
Another highly effective new therapy for CLL, including those with high-risk disease, is venetoclax, a selective oral small-molecule inhibitor of B-cell leukemia/lymphoma-2 (BCL-2) that primes CLL cells for apoptosis.16 In 2016, venetoclax monotherapy was approved by the US Food and Drug Administration (FDA) for adults with relapsed or refractory (R/R) CLL with deletion 17p, based on the positive results of 2 open-label, multicenter, phase 2 clinical studies, M13-982 and M14-032.17-20 In a subsequent phase 3 trial (MURANO) of adults with R/R CLL, comparing fixed-duration venetoclax plus rituximab (V+R) to bendamustine plus rituximab (B+R), those receiving V+R had higher rates of 2-year progression- free survival (PFS) compared to B+R (84.9% vs 36.3%).21 The survival benefit was sustained across all clinical and biologic subgroups, including those with deletion 17p.21 Based on the MURANO trial’s results, V+R received FDA approval in 2018 for adults with R/R CLL, with or without deletion 17p. In 2019, the approval of venetoclax in CLL was expanded to previously untreated patients based on the results of the CLL14 trial,22 in which venetoclax was administered in combination with obinutuzumab (V+O) for 12 months. The trial reported 3-year PFS rates of 81.9% (95% CI: 76.5% to 87.3%) in the V+O group compared to 49.5% (42.4% to 56.6%) in the chlorambucil plus obinutuzumab (C+O) group, and the benefit was maintained in patients with TP53 deletion, 17p mutation, or both, as well as in patients with unmutated immunoglobulin heavy-chain genes, although these higher risk groups did have shorter PFS with V+O than patients with lower risk disease.22,23 More recently reported long-term follow up results from both MURANO and CLL14 trials have also demonstrated that sustained PFS benefit with venetoclax-based regimens was achieved at 3 years off treatment.24,25
Recent studies have reported that oral targeted therapies for CLL may be associated with considerable economic burden when used continuously.26,27 For example, a cost-effectiveness analysis by Patel et al found that the use of first-line ibrutinib was not cost-effective in older adults with CLL in the United States.28 In contrast, time-limited therapies may be more cost-effective. For example, a budget impact analysis by Cho et al, conducted from a US payer’s perspective, reported that the total costs savings of introducing first-line fixed-duration V+O to a 1-million-member health plan was $1.5 million over 3 years compared with a scenario without it.29 The study included chemoimmunotherapy regimens and ibrutinib with or without an anti-CD20 monoclonal antibody.
The increased availability of oral targeted therapies (time- limited or continuous) has transformed the treatment paradigm in CLL, offering several effective treatment options in various lines of therapy, but there is a paucity of literature pertaining to the economic impact of different treatment sequencing. Since its FDA approval in 2019, the budget impact of 12-month fixed duration V+O as first-line treatment for CLL in the US was found to be cost saving;29 however, the long-term costs and budget impact of full treatment sequences beginning with V+O (ie, first-line) have not been investigated. To address this knowledge gap, this study was designed to estimate the total cumulative costs per patient of treatment sequences for adults with CLL, with and without deletion 17p over 10 years. In addition, this study evaluates the budget impact of introducing sequences with V+O as first-line therapy for CLL from a US payer perspective, based on the estimated costs of treatment sequences.
Methods
Model overview
A cost calculator and budget impact model were developed in Excel 2016 (Microsoft, Redmond, WA) to estimate the costs of treatment sequences for CLL and the budget impact com- paring scenarios with and without first-line V+O from a US payer’s perspective over 10 years. A 10-year time horizon was used to comprehensively capture the long-term costs of treat- ment sequences and to appropriately reflect the disease course of CLL. The target population included previously untreated adult patients with CLL; those with and without deletion 17p were modeled separately to account for different treatment sequence options in the 2 populations. Patients received first-line treatment in the first year and were distributed into 5 health states, namely, first line, second line, third line, later line (ie, best supportive care), and death, in subsequent years based on progression and survival data from clinical trials (Figure 1). 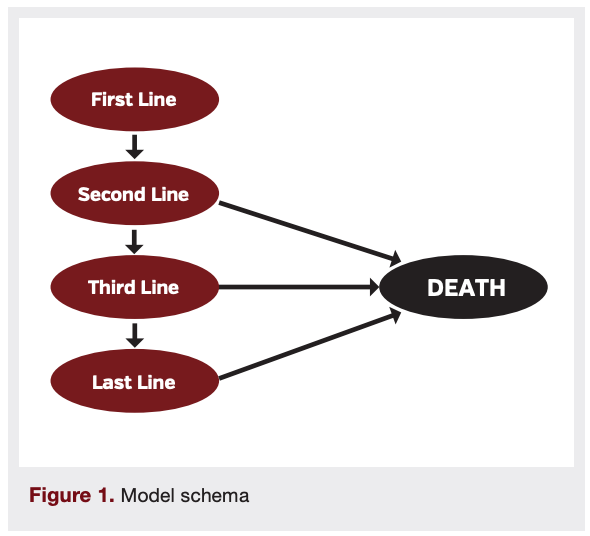 A total of 249 unique treatment sequences (159 for the population with deletion 17p; 204 for the population without deletion 17p) used in clinical practice in the United States were included based on expert clinical opinion.30 Among the included treatment sequences, venetoclax-based therapies could be used in the first line and as retreatment in the second or third line.
A total of 249 unique treatment sequences (159 for the population with deletion 17p; 204 for the population without deletion 17p) used in clinical practice in the United States were included based on expert clinical opinion.30 Among the included treatment sequences, venetoclax-based therapies could be used in the first line and as retreatment in the second or third line.
Model inputs
Efficacy and cost inputs were used in the cumulative cost calculations. For the budget impact analysis, epidemiology inputs were used to estimate the target population and market share inputs were used to reflect the mix of different treatment sequences.
Efficacy
The proportion of patients in each health state were estimated based on PFS and overall survival (OS) data from published clinical trials for both patients with and without deletion 17p.17,31-41 When multiple data sources were available, pivotal trials with larger sample sizes and more consistent trial settings were prioritized. Due to the paucity of long-term data, median survival or landmark survival rates observed in the clinical trials were extrapolated to the modeled time horizon, assuming constant annual rates of progression and death. Due to limited data in the second- and third-line settings separately, efficacy data for the overall R/R setting was used for second-line therapies and a hazard ratio (HR) estimated based on real-world data (CLL Collaborative Study of Real World Evidence [CORE] analysis)42 was applied to the corresponding second-line data, to reflect the faster progression from the third-line health state (HR=1.17).
