


Impact of Shared Decision-Making and Patient Decision Aids on Health Care Cost and Utilization in the US: A Systematic Review
J Clin Pathways. 2022;8(8):33-43. doi:10.25270/jcp.2022.12.01
Received: May 2022; Accepted: July 2022
Abstract
Prior research supports use of shared decision-making (SDM) and patient decision aids (PtDAs) to promote patient-centered, high-quality care. Impact on costs and utilization is less clear. We conducted a systematic review to explore this impact in the context of value-based care in the United States. Using PubMed, we searched for articles published from January 2010 to September 2019 that were peer-reviewed, primary research, English language, and in the US setting. We analyzed articles that featured SDM, a PtDA, or a combination of both with outcomes in three categories: cost, utilization, and prevention-related care. Fifty-one articles met inclusion criteria (15 SDM, 25 PtDA, 11 combined). Articles covered diverse clinical areas, the most common one being oncology (N = 15). The majority (61%) of reviewed articles reported statistically significant findings indicating that SDM and PtDAs reduce health care costs and utilization and/or increase prevention-related care. Additionally, 71% of all articles reported at least one outcome with no significant difference (an article can have multiple outcomes). Findings were similar across interventions (SDM vs PtDA vs combined). Eight articles reported cost outcomes: five found outcomes with decreases, six found outcomes with no difference. Twenty-five articles reported utilization outcomes: 14 decreases, three increases, 19 no difference. Thirty-two articles reported prevention-related care outcomes: two decreases, 20 increases, 21 no difference. Two subcategories had the most articles showing improved utilization and prevention-related care: crisis utilization and nonopioid medication prescribing/adherence. Overall findings suggest that SDM and PtDAs often reduce costs or improve utilization, and differences in results across settings and disease areas may reflect the heterogeneity of study purposes, designs, and outcomes measured. Further research is needed to investigate return on investment; impact across clinical areas; and optimal combination of interventions to improve cost, utilization, and patient-centered outcomes.
Shared decision-making (SDM) has been called the “pinnacle of patient-centered care” and elevated as a mechanism for improving value-based care, defined as a system in which payment for health care services is tied to the quality and/or outcomes of the care delivered.1-3 Patient decision aids (PtDAs) have also emerged as tools for patients to take a more active role in their care decisions.4 In the United States, the move to value-based care was catalyzed by the Affordable Care Act, and policymakers have begun to integrate SDM into various state and federal value-based programs.5,6
SDM is a process by which patients and clinicians work together to explore care choices, evaluate evidence of the benefits and risks of each choice, understand goals and preferences, and jointly make informed care decisions.1 PtDAs are evidence-based tools that facilitate SDM and promote patient activation in the decision-making process.4 PtDAs are available for many specific clinical conditions and screening or treatment options in various formats such as paper, video, or web-based platforms.7 PtDAs are often used as a component of or precursor to SDM, but do not by themselves constitute SDM in the absence of collaboration between clinician and patient to make a decision. Similarly, patient education materials (eg, brochures, handouts) may help increase patient knowledge and provide background information, but they are not considered PtDAs in the absence of detailed focus on options and outcomes to promote patient engagement in the decision-making process.8
SDM has been shown to increase patient knowledge, reduce decisional conflict, and improve patient health.9-12 Some studies have also demonstrated improvements in other care outcomes, such as treatment/medication adherence and quality of life.13-16 Additionally, PtDAs have been associated with improved patient knowledge, informed decision-making, and reduced decisional conflict.8,17,18 However, definitions and processes of SDM and PtDAs are inconsistent across the landscape, creating difficulty in generalizing results across populations and diverse clinical conditions.
While the main goal of SDM and PtDAs is to promote patient-centered, high-quality care, their impact on cost of care is less clear. There is also a lack of understanding about how SDM and PtDAs can be deployed in tandem to optimize outcomes related to utilization, cost, and preventive care. Some stakeholders believe SDM will lead to lower health care costs, assuming that patients who are informed about treatment benefits and limitations (and empowered to make decisions) will select less invasive and less costly treatment.19 A systematic review found that PtDAs reduced the number of patients who chose elective surgery, but individual patients may make different decisions depending on their preferences and clinical factors.18,20 Results were inconclusive in another systematic review that focused specifically on cost savings from using PtDAs.21 A 2020 publication found that implementing PtDAs for some conditions may actually increase the number of patients choosing to undergo certain elective knee and hip procedures.7
Findings are also mixed for the impact of SDM and PtDAs on prevention-related care outcomes. For example, one review found that collaborative care interventions using an SDM approach were associated with improved medication adherence among patients with depression, while another review found that evidence was inconclusive that using PtDAs improves adherence to oral anticoagulants among patients with atrial fibrillation.22,23 Similarly, a 2020 review and meta-analysis found that SDM has been associated with increased influenza vaccination rates, while another 2020 review found that evidence for the impact of PtDAs on vaccination coverage was inconclusive.24,25
Considering potential return on investment further complicates the picture. Providers with limited resources may favor PtDAs because clinicians and health system administrators perceive that SDM requires additional resources for implementation and delivery, whereas PtDAs make the decision-making process more efficient by reducing the time spent with each patient.26,27 Additionally, SDM and PtDA processes that help patients decide whether to engage in prevention-related care—such as screening for health conditions, taking medications to manage chronic conditions, or seeking mental health services—can lead to increased health care costs in the short term but may help prevent longer-term costs.28
With the continued move toward value-based care, understanding the relative effectiveness of SDM and PtDAs on reducing health care costs and unnecessary utilization can help providers, payers, and policymakers assess the value of these strategies in clinical practice. To evaluate the hypothesis that SDM and PtDA interventions reduce costs and utilization and increase prevention-related care, we performed a systematic literature review of SDM, PtDAs, and combined SDM and PtDA interventions. Prior systematic reviews have not attempted to synthesize and compare the evidence on SDM and PtDAs as distinct concepts, nor do they study utilization, cost, and prevention-related care. Our review adds to the literature by summarizing evidence on the impact of SDM as a process, PtDAs as tools to support decision-making, and the combination of SDM and PtDAs on cost, utilization, and prevention-related care.
Methods
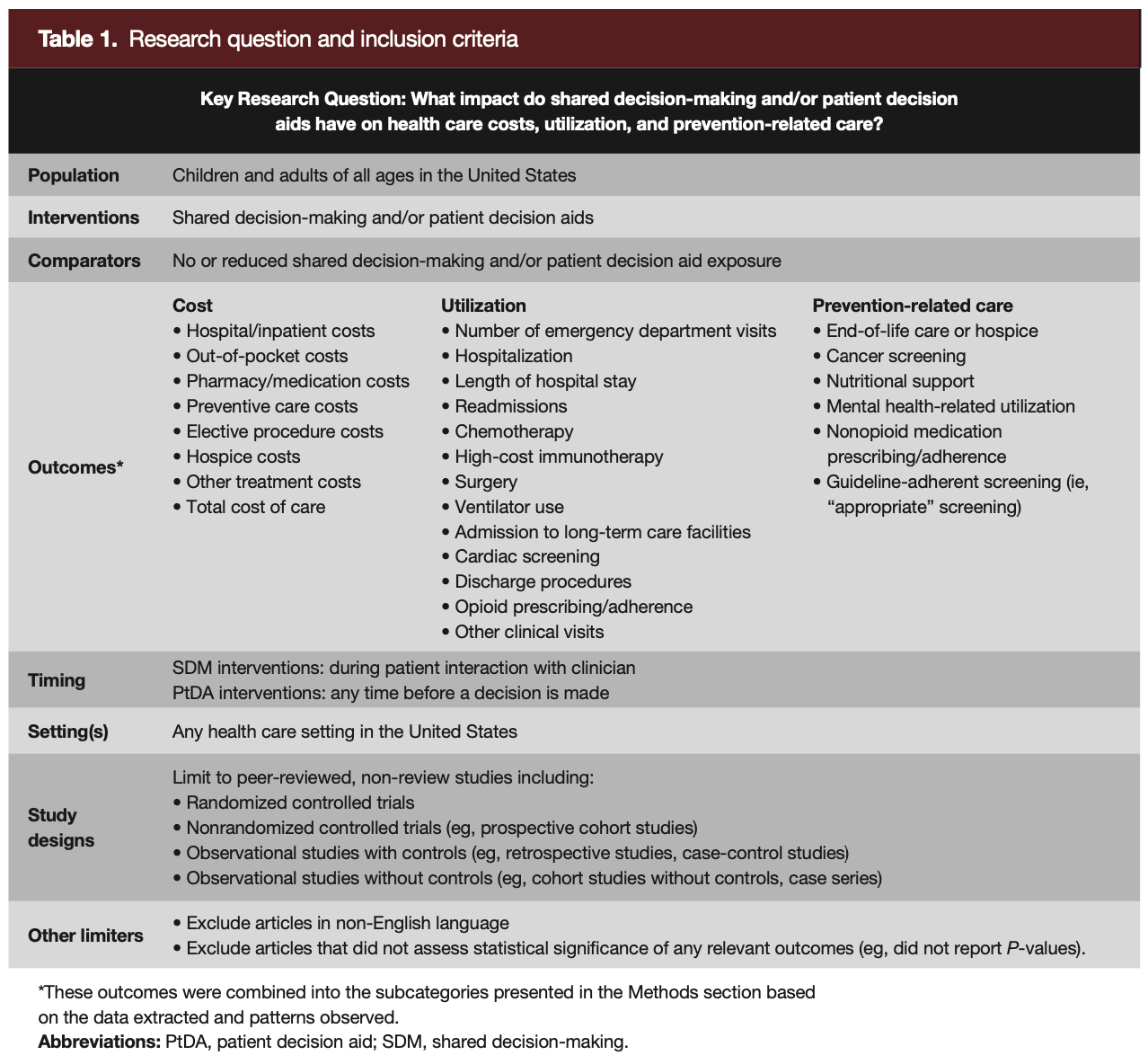
We followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines.29 We used a PICOTS (Population, Interventions, Comparator[s], Outcomes, Timing, Setting[s]) framework,30 with the addition of study design and other limiters, to guide the search strategy and overall scope of the systematic review (Table 1).
Search and Article Selection
We conducted a structured PubMed search for peer-reviewed English language articles published between January 1, 2010, and September 30, 2019, to capture articles published after the implementation of the Affordable Care Act, which included a provision to encourage greater use of SDM.31 We employed Boolean logic and terms in our search process. Using Covidence as our systematic review workflow platform, reviewers screened titles, abstracts, and full texts, with at least two reviewers independently screening. Disagreements were resolved by an adjudicator. We included articles that tested a SDM and/or PtDA interventions in a US health care setting and reported at least one cost, utilization, or prevention-related care outcome.
Intervention Criteria
Following the National Quality Forum guidelines, we defined SDM as “a process of communication in which clinicians and patients work together to make optimal health care decisions.”32 Examples included structured decision-making meetings or patient-reported SDM as recorded on tools such as the 9-item Shared Decision Making Questionnaire (SDM-Q-9).33 By using this definition as part of the inclusion criteria, our goal was to focus on the collaborative SDM process wherein clinicians and patients work together to make a health care decision.
We defined PtDAs as evidence-based tools in any format designed to educate patients and their caregivers or surrogates about their options, such as benefits, risks, and costs, and to help patients to actively participate in making informed, deliberate health care choices.4,34 We included both PtDAs that patients used with clinicians and those that they used independently (eg, to prepare for an appointment).
We defined interventions as combined when they included both SDM and a PtDA. For example, Prabhu et al describe a 10-minute SDM session in which a clinician reviewed information verbally while a patient viewed a computer-based PtDA.35
Study Design
We excluded discrete choice experiments, decision scenarios, hypothetical results (eg, patient preferences for treatment with unknown adherence to treatment plan), reviews, commentaries, opinion pieces, and case studies. We also excluded articles in non-English languages and articles that did not assess or report statistical significance of any relevant outcomes (eg, did not report P-values).
Evaluation
Reviewers extracted key data elements—such as study characteristics, intervention type, and outcomes—from each article into a predesigned data extraction spreadsheet using Microsoft Excel 365. At least two reviewers were involved in extraction for each article, with one reviewer completing primary extraction and a second reviewer validating each field.
We assessed each article’s level of evidence based on the Quality Rating Scheme for Studies and Other Evidence presented by The Journal of the American Medical Association (modified from the Oxford Centre for Evidence-based Medicine for ratings of individual studies)36 and evaluated potential bias in randomized controlled trials (RCTs) using Cochrane’s risk of bias tool.37
We identified three main categories of outcomes: cost, utilization, and prevention-related care.
- The cost category addressed outcomes pertaining to a dollar amount.
- The utilization category addressed outcomes involving resource-intensive services or procedures.
- The prevention-related care category addressed outcomes involving processes or procedures that could potentially improve other health outcomes and reduce future high-cost utilization.38 We chose the term “prevention-related care” because many of the outcomes in this category are not considered “preventative care” but may prevent adverse outcomes or unnecessary spending downstream.
We counted an article within a given category when at least one outcome showed an increase, decrease, and/or no significant difference in that category. This is consistent with the methods described by the 2008 Centre for Reviews and Dissemination to summarize study characteristics and key outcomes.39
Only outcomes that were statistically significant (ie, P ≤ .05) were counted as increases or decreases. If an article’s outcomes in a given category had conflicting results (eg, some increased while others decreased or showed no differences), we counted the article once for each result. For example, Cox reported nine relevant outcomes: two cost outcomes that decreased, two cost outcomes with no differences, and five utilization outcomes with no differences.40 This article appears in the results three times: once for decreased costs, once for no differences in costs, and once for no differences in utilization.
Descriptive statistics, graphics, and other analyses were calculated using Microsoft Excel 365. We did not conduct a meta-analysis due to the wide variety of study designs, populations, and interventions in the included articles.
Results
Search Results
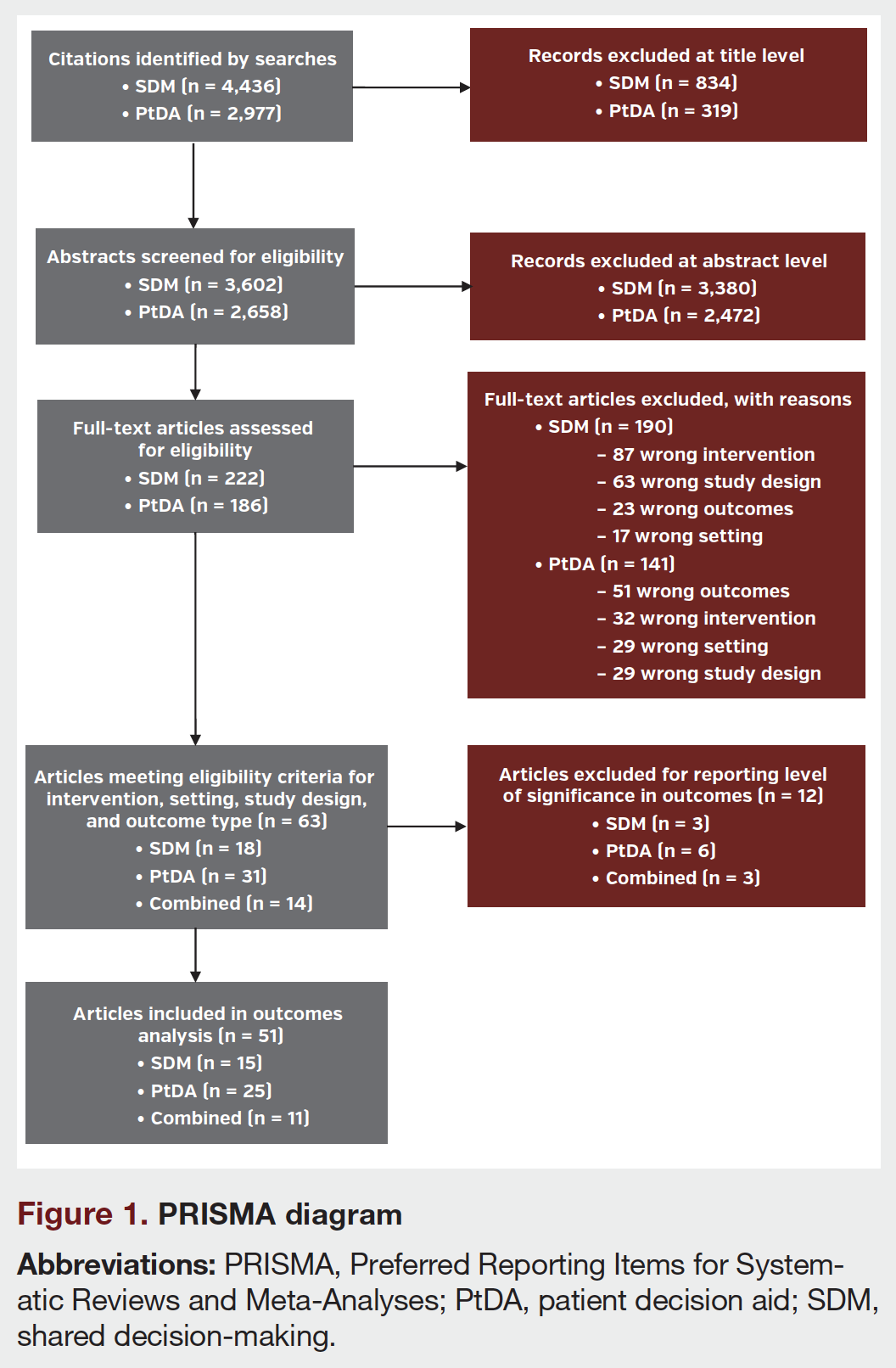
Our PubMed searches identified 4436 SDM and 2977 PtDA articles, with some articles overlapping across searches. After reviewing titles, abstracts, and full texts, a total of 51 articles met all inclusion criteria and were included in the analysis. Articles were primarily excluded due to wrong intervention (ie, not meeting the SDM and PtDA criteria), wrong study design, wrong outcomes, and/or wrong setting (ie, not in the United States). Figure 1 displays a PRISMA diagram of articles identified, excluded, and retained.