Costs
Cost components considered in the model included treatment and administration costs, monitoring costs, terminal care costs, tumor lysis syndrome (TLS) prophylaxis costs for venetoclax-based therapies, and costs associated with adverse events (AEs). Costs were estimated as a weighted average of commercial and Medicare costs based on the proportions of patients covered by each plan in the target population for the budget impact model, where applicable. All costs prior to 2020 were inflated to 2020 US dollars (USD) using the Consumer Price Index Medical Care Component (All Urban Consumers).43
Treatment costs
Annual treatment acquisition costs were estimated based on unit drug prices from IBM Micromedex RED BOOK44 and the dosing schedules from the US Prescribing Information (USPI) or clinical trials. Drug administration costs were estimated for intravenous (IV) drugs, derived from MarketScan routine cost of care analysis (data on file, AbbVie). Drug wastage due to potential discrepancies between vial size and actual dosage required was considered in the model for IV drugs. Annual costs in the first and subsequent years were different for therapies with a fixed-duration or ramp-up periods (Table 1).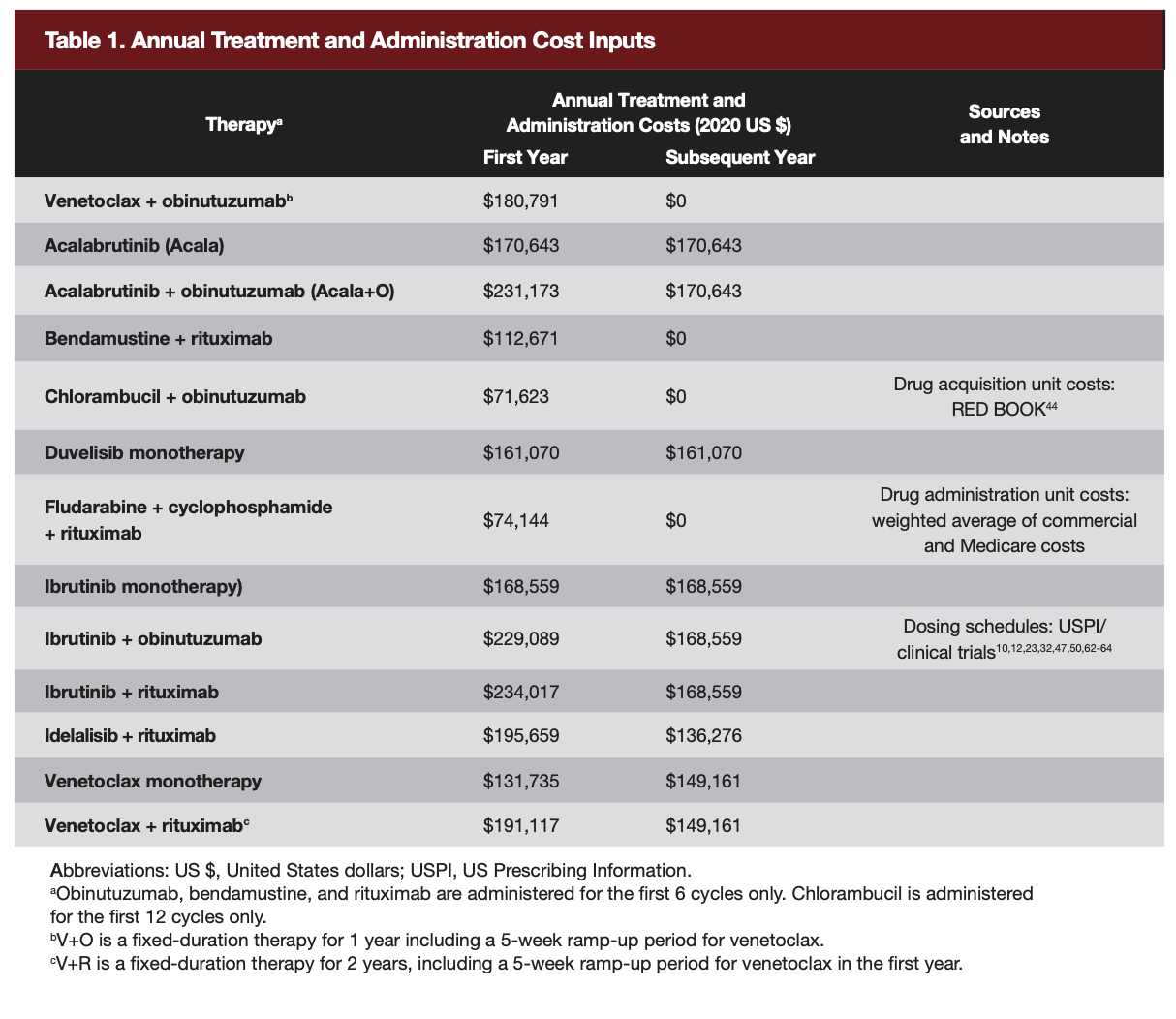
Monitoring and terminal care costs
Annual monitoring costs were applied to all patients alive in each year and included both treatment-specific costs and all-cause health care costs. Treatment-specific costs were applied according to the type of treatment (ie, chemoimmunotherapy or oral targeted therapy). All-cause health care costs included costs for hospitalizations; outpatient visits (home health, skilled nursing facility, office visits, ambulatory surgery center services, and other outpatient services); emergency department visits; durable medical equipment; and pharmacy fills. Annual monitoring costs totaled $37,098 for chemoimmunotherapies (including B+R, C+O, and fludarabine, cyclophosphamide and rituximab) and $37,221 for oral targeted therapies (all other therapies included in the model), based on published data.27,45
Three months of palliative care and a one-month hospital/hospice stay were assumed for terminal care. A one-time terminal care cost of $23,093, based on Sorensen et al,46 was applied in the model at the time when patients entered the death state.
TLS prophylaxis costs
A one-time TLS prophylaxis cost of $17,627 was applied for venetoclax-based regimens at the time of initiating therapy. This cost was calculated based on the USPI for venetoclax; the estimated unit costs of TLS prophylaxis for low-, moderate-, and high-risk patients; the proportion of patients in each risk level based on CLL14; and expert clinical opinion.23,47 Cost components for TLS prophylaxis included inpatient visits, outpatient visits, nurse visits, medical tests (eg, renal function panel, uric acid test), medications (eg, allopurinol and rasburicase), and computed tomography (CT) scans.
AE-related costs
Grade 3/4 AEs reported in at least 5% of patients for at least one of the comparator treatments in each line were assumed to incur a one-time cost at the time of initiating the therapy (ie, year 1 for first-line therapies and year 2 to year 10 for second- and third-line therapies). For second- and third-line therapies, AE rates were obtained from clinical trials of patients with R/R CLL and unit costs for managing individual AEs were obtained from the Agency for Healthcare Research and Quality’s Healthcare Cost and Utilization Project (HCUP).17,21,32,34,37,38,40,41,47-53
Epidemiology
In the budget impact analysis, a hypothetical cohort of 1 million individuals was assumed for the total health plan (80.0% covered by commercial health care insurance and 20% covered by Medicare, based on the Kaiser Family Foundation).54 The target population was determined based on published epidemiologic inputs; the incidence rates of CLL in patients aged 18 to 64 years (commercial) and patients aged ≥65 years (Medicare) were 0.0030% and 0.0275%, respectively, based on Surveillance, Epidemiology, and End Results Program (SEER) statistics and the US Census Bureau.55,56 Among these patients with CLL, 55% were assumed to be receiving drug treatment when entering the model. The proportion of treated patients with deletion 17p was 6.7%, based on Seymour et al.57
Market share
To estimate the market share of each treatment sequence with and without first-line V+O across 10 years, the market shares of first-line therapies were multiplied by the distribution of treatment sequences following each first-line therapy. Specifically, market share data of first-line therapies with and without first-line V+O were estimated based on market share forecasting (data on file, AbbVie); the distribution of treatment sequences following each first-line therapy from year 1 to year 10 were estimated based on discussions with 2 clinical experts.
Results
Estimated 10-year cumulative costs of treatment sequences
Costs of sequences by first-line therapy
Treatment sequences for CLL starting with fixed-duration V+O resulted in considerably lower cumulative 10-year costs compared with sequences starting with other novel agents (eg, I mono, Acala) administered until disease progression (Table 2). Cumulative cost savings were estimated for first-line V+O sequences compared to I mono or Acala sequences among patients with or without deletion 17p.
Among patients with deletion 17p, the cumulative 10-year costs per patient of sequences starting with V+O ranged from $935,781 to $1,345,961; sequences starting with I mono or Acala ranged from $1,426,924 to $1,906,544 in this population. The difference in cumulative costs between the most costly first-line V+O sequence (V+O –> Acala –> Ide+R) and the least costly first-line Acala sequence (Acala –> V+O –> D mono) was $80,963, equivalent to a 6.0% difference in costs (of the V+O sequence), favoring the first-line V+O sequence as the less costly option. The cost difference was mainly attributed to treatment costs (108.8%) and terminal care costs (0.6%), while other costs were slightly higher in the V+O sequence. Conversely, the difference between the least costly first-line V+O sequence (V+O –> Ide+R –> V+R) and the costliest first-line I mono sequence (I mono –> Acala –> V mono) was $970,763, equivalent to a 50.9% difference in costs.