Study Characteristics
The 51 included articles covered a variety of SDM and PtDA interventions. Fifteen articles featured SDM interventions, 25 featured PtDA interventions, and 11 described combined interventions. While many articles focused on only SDM, only a PtDA, or a single combined SDM/PtDA intervention, only one study (Stamm 201741) compared the use of a PtDA alone to an SDM/PtDA combined intervention.
Included studies were diverse in sample sizes, ranging from 27 to 5,653,616 individuals, and included patients from a variety of racial or ethnic groups, genders, and ages. The majority (N = 49) focused on adult populations (14 SDM, 25 PtDA, 10 combined). Two articles addressed pediatric-only populations (1 SDM, 1 combined). While most articles were not restricted to a specific race/ethnicity, four PtDA articles focused on Black individuals. Eight articles restricted their research to only women (2 SDM, 3 PtDA, 3 combined) and four articles focused on only men (1 SDM, 2 PtDA, 1 combined).
The most common clinical area across articles was oncology (N = 15; 3 SDM, 10 PtDA, 2 combined), with many articles addressing cancer screening. Other common clinical areas included cardiovascular conditions, orthopedics, and mental health. Studies were conducted in a variety of care settings, ranging from ambulatory clinics to hospitals to nursing homes, with primary care being the most common (N = 19).
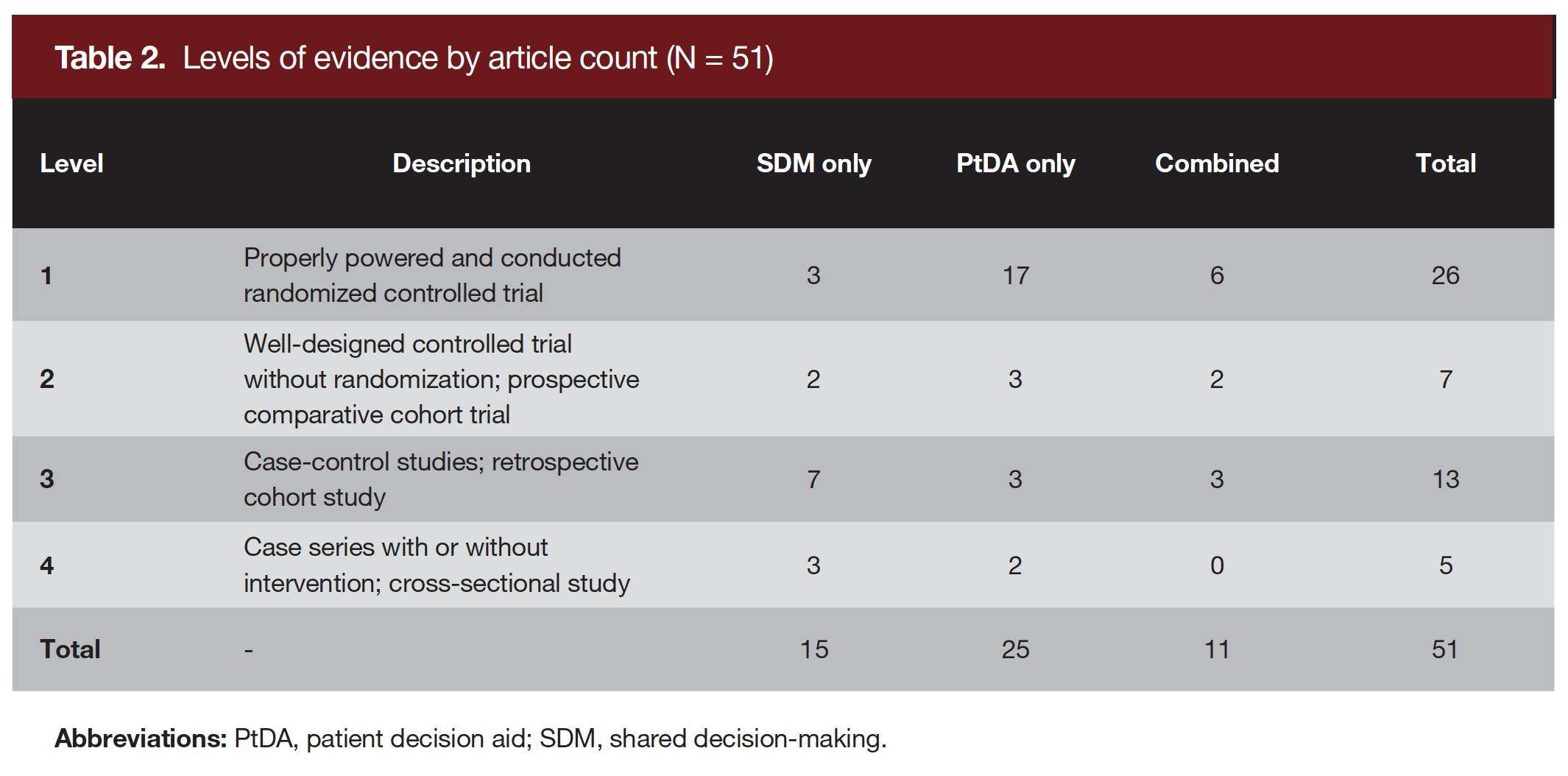
We compared level of evidence and risk of bias for included articles. Table 2 describes four levels of evidence and shows how many articles met the criteria for each. Twenty-six of 51 articles were Level 1 evidence (ie, RCTs), including the majority of PtDA-only articles (17 of 25). Conversely, seven of the 15 SDM articles had Level 3 evidence (ie, case-control studies, retrospective cohort studies), with 13 total Level 3 articles across interventions. This variation in level of evidence may be due to differences in intervention components: by our definition, SDM interventions involve collaboration between clinicians and patients, which can be difficult to randomize in a study design, whereas PtDAs may be more amenable to RCT design.