Among patients without deletion 17p, the cumulative costs per patient of sequences starting with V+O ranged from $690,346 to $951,633; sequences starting with I mono and Acala ranged from $1,720,745 to $1,976,767, and $1,742,308 to $1,900,689, respectively. For these patients, the difference in cumulative costs between the most costly first-line V+O sequence (V+O –> Acala –> Ide+R) and the least costly first-line I mono sequence (I mono ∀ V+O ∀ V+R) was $769,112, equivalent to a 44.7% difference in costs, favoring the first-line V+O sequence as the less costly option. Conversely, the difference between the least costly first-line V+O sequence (V+O –> B+R –> V+R) and the most costly first-line I mono sequence (I mono –> Acala –> V mono) was $1,286,421, equivalent to a 65.1% difference in costs. With a similar trend, the difference in cumulative costs between first-line V+O sequences and first-line Acala sequences ranged from $790,675 to $1,210,343, favoring the first-line V+O sequence as the less costly option. Similar to patients with deletion 17p, substantial cost savings were also estimated when using sequences with first-line V+O compared with those with first-line Acala (Table 2).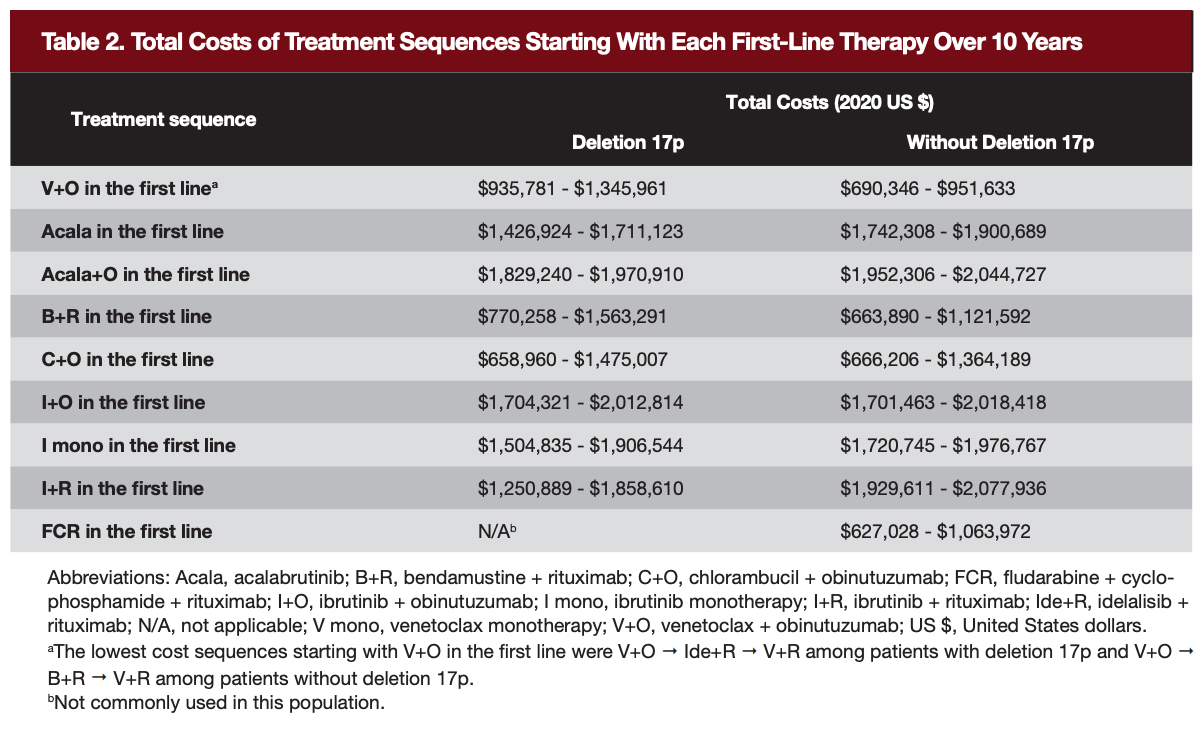
Costs of the most used sequences
Five of the most commonly used sequences in each population were selected based on the market share data over ten years in the scenario with V+O. Among patients with deletion 17p (Figure 2), V+O –> Acala –> Ide+R was the most commonly used sequence; it was estimated to incur the lowest cumulative costs per patient over 10 years when compared with 4 other commonly used sequences ($1,345,961 vs $1,714,123 to $1,906,544). V+O –> Acala –> Ide+R resulted in cost savings of $550,678 over 10 years, or a 29.0% difference in costs per patient when compared with the most commonly used sequence (I mono –> AcalaV+R).
Similarly, among patients without deletion 17p (Figure 2), 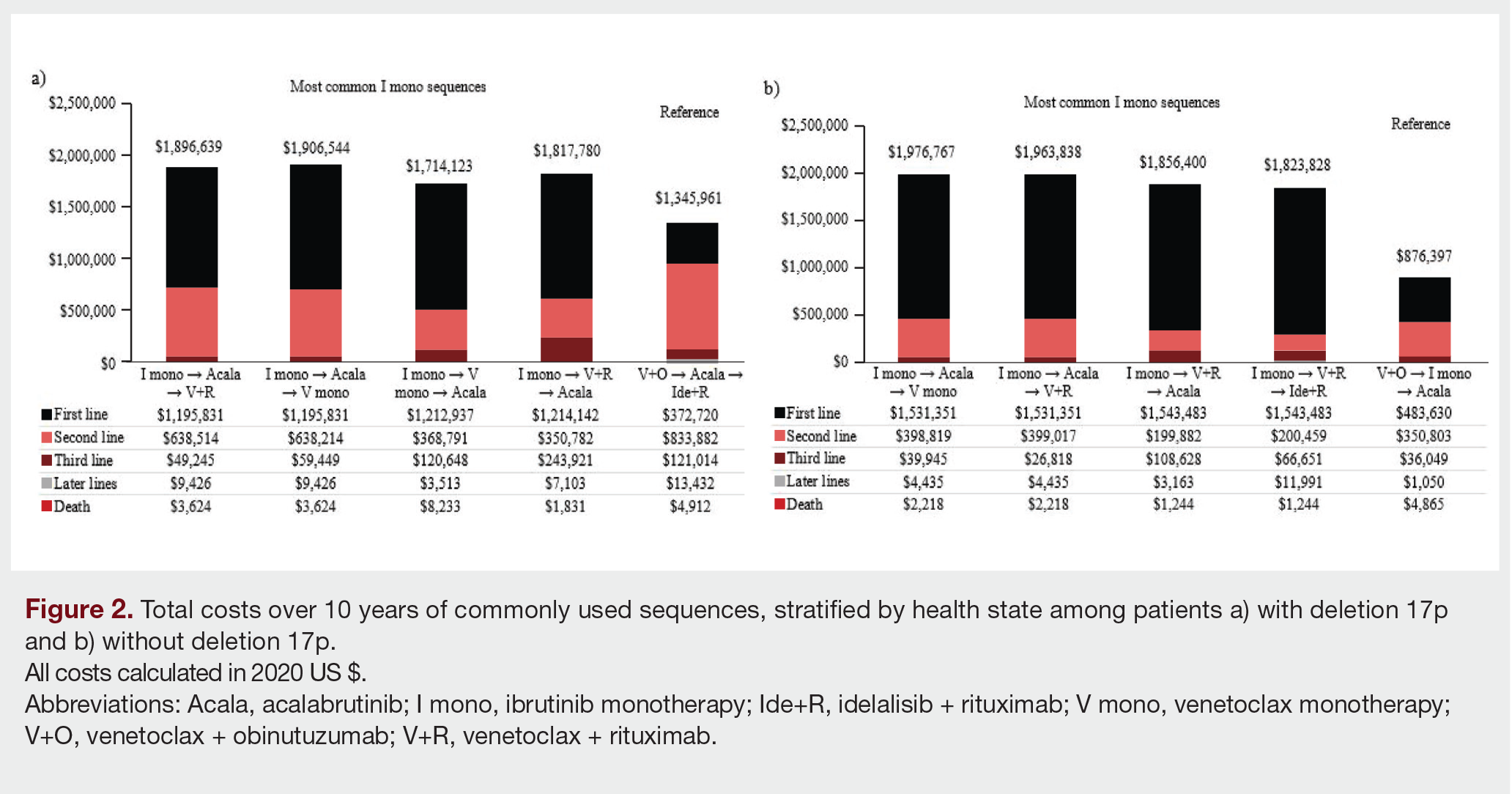 the most commonly used sequence starting with V+O (V+O–>I mono –> Acala) was associated with the lowest cumulative costs per patient over 10 years, compared with 4 other commonly used sequences starting with I mono ($876,397 vs. $1,823,828 to $1,976,767). Compared to the most commonly used sequence which was also the most costly sequence starting with I mono in this population (I mono –> Acala –> V mono), the sequence V+O–> I mono –> Acala was estimated to result in cost savings of $1,100,370 over 10 years, a 55.7% difference in costs per patient.
the most commonly used sequence starting with V+O (V+O–>I mono –> Acala) was associated with the lowest cumulative costs per patient over 10 years, compared with 4 other commonly used sequences starting with I mono ($876,397 vs. $1,823,828 to $1,976,767). Compared to the most commonly used sequence which was also the most costly sequence starting with I mono in this population (I mono –> Acala –> V mono), the sequence V+O–> I mono –> Acala was estimated to result in cost savings of $1,100,370 over 10 years, a 55.7% difference in costs per patient.
In both populations, cumulative costs of treatment sequences were largely determined by the therapies used in the first 2 lines (black and pink portions in Figure 3a [with deletion 17p] and Figure 3b [without deletion 17p]).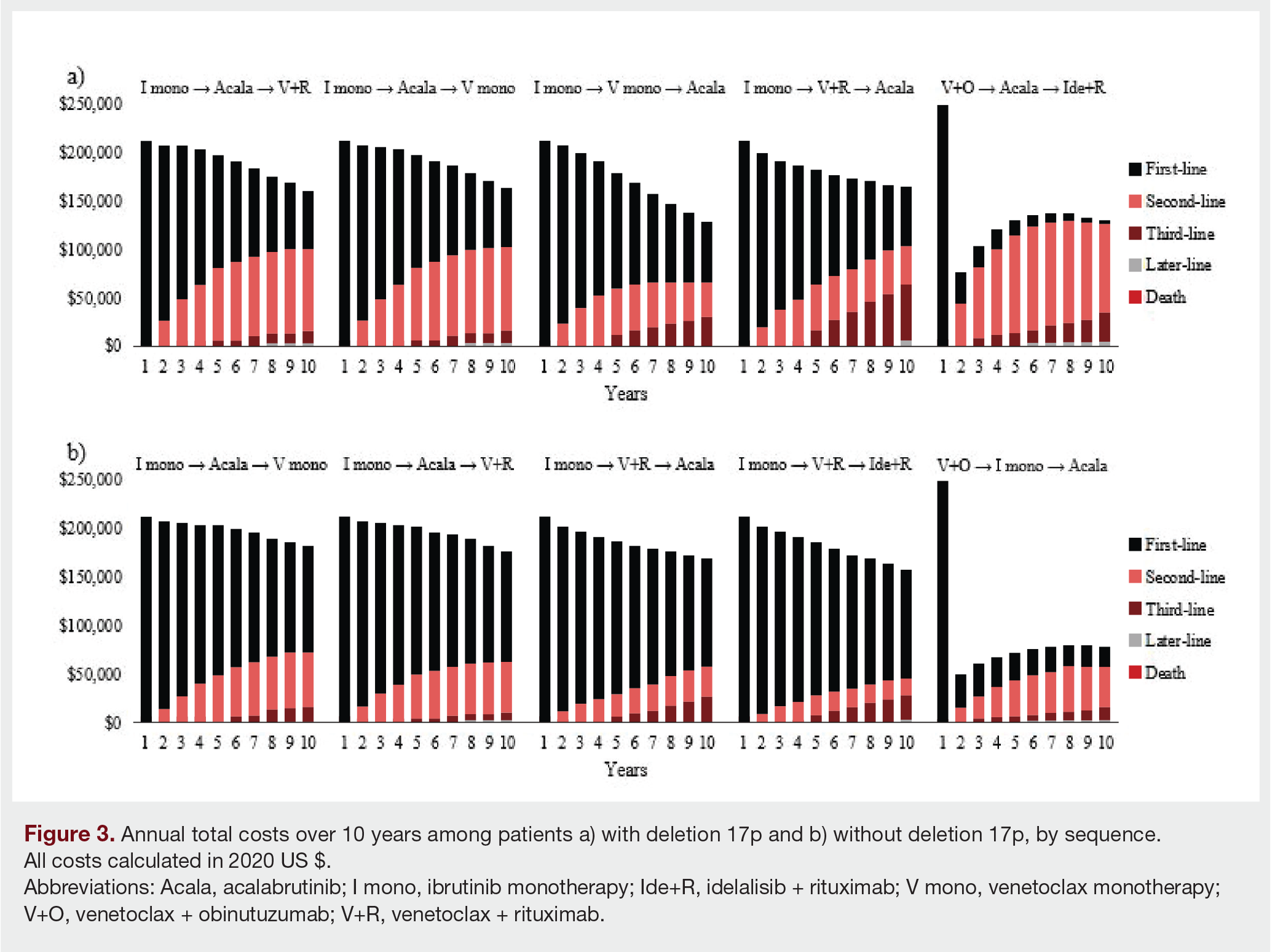 In both populations, sequences starting with V+O were estimated to result in considerably lower costs beginning at year 2 compared with sequences starting with I mono in both populations, resulting in lower cumulative costs across the 10-year horizon. A similar comparative trend was observed for V+O sequences compared with sequences starting with Acala.
In both populations, sequences starting with V+O were estimated to result in considerably lower costs beginning at year 2 compared with sequences starting with I mono in both populations, resulting in lower cumulative costs across the 10-year horizon. A similar comparative trend was observed for V+O sequences compared with sequences starting with Acala.
Costs of different first-line V+O sequences
Table 3 lists the estimated costs associated with treatment sequences beginning with V+O among patients with or without deletion 17p. In the R/R setting, the model indicated that sequences including retreatment with venetoclax-based regimens (ie, V+R or V mono) can also lead to cost savings. Among sequences starting with V+O, retreatment with a venetoclax-based regimen in second line often resulted in relatively lower cumulative costs in patients without deletion 17p, ranging from $759,633 to $913,474 compared with V+O sequences with acalabrutinib in second line, ranging from $927,401 to $951,633 (Table 3). 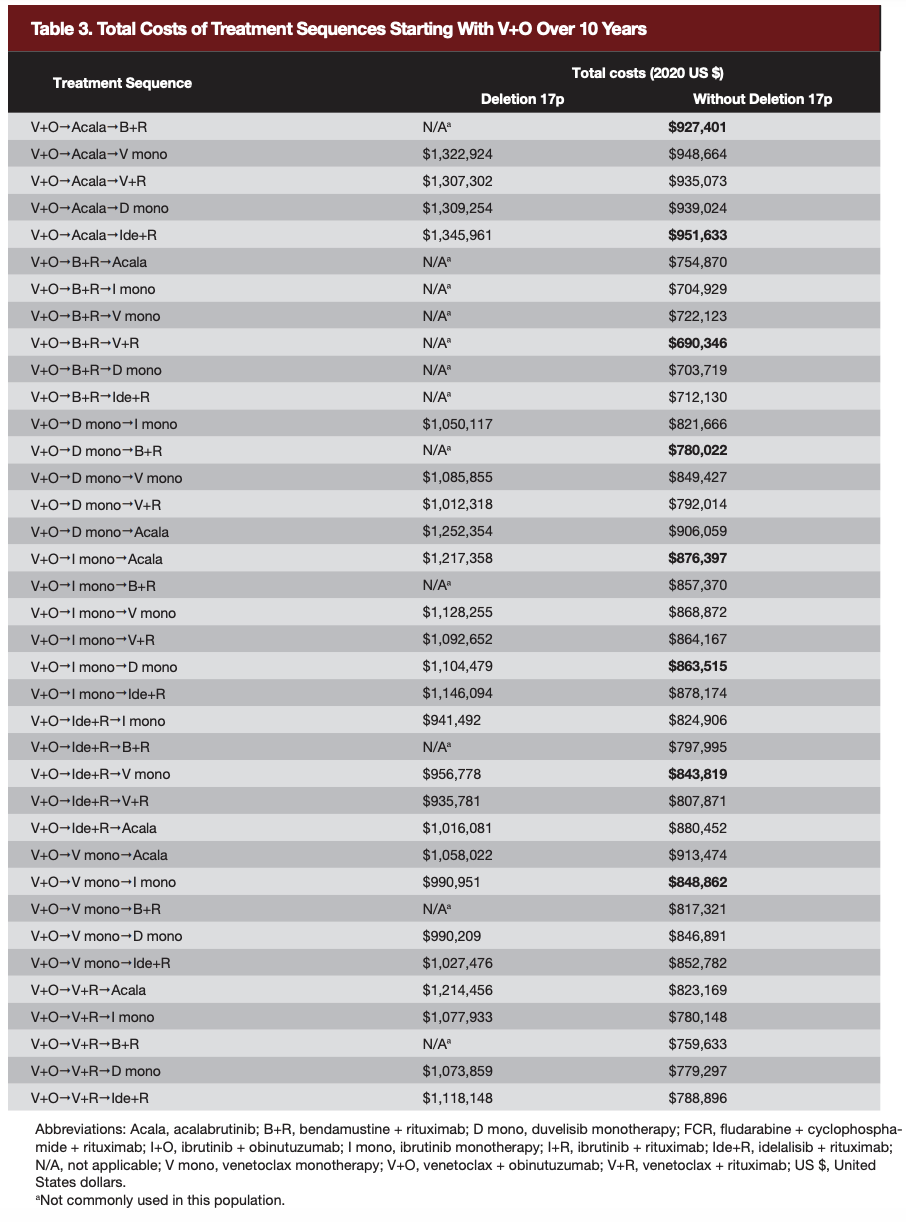 Similarly, in patients with deletion 17p, retreatment using venetoclax-based therapies in second line also often led to cost savings compared with using other novel therapies in second line in the model. For example, the average 10-year cumulative costs per patient of sequences with first-line V+O and second-line V mono were $1,016,664, while the average costs of sequences using I mono or Acala in second line following V+O were $1,137,767 and $1,321,360, respectively.