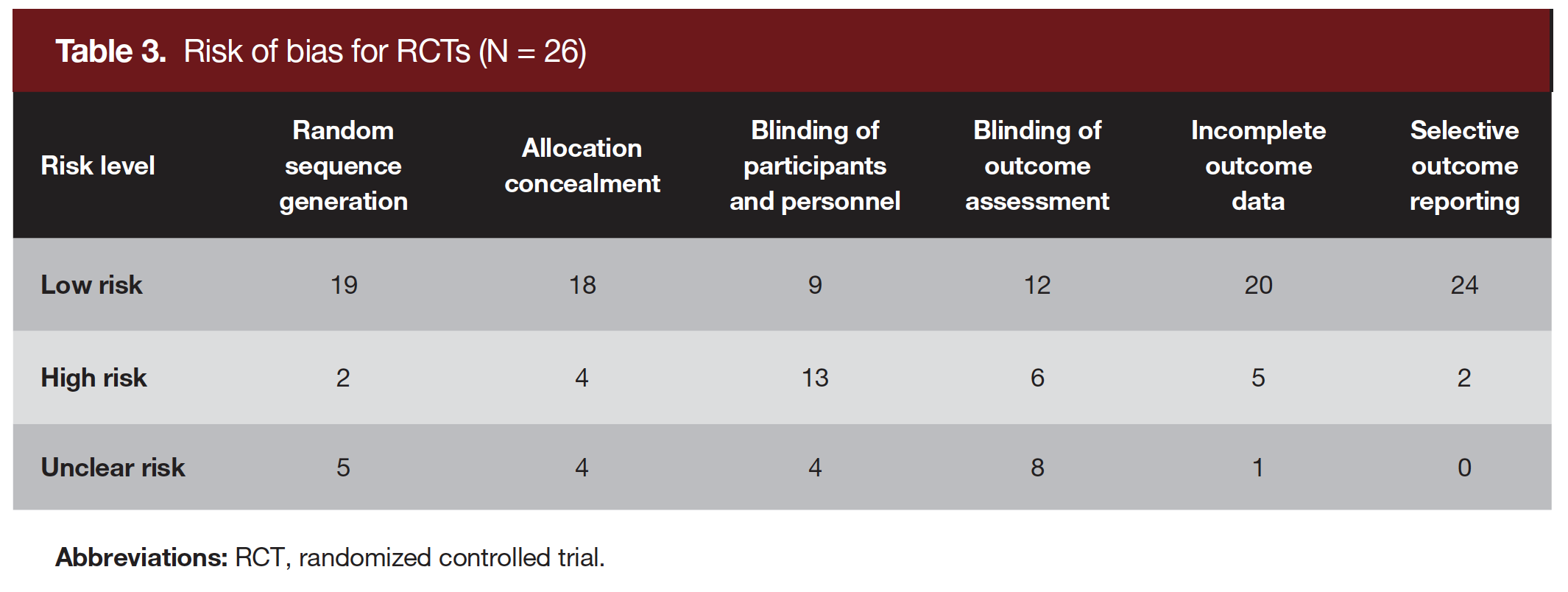
Risk of bias was low for most of the Cochrane risk of bias domains across included RCTs (Table 3). However, 13 RCTs were high risk for the “Blinding of Participants and Personnel” domain, possibly due to difficulties in blinding patients and clinicians to components of the SDM and/or PtDA intervention.
Outcome Categories
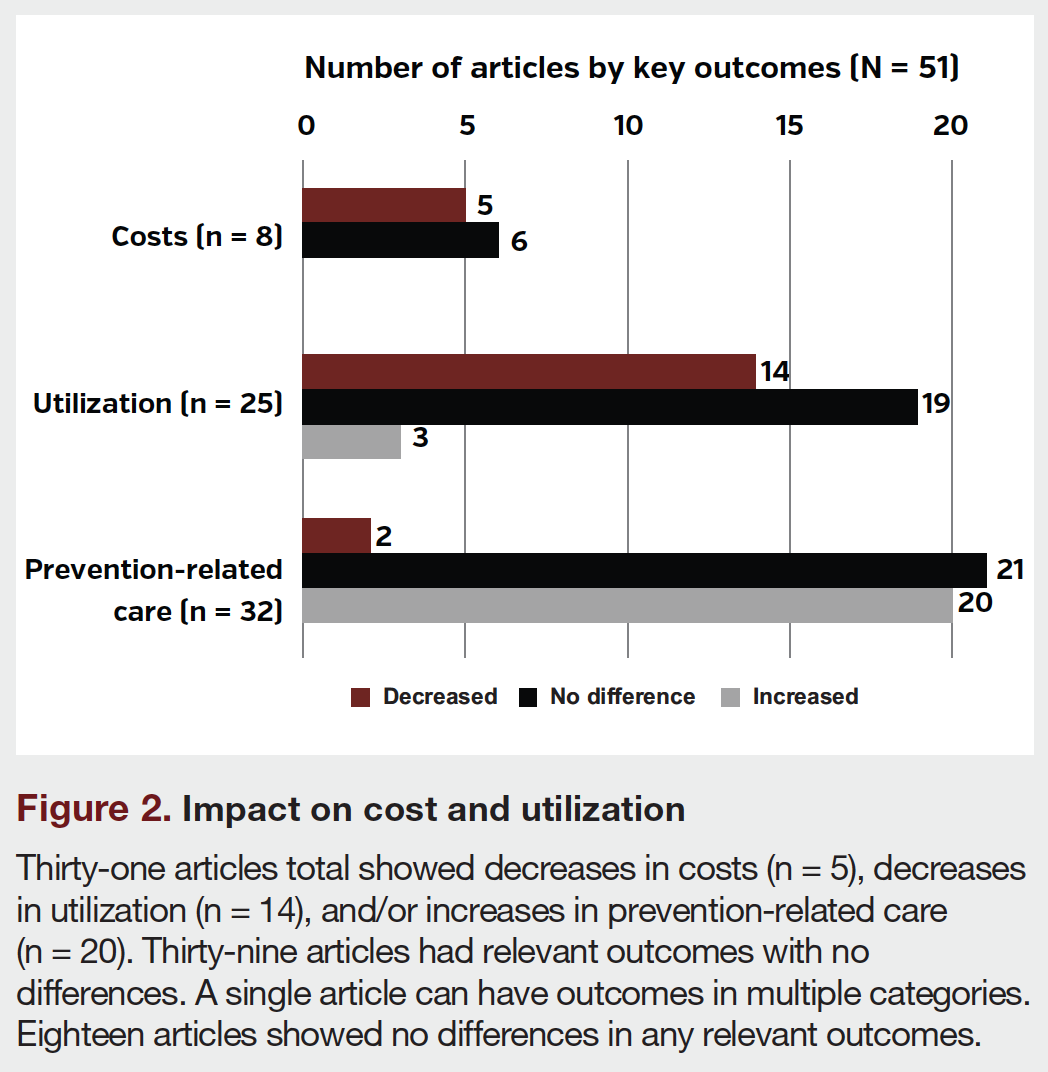
The 51 articles reported outcomes of interest as follows across the three main categories: cost (N = 8), utilization (N = 25), and prevention-related care (N = 32). Thirty-nine articles had outcomes in only one category, 10 had outcomes in two categories, and only two articles9,42 had outcomes in all three categories. Figure 2 summarizes the number of articles with cost, utilization, and prevention-related care outcomes. We divided these outcomes into subcategories to enable more detailed analysis.