Similarly, in patients with deletion 17p, retreatment using venetoclax-based therapies in second line also often led to cost savings compared with using other novel therapies in second line in the model. For example, the average 10-year cumulative costs per patient of sequences with first-line V+O and second-line V mono were $1,016,664, while the average costs of sequences using I mono or Acala in second line following V+O were $1,137,767 and $1,321,360, respectively.
Budget Impact
In a hypothetical health plan with 1 million members, the model estimated that 3 with CLL with deletion 17p and 41 without deletion 17p would be eligible for treatment sequences starting with V+O each year. From a US payer’s perspective, the 5- and 10-year total budget impacts were estimated at $121,568,391 and $428,864,524, respectively, in patients with deletion 17p and $109,068,039 and $372,419,081 in patients without deletion 17p (Figure 4).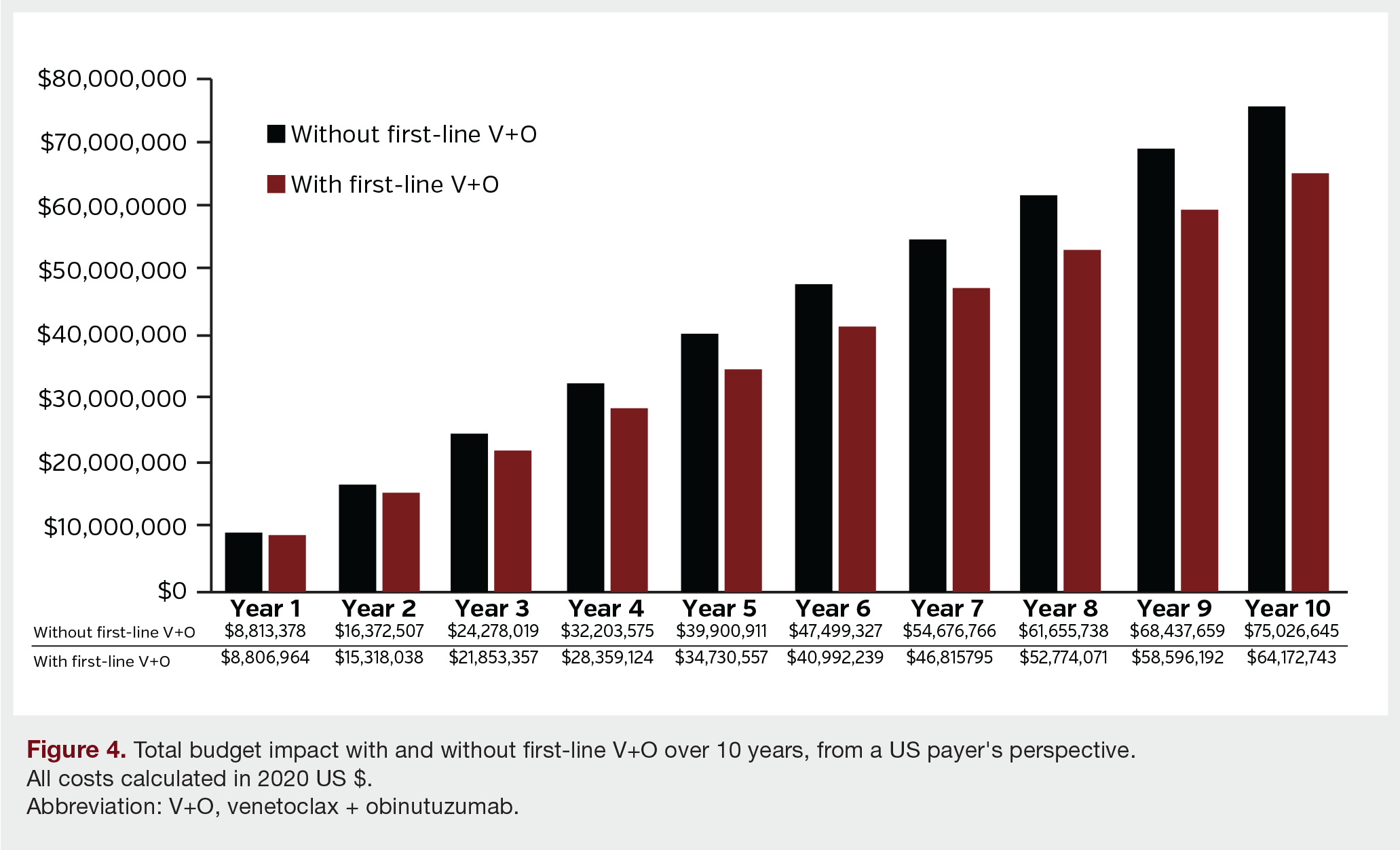 For the overall population, the total budget decreased across 10 years in the scenario with first-line V+O compared to the scenario without first-line V+O (Figure 4). The model estimated that the total budget impact of introducing sequences with first-line V+O led to cost savings of $12.5 million and $56.4 million over 5 and 10 years, respectively, for a US health plan of 1 million members (Figure 5). These costs savings were driven by substantially lower treatment costs in years 2 to 10 (savings of $53,796,012), lower AE-related costs across all years (savings of $4,155,857), and lower monitoring costs in years 7 to 10 (savings of $120,068).
For the overall population, the total budget decreased across 10 years in the scenario with first-line V+O compared to the scenario without first-line V+O (Figure 4). The model estimated that the total budget impact of introducing sequences with first-line V+O led to cost savings of $12.5 million and $56.4 million over 5 and 10 years, respectively, for a US health plan of 1 million members (Figure 5). These costs savings were driven by substantially lower treatment costs in years 2 to 10 (savings of $53,796,012), lower AE-related costs across all years (savings of $4,155,857), and lower monitoring costs in years 7 to 10 (savings of $120,068).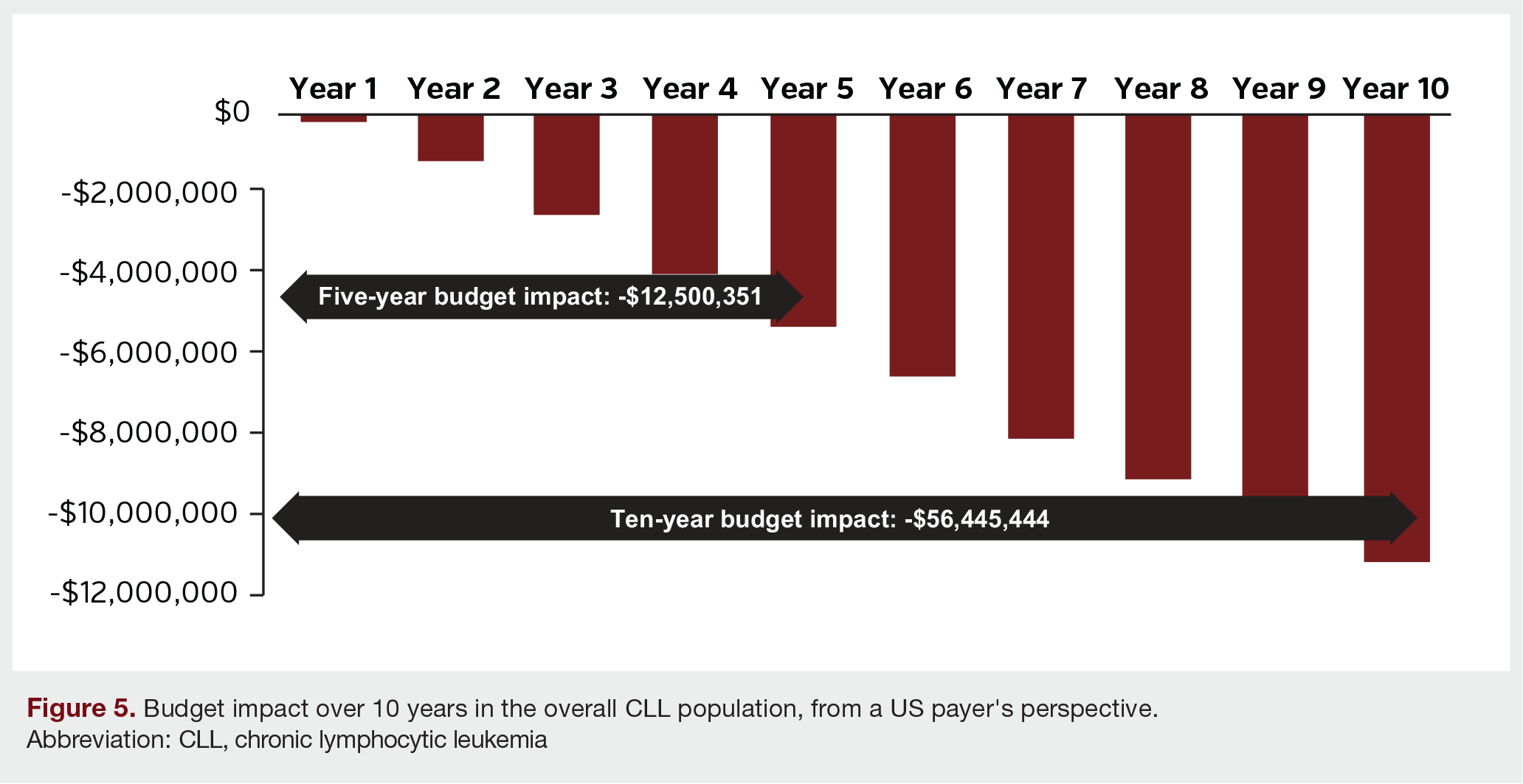
Discussion
The FDA has approved 6 new drugs and combinations for CLL since 2013, resulting in 720 unique potential sequences of novel therapies. As the treatment landscape for CLL rapidly evolves with the emergence of new drug agents, both clinicians and patients with CLL are presented with a significantly wider range of viable treatment options. Thus, understanding optimal treatment sequencing has become increasingly important in the management of CLL. The rapidly evolving treatment landscape is accounted for in the model’s market share estimates. For example, the declining use of sequences with B+R over time is reflected by a reduction in market shares of B+R sequences over the modelled 10-year time horizon. To that end, this cost of care and budget impact model estimated the economic impact of various treatment sequences for CLL among patients with and without the high-risk deletion 17p from a US payer’s perspective.