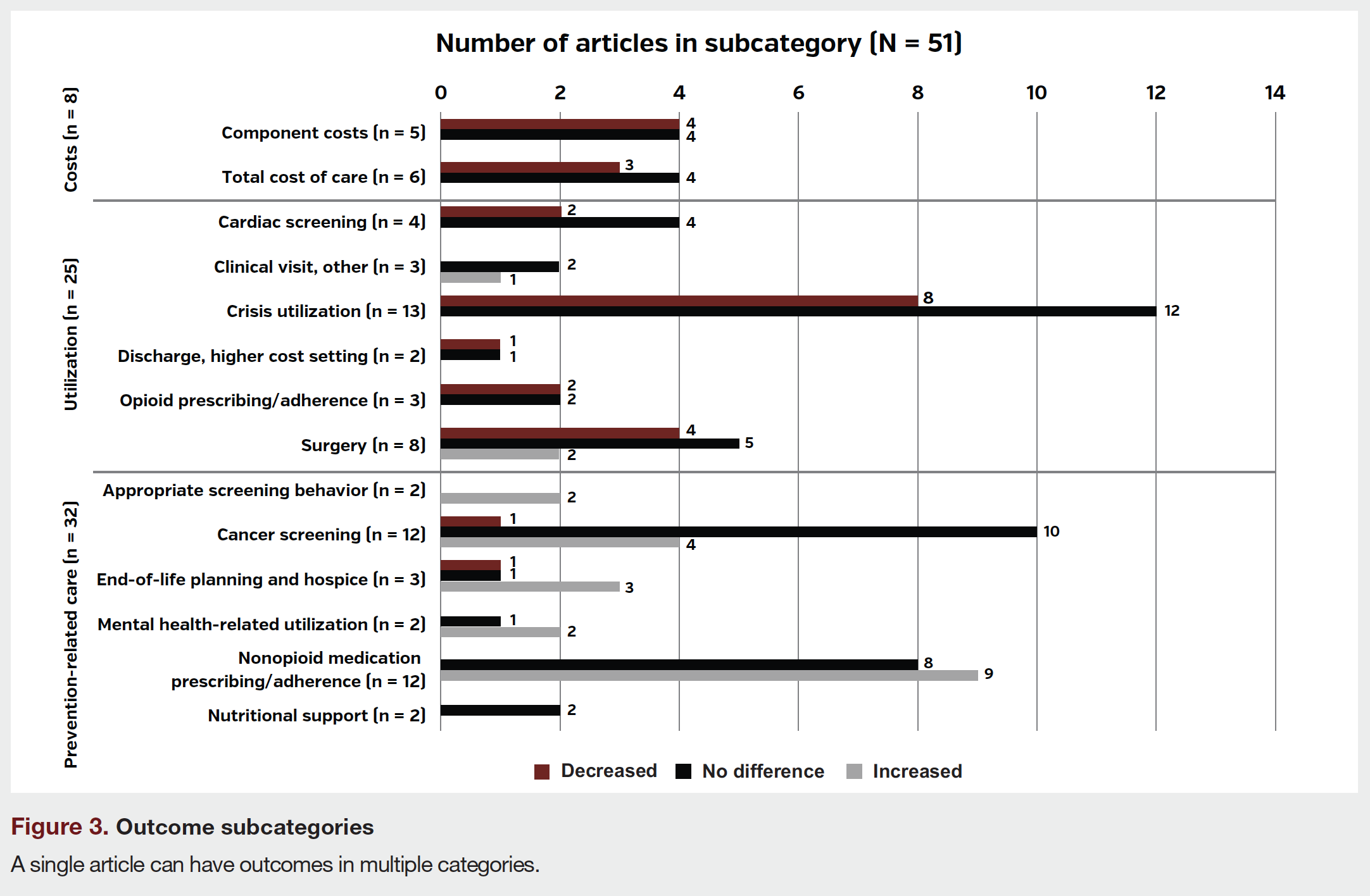
- Two subcategories of cost outcomes included component costs (eg, hospital, pharmacy, out-of-pocket, treatment) and total cost of care.
- Six subcategories of utilization outcomes included cardiac screening; crisis utilization (eg, hospitalization, emergency department use, ventilator use); discharge, higher cost setting; opioid prescribing/adherence; surgery; and clinical visit/other.
- Six subcategories of prevention-related care outcomes included end-of-life planning or hospice; nonopioid medication prescribing/adherence; cancer screening; nutritional support; mental health-related utilization; and “appropriate” screening behavior in alignment with clinical guidelines.
Figure 3 shows the number of articles with outcomes in each of the 14 subcategories.
About 61% of the articles (31 of 51) present results consistent with the hypothesis that SDM and PtDA interventions decrease cost or utilization and/or increase prevention-related care. Additionally, 76% of the articles (39 of 51) had outcomes with no differences. Five articles found outcomes contrary to our hypotheses by reporting increases in utilization or decreases in prevention-related care, and 18 articles found no significant differences in any relevant outcomes. A single article can have outcomes in multiple categories or multiple outcomes in the same category.
Figure 2 illustrates the impact of studied interventions on main outcome categories. Figure 4 further divides these results by level of evidence. The highest proportion of Level 1 evidence (RCTs) were found in prevention-related care, with eight of the 17 RCTs showing outcomes that increased.
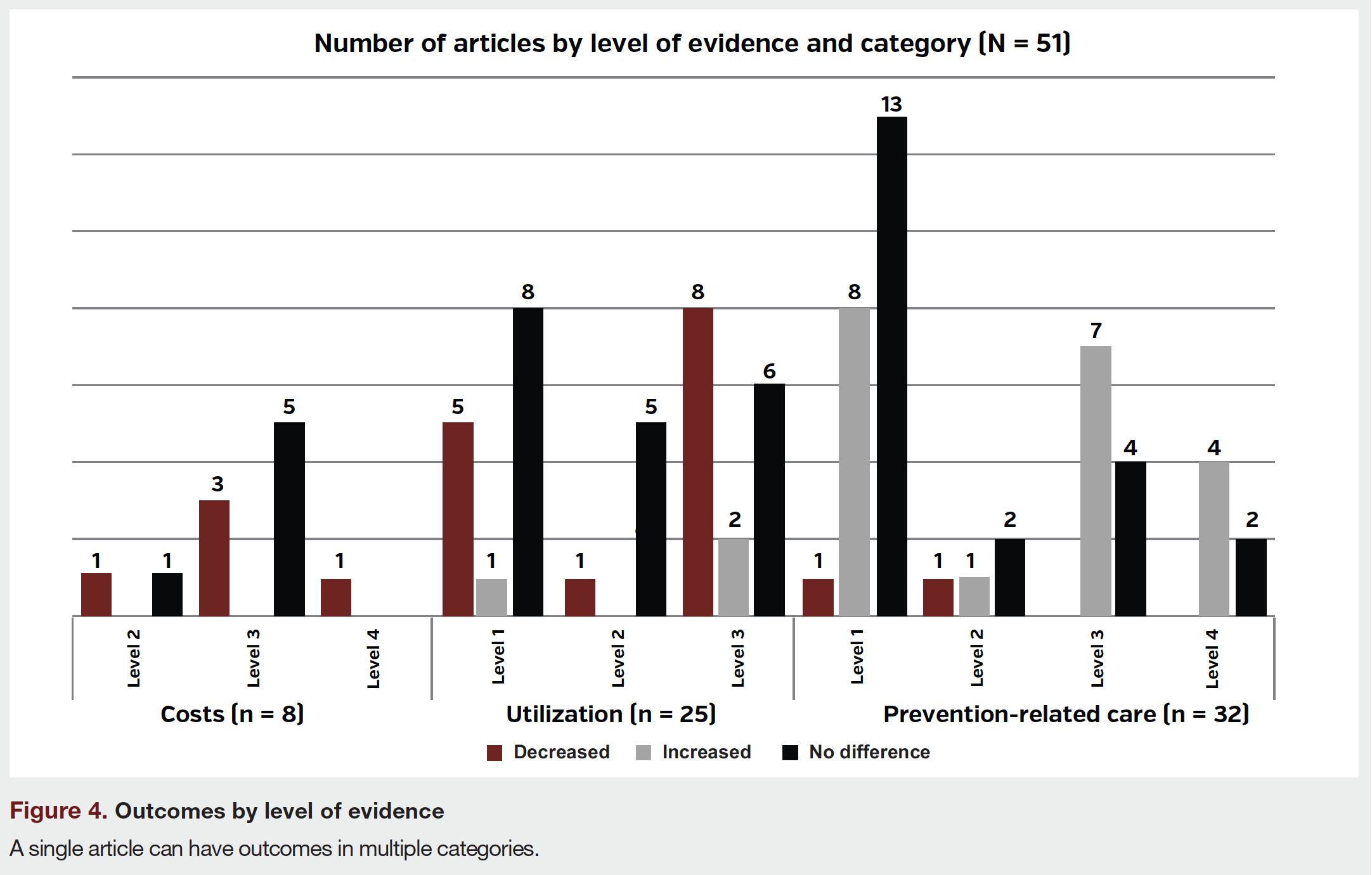
- Eight articles, none of them RCTs, assessed costs: five reported outcomes that decreased and six reported outcomes that showed no difference.
- Twenty-five articles, including 11 RCTs, assessed utilization: 14 reported outcomes that decreased (5 RCTs), three reported increases (1 RCT), and 19 reported outcomes that showed no difference (8 RCTs).
- Thirty-two articles, including 17 RCTs, assessed prevention-related care: 20 reported outcomes that increased (8 RCTs), two reported decreases (1 RCT), and 21 reported outcomes that showed no difference (13 RCTs).
We conducted a subanalysis of Level 1 studies with low risk of bias in all domains. Of the six articles with the highest level of evidence, one featured SDM and five featured PtDAs. The SDM article43 captured one utilization outcome, median number of hospital days, and did not find a significant difference. One of the PtDA articles44 found significant decreases in cardiac stress testing (utilization). Ibrahim et al45 found increases in total knee replacement surgery, while Watts46 found increases in treatment for posttraumatic stress disorder after use of a PtDA. The other three articles did not find significant differences in any relevant outcomes.