In our model, treatment sequences starting with V+O for a fixed duration resulted in considerably lower cumulative costs compared with sequences starting with other novel agents administered until disease progression (ie, ibrutinib, acalabrutinib) in both patient populations (with and without deletion 17p). In addition, among sequences starting with V+O in first-line, retreatment with a venetoclax-based regimen in second line was estimated to result in additional cost savings in many instances. Overall, the total budget impact of introducing sequences with V+O in the first-line is expected to be cost saving to US payers over 5- and 10-year horizons, primarily due to lower treatment costs in years 2 to 10 for sequences starting with 12-month fixed-duration V+O.
To our knowledge, our model is the first to evaluate the economic impact of almost 250 different sequences for patients with CLL, both with and without deletion 17p, in the United States. Our findings indicate that sequences starting with novel agents with a fixed duration of treatment, such as V+O, offer a more favorable economic profile compared with other novel agents administered until progression, such as ibrutinib and acalabrutinib. When seeking to understand optimal treatment sequences in clinical practice, efficacy, cost-effectiveness, and the impact to health systems should all be considered. The economic impact of the vast range of possible sequences in the US has not been deeply investigated, although a few studies have investigated optimal sequencing for CLL in clinical outcomes. Such studies can be challenging due to ethical concerns regarding randomization, the challenge regarding the number of potential sequences, and administrative barriers.58,59 A large multicenter retrospective study in the United States by Mato et al evaluated patient outcomes associated with CLL treatment sequences, including ibrutinib, idelalisib, and venetoclax, among 683 patients.59 The results suggested that ibrutinib appeared superior to idelalisib in the first line in overall response rates and PFS and, in the setting of kinase inhibitor failure, venetoclax appeared superior to chemoimmunotherapy combinations. Another retrospective study indicated that the incorporation of novel targeted therapies may generate deeper clinical responses and prolonged remission.58 In a comparative analysis by Eyre et al of patients with CLL who received either ibrutinib or venetoclax with or without a CD20-targeting agent as the first novel therapy after relapse, venetoclax was associated with a significantly longer PFS and comparable OS.60 Though novel targeted therapies and sequences were evaluated in several studies, we did not identify any clinical trial that compared treatment sequences starting with different novel targeted therapies in head-to-head comparisons, or studies which comprehensively assessed the economic impact associated with existing novel vs conventional treatment sequences. This study added to the limited evidence and provided data which could inform treatment sequence selection in the ever-evolving treatment landscape. Future clinical trials and real-world studies comparing various treatment sequences are still needed among patients with various risk factors (ie, deletion 17p), especially given the number of new treatment options and those that will continue to emerge.
Furthermore, health care payers and decision makers continue to monitor the treatment landscape and are conscious of the high economic toll and budget impact of oncology treatments, which is of particular relevance to CLL due to its long disease course. Therefore, treatments offering a fixed-treatment duration may offer a more favorable option for CLL compared with other available agents administered until progression. For example, clinicians may not recommend ibrutinib to younger, fitter patients, as this commits a patient to costly continuous treatment which may be also associated with other issues such as ongoing toxicities and development of resistance from daily exposure to a targeted agent.58 In addition, outcomes-based agreements to curtail spending in oncology are not often utilized, as oncology remains a protected class in the United States. According to a recent survey study by Runyan et al, traditional cost management tools were not effective in controlling costs for CLL, and health care payers resorted to innovative tools such as pathways of care.61 However, it may take years for the effects of new tools to be understood following their integration. Runyan et al noted that, compared to seeking pathways of care, optimizing the pathway of treatment administration (ie, treatment sequencing) may be a more effective way to control CLL costs, and the cost savings became evident after 2 years.61 In our model, the introduction of sequences with V+O in the first line resulted in cost savings of $942,261 after 2 years and there were even more cost savings from years 2 to 10. Thus, considering the total costs across treatment lines may lead to costs savings over the entire duration of therapy, ultimately lowering the budget impact to health care payers.
The results of this study should be interpreted in the context of several limitations, some of which are inherent to economic modelling. First, efficacy and safety inputs were obtained from various clinical trials and sources based on heterogeneous patient populations and were assumed applicable to the target population based on the best available data. Though heterogeneity in the patient characteristics exists, all data were obtained from a US setting and the quality of the studies (eg, sample size, length of follow up, patient enrolment criteria, and process) were evaluated to provide the most suitable data for our model. Second, long-term effectiveness data in both trial settings and in the real world were not available in the published literature. Therefore, efficacy outcomes observed in clinical studies were extrapolated to 10 years based on assumptions. Though the extrapolated data may not perfectly emulate real-world treatment effectiveness, it provides the best possible understanding of the relative long-term outcomes of different treatment sequences given the available data and allows for useful new information on the relative direction of costs and budget impact (ie, cost saving) in the real-world. Finally, the model assumed no dose reductions or treatment discontinuation due to tolerability issues, with no treatment gaps between progression and initiation of the next line of therapy, assuming patients received at least 2 lines of therapy before death. A balance between the number of assumptions in the model and recapitulating real-world clinical practice was required due to the limited data available in the published literature and the hypothetical nature of economic modelling. However, despite these limitations, our model still provides valuable new information on the relative economic impact of different treatment sequences for CLL in the real world.
In summary, in this budget impact model from a US payer’s perspective, treatment sequences starting with V+O for a fixed duration resulted in considerably lower costs compared with sequences starting with other novel agents administered until disease progression. The cost savings of sequences with first-line V+O were due to substantial reductions in treatment costs associated with the fixed duration of therapy. Furthermore, treatment sequences including retreatment with a venetoclax-based regimen also lead to cost savings. These results were consistent among patients with deletion 17p and those without it. Our study results not only shed light on different treatment sequences in the context of economic savings, but also illustrate the benefit of fixed-treatment duration, further informing treatment decision-making in CLL.
This article has supplementary material, which can be accessed here.
Author Information
Authors: Matthew S Davids MD, MMSC1; Beenish S Manzoor, PhD, MPH2; Nisha C Hazra, PhD, MSc3; Honghao Fang, MSc4; Arliene Ravelo, MPH5; Fang Han4; Annie Guerin, MS6; Kavita Sail, PhD2; Sheila Shapouri, MS5; Mazyar Shadman, MD, MPH7
Affiliations:1Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA; 2AbbVie Inc, North Chicago, IL; 3Analysis Group, Inc, London, United Kingdom; 4Analysis Group, Inc, Beijing, China; 5Genentech, South San Francisco, CA; 6Analysis Group, Inc, Montreal, Canada; 7University of Washington and Fred Hutchinson Cancer Research Center, Seattle, WA
Address Correspondence to:
Beenish Manzoor, PhD MPH
1 North Waukegan Rd. Dept. GMH1, ABV1 - 3NW, North Chicago, IL 60064
Phone: 847-936-6256
Email: beenish.manzoor@abbvie.com
Funding: This study was funded by AbbVie, Inc and Genentech.