As shown in Figure 3, an analysis of subcategories found evidence that SDM and PtDAs were associated with increases in medication prescribing/adherence to nonopioids in the majority (75%) of the 12 articles that reported this outcome. Eight of 13 (62%) articles reported interventions associated with decreases in crisis utilization. Many articles in both subcategories also reported at least one outcome with no differences (8 of 12 for medication adherence to nonopioids and 12 of 13 for crisis utilization). The most frequently studied outcome subcategory was cancer screening, reported in 12 articles. Ten of these articles found at least one screening outcome with no differences, four found increases, and one found decreases. Results for the eight articles reporting cost outcomes were also mixed. Three of the six articles reporting total cost of care found decreases, and four reported outcomes with no differences. Similarly, four of the five articles reporting component costs found decreases, and four found outcomes with no differences.
Figure 5 shows relative impacts of SDM, PtDA, and combined interventions on the main categories of cost, utilization, and prevention-related care. At least half of the articles for every intervention type and category had at least one outcome with no significant differences.
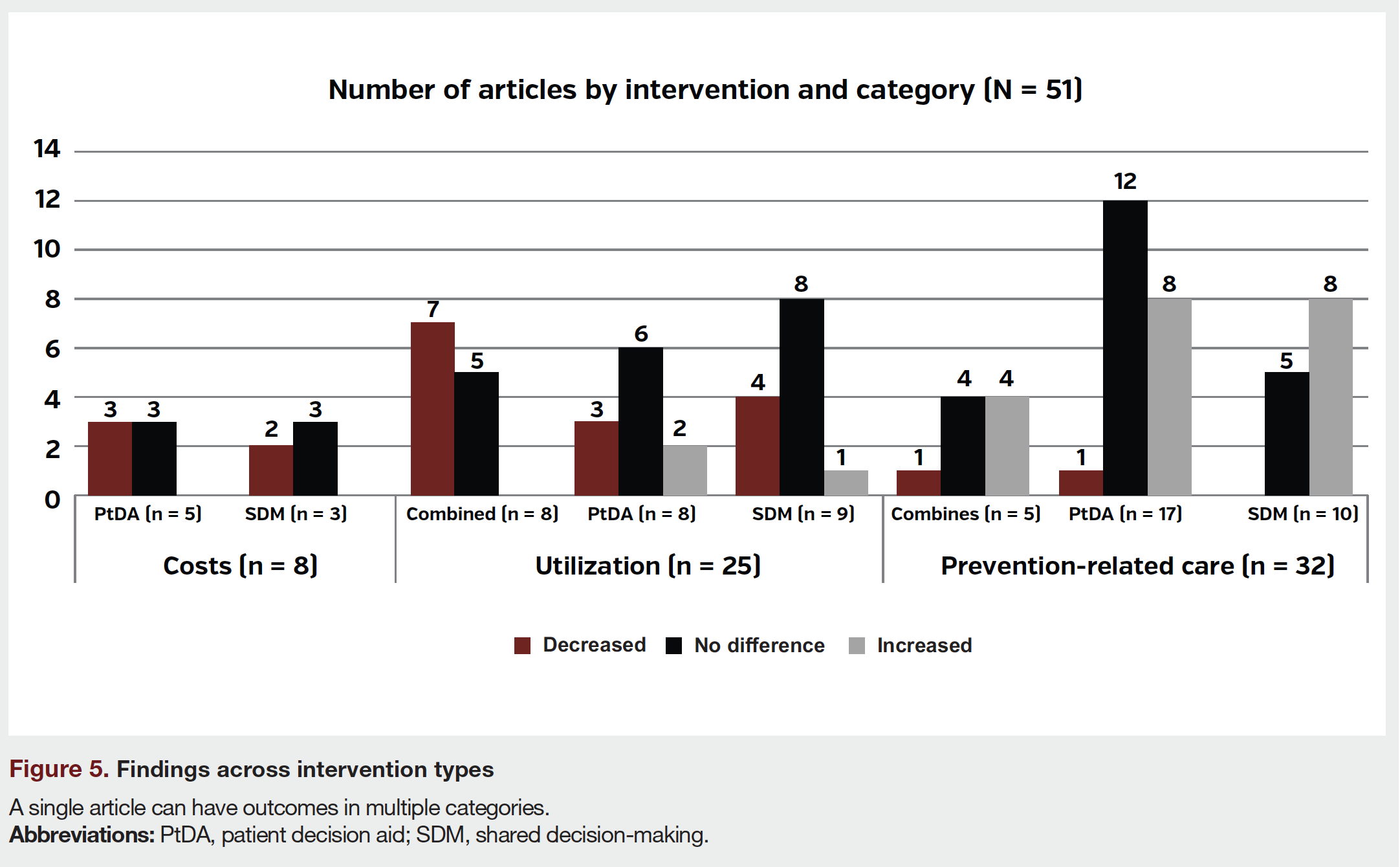
- Cost outcomes: Performance on cost outcomes was similar; SDM (2 of 3) and PtDA (3 of 5) intervention articles found decreases. No combined-intervention articles assessed costs.
- Utilization outcomes: More combined-intervention articles found decreases (7 of 8) compared to articles testing only SDM (4 of 9) or PtDA (3 of 8) interventions.
- Prevention-related care outcomes: A larger proportion of SDM (8 of 10) and combined-intervention (4 of 5) articles found increases as compared to PtDA articles (8 of 17).
Discussion
Variation in Study Results
A majority of articles showed some decreases in costs and utilization or increases in prevention-related care associated with SDM and PtDA interventions. However, evidence was mixed both across articles and within individual articles, with 76% of articles reporting at least one relevant outcome with no significant difference.
The variation in results may be related to the focus and methods of included articles. The studies reported by some articles were not intended to investigate cost or utilization as primary intervention outcomes but reported these results as secondary outcomes. For example, Hess et al demonstrated that using a PtDA in the emergency department reduced frequency of the primary outcome, cardiac stress testing (in the utilization category), without increasing the secondary outcomes of rehospitalizations or repeat emergency department visits (utilization).44
For articles intended to directly test the impact of an intervention on cost or utilization, variation in outcomes may be due to differences in the intervention design (eg, brochure vs computer-based PtDA), care setting (eg, inpatient vs outpatient), and/or patient population (eg, pediatric vs adult). Another reason for the variation in results could be that our review explored a broad range of therapeutic areas and did not restrict its scope to a specific type of health condition.
The impact of SDM and PtDAs on cost and utilization may also vary based on the severity and type of condition, and different intervention strategies may be more impactful in different situations. For example, SDM may have a greater impact in decreasing costs for specific diseases (eg, late-stage diseases47) where improved engagement of the patient in decisions regarding potential treatment options could result in achieving the patient’s goals of care while also decreasing costs (eg, by forgoing unwanted treatment at the end of life). In contrast, PtDAs may be more efficient to implement for decisions related to preventive care (eg, cancer screening). In the absence of conclusive evidence comparing SDM vs PtDAs, one hypothesis might be that PtDAs have a greater potential for return on investment when the goal is to reduce costs. This is because, as indicated in prior literature, PtDAs may save staff time and make the decision-making process more efficient.26,27
Five articles performed contrary to our hypothesis, but these may actually reflect care improvements. For example, Ibrahim et al found that a PtDA increased total knee replacement surgery for Black patients with end-stage osteoarthritis of the knee.45 Increasing surgery in this instance may represent improved access and help reduce health care disparities. Arterburn et al found that PtDA use was associated with an increased rate of transurethral prostate procedures at 180 days among patients with prior treatment for benign prostatic hyperplasia.48 Though this represents increased utilization (vs no treatment), transurethral prostate procedures may be an alternative to higher-cost options.49 Likewise, several articles assessed prevention-related care (specifically cancer screening) that may not be recommended depending on individual patients’ characteristics, such as advanced age.
Outcomes in the Value-based Care Context
While evidence shows potential of SDM and PtDAs for improving patient outcomes, impact on costs may be limited due to health care provider and patient incentives. In 2018, approximately 64% of US health care payments were still fee-for-service.50 While SDM and PtDAs may lead to some patients choosing less costly treatments, decisions of individual patients may not be enough to counterbalance fee-for-service payment models that incentivize providers for higher volumes of care or more expensive treatments. Research also indicates that prevention-related care may not lead to major savings in health care spending and is not guaranteed to reduce costs. For example, a 2010 study indicated that even if patients achieved 90% compliance with 20 evidence-based preventive services, the US health care system would have saved only 0.2% of the total amount of personal health care spending.28
In emerging value-based payment models, a favorable result of SDM and PtDAs might be to promote decisions that account for patient preferences without adding significant costs. The 2022 recommendations of the US Preventive Services Task Force endorsed SDM as a means to advance the “ethical imperative” of allowing patients to be more “informed and involved in their health care decisions,” whether or not it improves outcomes.51
In some cases, greater health care utilization and higher costs arising from SDM or PtDAs may provide arguably higher value depending on patient preferences, the clinical situation, improved quality outcomes, and/or future costs avoided. The Centers for Medicare & Medicaid Services may have recognized this, because the agency included SDM quality measures in several value-based payment models such as the Merit-Based Incentive Payment System and the Medicare Shared Savings Program.52,53 At the US state level, the Washington State Health Care Authority supports and regulates SDM and has recognized the value of using PtDAs as part of the SDM process. In 2016, Washington became the first state to certify PtDAs that meet certain standards established by the International Patient Decision Aids Standards Collaboration.54
Limitations and Generalizability
Our findings cannot be generalized to interventions that do not meet our SDM and PtDA inclusion criteria. Though researchers have described a broad array of practices as SDM or PtDA interventions, we focused our inquiry on interventions that met definitions advanced by the National Quality Forum and the Medicare Payment Advisory Commission. Applying this precision allowed us to focus on the impact of these practices within the US value-based care context; however, we were limited by the descriptions provided in each article and were unable to validate whether patient values and preferences were elicited and incorporated into the decision-making process. Additionally, our categorization of which outcomes fit in the utilization and prevention-related care categories relied on our understanding of the value-based care landscape.55,56 Our analytic methods precluded assessing the magnitude of the effects or differentially weighting studies (eg, based on level of evidence or risk of bias).57
Prior systematic reviews included studies from a broad range of countries and health care systems. Our review focused on SDM and/or PtDA practices in the United States to understand their impact on utilization in this unique health care system. Although the findings from this review cannot be generalized beyond the United States, they may also be relevant to stakeholders in international settings who are working toward patient-centered practices in value-based care models.
Directions for Future Research
Further research is needed to better understand the role of SDM and PtDAs in specific clinical contexts and assess how these interventions can work together to improve outcomes. Considering the varying definitions and types of SDM and PtDA interventions, further research is also needed to identify common characteristics of effective PtDA and/or SDM interventions. A 2019 systematic review offers a starting point by documenting potential common SDM characteristics.58 Additionally, research is needed to understand the implications of using a PtDA vs SDM or combined-intervention process to guide patient-provider communication, including relative return on investment. Medication adherence may be a particularly interesting topic to explore given the work that has already been done in this area.
Conclusion
Prior research has shown the relevance of SDM and PtDAs in improving patient outcomes. Our systematic review on SDM and PtDAs in the United States found that these interventions often, but not always, yield decreases in costs and utilization and increases in prevention-related care that may result in downstream savings.
However, evaluating patient-centered processes in the value-based care environment is complex. Increases in utilization sometimes reflect more equitable care, and unchanged costs mean increased value when quality improves. Thus, future research may find that PtDAs may have a higher return on investment in some contexts, while SDM and combined interventions lead to better patient care in others. Further research is needed to assess performance differences across interventions, the impact of these interventions on other patient-centered outcomes (eg, quality of care, patient satisfaction), and relative return on investment.
The stated goal of SDM and PtDA interventions is often to help patients share in deciding what is right for their care, whether or not these decisions create savings.4,9 While evidence suggests SDM and PtDAs may help right-size care in key areas, such as reducing crisis utilization and improving nonopioid medication prescribing/adherence, the interventions are not guaranteed to reduce health care costs.
Author Information
Theresa Schmidt, MA; Tom Valuck, MD, JD; Jacqlyn Riposo, MBA; Palak Patel, MHA; Brittany Perkins, MPH; Kimberly Westrich, MA; Robert W. Dubois, MD, PhD
Affiliations: Schmidt, Valuck, Riposo, Patel, and Perkins are employees of Real Chemistry, a health care innovation and consulting firm with many clients including, life sciences, nonprofit, payer, and provider organizations. At the time of writing, Westrich and Dubois were employees of NPC, an industry funded health policy research group that is not involved in lobbying or advocacy.
Address correspondence to: Theresa Schmidt, MA
701 8th St NW
Washington, DC 20001
Phone: (614) 440-8176
Email: tschmidt@realchemistry.com
Acknowledgments: The authors thank Kaitlyn Whiton and Matt Castner for their support for the analytic approach and Brian Sils for his many insightful comments and suggestions.
Disclosures: Funding for this study was provided the National Pharmaceutical Council. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, and writing and publishing the report.
References
1. Barry MJ, Edgman-Levitan S. Shared decision making--pinnacle of patient-centered care. N Engl J Med. 2012;366(9):780-781. doi:10.1056/NEJMp1109283.
2. LaPointe J. What Is Value-Based Care, What It Means for Providers? RevCycleIntelligence. 2019. Accessed June 14, 2021. https://revcycleintelligence.com/features/what-is-value-based-care-what-it-means-for-providers.
3. CMS’ Value-Based Programs. Centers for Medicare and Medicaid Services. 2020. Accessed June 14, 2021. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/Value-Based-Programs.
4. National Standards for the Certification of Patient Decision Aids. National Quality Forum. 2016. Accessed June 14, 2019. http://www.qualityforum.org/Publications/2016/12/National_Standards_for_the_Certification_of_Patient_Decision_Aids.aspx.
5. The SHARE Approach-Achieving Patient-Centered Care with Shared Decision making: A Brief for Administrators and Practice Leaders. Agency for Healthcare Research and Quality. 2020. Accessed June 14, 2021. https://www.ahrq.gov/health-literacy/professional-training/shared-decision/tool/resource-9.html.
6. Spatz ES, Elwyn G, Moulton BW, et al. Shared decision making as part of value based care: New U.S. policies challenge our readiness. Z Evid Fortbild Qual Gesundhwes. 2017;123-124:104-108. doi:10.1016/j.zefq.2017.05.012.
7. Hurley VB, Rodriguez HP, Kearing S, et al. The Impact Of Decision Aids On Adults Considering Hip Or Knee Surgery. Health Aff (Millwood). 2020;39(1):100-107. doi:10.1377/hlthaff.2019.00100
8. Stacey D, Légaré F, Col NF, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2014;(1):CD001431. doi:10.1002/14651858.CD001431.pub4.
9. Hughes TM, Merath K, Chen Q, et al. Association of shared decision-making on patient-reported health outcomes and healthcare utilization. Am J Surg. 2018 Jul; 216(1):7-12. doi: 10.1016/j.amjsurg.2018.01.011.
10. Shay LA, Lafata JE. Where is the evidence? A systematic review of shared decision making and patient outcomes. Med Decis Making. 2015;35(1):114-131. doi:10.1177/0272989X14551638.
11. Wyatt KD, List B, Brinkman WB, et al. Shared Decision Making in Pediatrics: A Systematic Review and Meta-analysis. Acad Pediatr. 2015;15(6):573-583. doi:10.1016/j.acap.2015.03.011.
12. Woodhouse KD, Tremont K, Vachani A, et al. A Review of Shared Decision-Making and Patient Decision Aids in Radiation Oncology [published correction appears in J Cancer Educ. 2017 Jun;32(2):246]. J Cancer Educ. 2017;32(2):238-245. doi:10.1007/s13187-017-1169-8.
13. LeBovidge J, Borok J, Udkoff J, et al. Atopic dermatitis: therapeutic care delivery: therapeutic education, shared decision-making, and access to care. Semin Cutan Med Surg. 2017;36(3):131-136. doi:10.12788/j.sder.2017.029.
14. Taylor YJ, Tapp H, Shade LE, et al. Impact of shared decision making on asthma quality of life and asthma control among children. J Asthma. 2018;55(6):675-683. doi:10.1080/02770903.2017.1362423.
15. Wilson SR, Strub P, Buist AS, et al. Shared treatment decision making improves adherence and outcomes in poorly controlled asthma. Am J Respir Crit Care Med. 2010;181(6):566-577. doi:10.1164/rccm.200906-0907OC.