Acknowledgements: Medical writing was provided by Shelley Batts, PhD, an employee of Analysis Group, Inc.
Corrections: This article was corrected November 1, 2023, to fix errors with the figure titles and legends for Figures 2-5; missing citations to two supplementary tables from the final article; missing supplementary material from the online version; a misspelling of the corresponding author’s first name; and minor typographical errors.
References
1. van den Broek EC, Kater AP, van de Schans SA, et al. Chronic lymphocytic leukaemia in the Netherlands: trends in incidence, treatment and survival, 1989-2008. Eur J Cancer. 2012;48(6):889-895. doi:10.1016/j.ejca.2011.06.053.
2. Brenner H, Gondos A, Pulte D. Trends in long-term survival of patients with chronic lymphocytic leukemia from the 1980s to the early 21st century. Blood. 2008;111(10):4916-4921. doi:10.1182/blood-2007-12-129379
3. Kristinsson SY, Dickman PW, Wilson WH, Caporaso N, Björkholm M, Landgren O. Improved survival in chronic lymphocytic leukemia in the past decade: a population-based study including 11,179 patients diagnosed between 1973-2003 in Sweden. Haematologica. 2009;94(9):1259-1265. doi:10.3324/haematol.2009.007849
4. American Cancer Society. Key statistics for chronic lymphocytic leukemia. 2021; https://www.cancer.org/cancer/chronic-lymphocytic-leukemia/about/key-statistics.html. Accessed July 21, 2021.
5. National Cancer Institute. Cancer Stat Facts: Leukemia — Chronic Lymphocytic Leukemia (CLL). Accessed June 7, 2022; https://seer.cancer.gov/statfacts/html/clyl.html.
6. Pulte D, Castro FA, Jansen L, et al; GEKID Cancer Survival Working Group. Trends in survival of chronic lymphocytic leukemia patients in Germany and the USA in the first decade of the twenty-first century. J Hematol Oncol. 2016;9:28. Published 2016 Mar 22. doi:10.1186/s13045-016-0257-2
7. Brander D, Islam P, Barrientos JC. Tailored treatment strategies for chronic lymphocytic leukemia in a rapidly changing era. American Society of Clinical Oncology educational book American Society of Clinical Oncology Annual Meeting. 2019;39:487-498.
8. Hallek M. Chronic lymphocytic leukemia: 2020 update on diagnosis, risk stratification and treatment. American journal of hematology. 2019;94(11):1266-1287.
9. Zenz T, Häbe S, Denzel T, et al. Detailed analysis of p53 pathway defects in fludarabine-refractory chronic lymphocytic leukemia (CLL): dissecting the contribution of 17p deletion, TP53 mutation, p53-p21 dysfunction, and miR34a in a prospective clinical trial. Blood. 2009;114(13):2589-2597.
10. US Food and Drug Administration. Highlights of prescribing information: ZYDELIG (idelalisib). Accessed June 7, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/205858s014lbl.pdf
11. US Food and Drug Administration. Highlights of prescribing information: IMBRUVICA (ibrutinib). Accessed June 2, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/205552s033,210563s010lbl.pdf
12. US Food and Drug Administration. Highlights of prescribing information: COPIKTRA (duvelisib). Accessed June 7, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/211155s001lbl.pdf
13. US Food and Drug Administration. Highlights of prescribing information: CALQUENCE (acalabrutinib). Accessed June 7, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/210259s006s007lbl.pdf.
14. van der Straten L, Levin MD, Visser O, et al. Survival continues to increase in chronic lymphocytic leukaemia: a population-based analysis among 20 468 patients diagnosed in the Netherlands between 1989 and 2016. Br J Haematol. 2020;189(3):574-577. doi:10.1111/bjh.16397
15. Hallek M. Role and timing of new drugs in CLL. Hematol Oncol. 2017;35 Suppl 1:30-32. doi:10.1002/hon.2397
16. Souers AJ, Leverson JD, Boghaert ER, et al. ABT-199, a potent and selective BCL-2 inhibitor, achieves antitumor activity while sparing platelets. Nat Med. 2013;19(2):202-208. doi:10.1038/nm.3048
17. Stilgenbauer S, Eichhorst B, Schetelig J, et al. Venetoclax for Patients With Chronic Lymphocytic Leukemia With 17p Deletion: Results From the Full Population of a Phase II Pivotal Trial [published correction appears in J Clin Oncol. 2019 Sep 1;37(25):2299]. J Clin Oncol. 2018;36(19):1973-1980. doi:10.1200/JCO.2017.76.6840
18. Stilgenbauer S, Eichhorst B, Schetelig J, et al. Venetoclax in relapsed or refractory chronic lymphocytic leukaemia with 17p deletion: a multicentre, open-label, phase 2 study. Lancet Oncol. 2016;17(6):768-778. doi:10.1016/S1470-2045(16)30019-5
19. Coutre S, Choi M, Furman RR, et al. Venetoclax for patients with chronic lymphocytic leukemia who progressed during or after idelalisib therapy. Blood. 2018;131(15):1704-1711. doi:10.1182/blood-2017-06-788133
20. Jones JA, Mato AR, Wierda WG, et al. Venetoclax for chronic lymphocytic leukaemia progressing after ibrutinib: an interim analysis of a multicentre, open-label, phase 2 trial. Lancet Oncol. 2018;19(1):65-75. doi:10.1016/S1470-2045(17)30909-9
21. Seymour JF, Kipps TJ, Eichhorst B, et al. Venetoclax-Rituximab in Relapsed or Refractory Chronic Lymphocytic Leukemia. N Engl J Med. 2018;378(12):1107-1120. doi:10.1056/NEJMoa1713976
22. Al-Sawaf O, Zhang C, Tandon M, et al. Venetoclax plus obinutuzumab versus chlorambucil plus obinutuzumab for previously untreated chronic lymphocytic leukaemia (CLL14): follow-up results from a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2020;21(9):1188-1200. doi:10.1016/S1470-2045(20)30443-5
23. US Food and Drug Administration. Highlights of prescribing information: VENCLEXTA (venetoclax tablets). Accessed June 7, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/208573s023lbl.pdf
24. Al-Sawaf O, Zhang C, Lu T, et al. Al-Sawaf O, Zhang C, Lu T, et al. Minimal residual disease dynamics after venetoclax-obinutuzumab treatment: extended off-treatment follow-up from the randomized CLL14 study. J Clin Oncol. 2021;39(36):4049-4060. doi:10.1200/JCO.21.01181
25. Kater AP, Kipps TJ, Eichhorst B, et al. Five-year analysis of murano study demonstrates enduring undetectable minimal residual disease (uMRD) in a subset of relapsed/refractory chronic lymphocytic leukemia (R/R CLL) patients (Pts) following fixed-duration venetoclax-rituximab (VenR) therapy (Tx). Blood. 2020;136(Suppl1):19-21. doi:10.1182/blood-2020-136109
26. Lachaine J, Beauchemin C, Guinan K, et al. Impact of oral targeted therapy on the economic burden of chronic lymphocytic leukemia in Canada. Curr Oncol. 2021;28(1):332-345. Published 2021 Jan 9. doi:10.3390/curroncol28010037
27. Chen Q, Jain N, Ayer T, et al. Economic burden of chronic lymphocytic leukemia in the era of oral targeted therapies in the United States. J Clin Oncol. 2017;35(2):166-174. doi:10.1200/JCO.2016.68.2856
28. Patel KK, Isufi I, Kothari S, Davidoff AJ, Gross CP, Huntington SF. Cost-effectiveness of first-line vs third-line ibrutinib in patients with untreated chronic lymphocytic leukemia. Blood. 2020;136(17):1946-1955. doi:10.1182/blood.2020004922
29. Cho SK, Manzoor BS, Sail KR, et al. Budget Impact of 12-Month Fixed Treatment Duration Venetoclax in Combination with Obinutuzumab in Previously Untreated Chronic Lymphocytic Leukemia Patients in the United States. Pharmacoeconomics. 2020;38(9):941-951. doi:10.1007/s40273-020-00919-1
30. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: Chronic lymphocytic leukemia/small lymphocytic lymphoma (v 4.2020). 2019.
31. Sharman JP, Egyed M, Jurczak W, et al. Acalabrutinib with or without obinutuzumab versus chlorambucil and obinutuzmab for treatment-naive chronic lymphocytic leukaemia (ELEVATE TN): a randomised, controlled, phase 3 trial [published correction appears in Lancet. 2020 May 30;395(10238):1694]. Lancet. 2020;395(10232):1278-1291. doi:10.1016/S0140-6736(20)30262-2
32. Woyach JA, Ruppert AS, Heerema NA, et al. Ibrutinib Regimens versus Chemoimmunotherapy in Older Patients with Untreated CLL. N Engl J Med. 2018;379(26):2517-2528. doi:10.1056/NEJMoa1812836
33. Mato AR, Roeker LE, Allan JN, et al. Outcomes of front-line ibrutinib treated CLL patients excluded from landmark clinical trial. Am J Hematol. 2018;93(11):1394-1401. doi:10.1002/ajh.25261
34. Moreno C, Greil R, Demirkan F, et al. Ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab in first-line treatment of chronic lymphocytic leukaemia (iLLUMINATE): a multicentre, randomised, open-label, phase 3 trial [published correction appears in Lancet Oncol. 2019 Jan;20(1):e10]. Lancet Oncol. 2019;20(1):43-56. doi:10.1016/S1470-2045(18)30788-5
35. Cramer P, von Tresckow J, Bahlo J, et al. Bendamustine followed by obinutuzumab and venetoclax in chronic lymphocytic leukaemia (CLL2-BAG): primary endpoint analysis of a multicentre, open-label, phase 2 trial. Lancet Oncol. 2018;19(9):1215-1228. doi:10.1016/S1470-2045(18)30414-5
36. Ghia P, Pluta A, Wach M, et al. Acalabrutinib vs rituximab plus idelalisib (IDR) or bendamustine (BR) by investigator choice in relapsed/refractory (RR) chronic lymphocytic leukemia: Phase 3 ASCEND Study. Hematol Oncol. 2019;37(S2):86-87. doi: 10.1002/hon.54_2629
37. Fischer K, Cramer P, Busch R, et al. Bendamustine combined with rituximab in patients with relapsed and/or refractory chronic lymphocytic leukemia: a multicenter phase II trial of the German Chronic Lymphocytic Leukemia Study Group. J
Clin Oncol. 2011;29(26):3559-3566. doi:10.1200/JCO.2010.33.8061
38. Flinn IW, Hillmen P, Montillo M, et al. The phase 3 DUO trial: duvelisib vs ofatumumab in relapsed and refractory CLL/SLL. Blood. 2018;132(23):2446-2455. doi:10.1182/blood-2018-05-850461
39. O'Brien S, Furman RR, Coutre S, et al. Single-agent ibrutinib in treatment-naïve and relapsed/refractory chronic lymphocytic leukemia: a 5-year experience. Blood. 2018;131(17):1910-1919. doi:10.1182/blood-2017-10-810044
40. Sharman JP, Coutre SE, Furman RR, et al. Final results of a randomized, phase III study of rituximab with or without idelalisib followed by open-label idelalisib in patients with relapsed chronic lymphocytic leukemia. J Clin Oncol. 2019;37(16):1391-1402. doi:10.1200/JCO.18.01460
41. Ghia P, Pluta A, Wach M, et al. ASCEND: phase III, randomized trial of acalabrutinib versus idelalisib plus rituximab or bendamustine plus rituximab in relapsed or refractory chronic lymphocytic leukemia. J Clin Oncol. 2020;38(25):2849-2861. doi:10.1200/JCO.19.03355.
42. Mato AR, Sail K, Yazdy MS, et al. Treatment sequences and outcomes of patients with CLL treated with venetoclax and other novel agents post introduction of novel therapies. Blood. 2019;134(Supplement_1):1756. doi.org/10.1182/blood-2019-124600
43. US Bureau of Labor Statistics. Consumer Price Index - all urban consumers not seasonally adjusted US city average for medical care, 1998-2020. Accessed June 7, 2022. https://data.bls.gov/PDQWeb/cu
44. IBM Micromedex. RED BOOK. Accessed June 7, 2022. https://www.ibm.com/products/micromedex-red-book
45. Wang S, Lafeuille MH, Lefebvre P, Romdhani H, Emond B, Senbetta M. Economic burden of treatment failure in chronic lymphocytic leukemia patients. Curr Med Res Opin. 2018;34(6):1135-1142. doi:10.1080/03007995.2018.1464904
46. Sorensen SV, Goh JW, Pan F, et al. Incidence-based cost-of-illness model for metastatic breast cancer in the United States. Int J Technol Assess Health Care. 2012;28(1):12-21. doi:10.1017/S026646231100064X
47. Fischer K, Al-Sawaf O, Bahlo J, et al. Venetoclax and Obinutuzumab in Patients with CLL and Coexisting Conditions. N Engl J Med. 2019;380(23):2225-2236. doi:10.1056/NEJMoa1815281
48. Agency for Healthcare Research and Quality. HCUPnet. Accessed June 7, 2022. https://hcupnet.ahrq.gov/
49. Barr PM, Robak T, Owen C, et al. Sustained efficacy and detailed clinical follow-up of first-line ibrutinib treatment in older patients with chronic lymphocytic leukemia: extended phase 3 results from RESONATE-2. Haematologica. 2018;103(9):1502-1510. doi:10.3324/haematol.2018.192328
50. Eichhorst B, Fink AM, Bahlo J, et al. First-line chemoimmunotherapy with bendamustine and rituximab versus fludarabine, cyclophosphamide, and rituximab in patients with advanced chronic lymphocytic leukaemia (CLL10): an international, open-label, randomised, phase 3, non-inferiority trial. Lancet Oncol. 2016;17(7):928-942. doi:10.1016/S1470-2045(16)30051-1.
51. Sharman JP, Banerji V, Fogliatto LM, et al. ELEVATE TN: Phase 3 study of acalabrutinib combined with obinutuzumab (O) or alone vs o plus chlorambucil (Clb) in patients (Pts) with treatment-naive chronic lymphocytic leukemia (CLL). Blood. 2019;Nov 13(134). doi:10.1182/blood-2019-128404
52. Flinn IW, Gribben JG, Dyer MJS, et al. Phase 1b study of venetoclax-obinutuzumab in previously untreated and relapsed/refractory chronic lymphocytic leukemia. Blood. 2019;133(26):2765-2775. doi:10.1182/blood-2019-01-896290
53. Byrd JC, Brown JR, O'Brien S, et al. Ibrutinib versus ofatumumab in previously treated chronic lymphoid leukemia. N
Engl J Med. 2014;371(3):213-223. doi:10.1056/NEJMoa1400376
54. Kaiser Family Foundation. Health insurance coverage of the total population. Accessed June 7, 2022. https://www.kff.org/other/state-indicator/total-population/
55. Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2016. Accessed June 7, 2022. https://seer.cancer.gov/archive/csr/1975_2016/
56. US Census Bureau. National population projections datasets, Table 1. Projected population by single year of age, sex, race, and hispanic origin for the United States: 2016 to 2060. Accessed June 7, 2022. https://www.census.gov/data/datasets/2017/demo/popproj/2017-popproj.html
57. Seymour EK, Ruterbusch JJ, Beebe-Dimmer JL, Schiffer CA. Real-world testing and treatment patterns in chronic lymphocytic leukemia: A SEER patterns of care analysis. Cancer. 2019;125(1):135-143. doi:10.1002/cncr.31738
58. Barrientos JC. Sequencing of chronic lymphocytic leukemia therapies. Hematology Am Soc Hematol Educ Program. 2016;2016(1):128-136. doi:10.1182/asheducation-2016.1.128
59. Mato AR, Hill BT, Lamanna N, et al. Optimal sequencing of ibrutinib, idelalisib, and venetoclax in chronic lymphocytic leukemia: results from a multicenter study of 683 patients. Ann Oncol. 2017;28(5):1050-1056. doi:10.1093/annonc/mdx031
60. Eyre TA, Lamanna N, Roeker LE, et al. Comparative analysis of targeted novel therapies in relapsed, refractory chronic lymphocytic leukaemia. Haematologica. 2021;106(1):284-287. Published 2021 Jan 1. doi:10.3324/haematol.2019.241539
61. Runyan A, Banks J, Bruni DS. Current and Future Oncology Management in the United States. J Manag Care Spec Pharm. 2019;25(2):272-281. doi:10.18553/jmcp.2019.25.2.272
62. US Food and Drug Administration. Highlights of prescribing information: RITUXAN (rituximab). Accessed June 7, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/103705s5464lbl.pdf
63. US Food and Drug Administration. Highlights of prescribing information: GAZYVA (obinutuzumab). Accessed June 7, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/125486s025lbl.pdf
64. US Food and Drug Administration. Highlights of prescribing information: BENDEKA (bendamustine hydrochloride). Accessed June 7, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/208194s020lbl.pdf