16. Ben-Zacharia A, Adamson M, Boyd A, et al. Impact of Shared Decision Making on Disease-Modifying Drug Adherence in Multiple Sclerosis. Int J MS Care. 2018;20(6):287-297. doi:10.7224/1537-2073.2017-070.
17. Lim AH, Streeper NM, Best SL, et al. Clinical use of patient decision-making aids for stone patients. Can J Urol. 2017;24(4):8890-8894.
18. Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4(4):CD001431. doi:10.1002/14651858.CD001431.pub5.
19. O’Malley AS, Carrier E, Docteur E, et al. Policy Options to Encourage Patient-Physician Shared Decision Making: NIHCR Policy Analysis No 5. National Institute For Health Care Reform. 2011. Accessed June 15, 2021. https://nihcr.org/analysis/improving-care-delivery/prevention-improving-health/shared-decision-making/.
20. O’Connor AM, Llewellyn-Thomas HA, Flood AB. Modifying unwarranted variations in health care: shared decision making using patient decision aids. Health Aff (Millwood). 2004;Suppl Variation:VAR63-VAR72. doi:10.1377/hlthaff.var.63.
21. Scalia P, Barr PJ, O’Neill C, et al. Does the use of patient decision aids lead to cost savings? a systematic review. BMJ Open. 2020;10(11):e036834. doi:10.1136/bmjopen-2020-036834.
22. Samalin L, Genty J-B, Boyer L, Lopez-Castroman J, Abbar M, Llorca P-M. Shared decision-making: a systematic review focusing on mood disorders. Curr Psychiatry Rep. 2018;20(4):23. doi:10.1007/s11920-018-0892-0.
23. Song D, Zhou J, Fan T, et al. Decision aids for shared decision-making and appropriate anticoagulation therapy in patients with atrial fibrillation: a systematic review and meta-analysis. Eur J Cardiovasc Nurs. 2021;zvab085. doi:10.1093/eurjcn/zvab085.
24. Sanftenberg L, Kuehne F, Anraad C, Jung-Sievers C, Dreischulte T, Gensichen J. Assessing the impact of shared decision making processes on influenza vaccination rates in adult patients in outpatient care: a systematic review and meta-analysis. Vaccine. 2021;39(2):185-196. doi:10.1016/j.vaccine.2020.12.014.
25. Bruel S, Leclercq T, Ginzarly M, Botelho-Nevers E, Frappé P, Gagneux-Brunon A. Patient decision aid in vaccination: a systematic review of the literature. Expert Rev Vaccines. 2020;19(4):305-311. doi: 10.1080/14760584.2020.1742111.
26. Ankolekar A, Dekker A, Fijten R, et al. The Benefits and Challenges of Using Patient Decision Aids to Support Shared Decision Making in Health Care. JCO Clin Cancer Inform. 2018;2:1-10. doi:10.1200/CCI.18.00013.
27. Légaré F, Ratté S, Gravel K, et al. Barriers and facilitators to implementing shared decision-making in clinical practice: update of a systematic review of health professionals’ perceptions. Patient Educ Couns. 2008;73(3):526-535. doi:10.1016/j.pec.2008.07.018.
28. Maciosek MV, Coffield AB, Flottemesch TJ, et al. Greater use of preventive services in U.S. health care could save lives at little or no cost. Health Aff (Millwood). 2010;29(9):1656-1660. doi:10.1377/hlthaff.2008.0701.
29. Welcome to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) website! PRISMA. Accessed June 14, 2021. http://prisma-statement.org/.
30. Hartmann KE, Matchar DB, Chang SM. Assessing Applicability of Medical Test Studies in Systematic Reviews. In: Chang SM, Matchar DB, Smetana GW, Umscheid CA, eds. Methods Guide for Medical Test Reviews. Rockville (MD): Agency for Healthcare Research and Quality (US); June 2012.
31. Patient Protection and Affordable Care Act of 2010, Pub. L. No. 111–148, 124 Stat. 119 (2010), Codified as Amended 42 U.S.C. § 18001.
32. National Quality Partners™ Action Brief. Shared Decision Making: A Standard of Care for All Patients. National Quality Forum. October 2017. Accessed June 14, 2021. https://www.qualityforum.org/NQP/Shared_Decision_Making_Action_Brief.aspx.
33. SDM-Q-9/SDM-Q-DOC: The 9-item Shared Decision Making Questionnaire. Patient ALS Partner. Accessed June 14, 2021. http://www.patient-als-partner.de/index.php?article_id=20&clang=2%2F.
34. Report to the Congress: Aligning Incentives in Medicare. Medicare Payment Advisory Commission. June 2010. Accessed June 14, 2021. http://medpac.gov/docs/default-source/reports/Jun10_EntireReport.pdf?sfvrsn=0.
35. Prabhu M, McQuaid-Hanson E, Hopp S, et al. A Shared Decision-Making Intervention to Guide Opioid Prescribing After Cesarean Delivery. Obstet Gynecol. 2017;130(1):42-46. doi:10.1097/AOG.0000000000002094.
36. Instructions for Authors. The Journal of the American Medical Association. 2019. Accessed June 14, 2021. https://jamanetwork.com/journals/jama/pages/instructions-for-authors.
37. Chapter 8: Assessing risk of bias in included studies. Cochrane Handbook for Systematic Reviews of Interventions: Version 5.1.0. The Cochrane Collaboration. 2011. Accessed June 14, 2021. https://handbook-5-1.cochrane.org/chapter_8/8_assessing_risk_of_bias_in_included_studies.htm.
38. Elwyn G, Frosch DL, Kobrin S. Implementing shared decision-making: consider all the consequences. Implement Sci. 2016;11:114. doi:10.1186/s13012-016-0480-9.
39. CRD’s guidance for undertaking reviews in health care. Centre for Reviews and Dissemination. Accessed January 14, 2022. https://www.york.ac.uk/media/crd/Systematic_Reviews.pdf.
40. Cox CE, Lewis CL, Hanson LC, et al. Development and pilot testing of a decision aid for surrogates of patients with prolonged mechanical ventilation. Crit Care Med. 2012;40(8):2327-2334. doi:10.1097/CCM.0b013e3182536a63.
41. Stamm AW, Banerji JS, Wolff EM, et al. A decision aid versus shared decision making for prostate cancer screening: results of a randomized, controlled trial. Can J Urol. 2017;24(4):8910-8917.
42. Lindly OJ, Zuckerman KE, Mistry KB. Clarifying the Predictive Value of Family-Centered Care and Shared Decision Making for Pediatric Healthcare Outcomes Using the Medical Expenditure Panel Survey. Health Serv Res. 2017;52(1):313-345. doi:10.1111/1475-6773.12488.
43. Carson SS, Cox CE, Wallenstein S, et al. Effect of palliative care-led meetings for families of patients with chronic critical illness: a randomized clinical trial. JAMA. 2016;316(1):51-62. doi:10.1001/jama.2016.8474
44. Hess EP, Knoedler MA, Shah ND, et al. The chest pain choice decision aid: a randomized trial. Circ Cardiovasc Qual Outcomes. 2012;5(3):251-259. doi:10.1161/CIRCOUTCOMES.111.964791.
45. Ibrahim SA, Blum M, Lee GC, et al. Effect of a Decision Aid on Access to Total Knee Replacement for Black Patients With Osteoarthritis of the Knee: A Randomized Clinical Trial. JAMA Surg. 2017;152(1):e164225. doi:10.1001/jamasurg.2016.4225.
46. Watts BV, Schnurr PP, Zayed M, Young-Xu Y, Stender P, Llewellyn-Thomas H. A randomized controlled clinical trial of a patient decision aid for posttraumatic stress disorder. Psychiatr Serv. 2015;66(2):149-154. doi:10.1176/appi.ps.201400062.
47. Volandes AE, Paasche-Orlow MK, Davis AD, Eubanks R, El-Jawahri A, Seitz R. Use of video decision aids to promote advance care planning in Hilo, Hawai’i. J Gen Intern Med. 2016;31(9):1035-1040. doi:10.1007/s11606-016-3730-2.
48. Arterburn D, Wellman R, Westbrook EO, et al. Decision aids for benign prostatic hyperplasia and prostate cancer. Am J Manag Care. 2015;21(2):e130-e140.
49. Gill BC, Ulchaker JC. Costs of Managing Benign Prostatic Hyperplasia in the Office and Operating Room. Curr Urol Rep. 2018;19(9):72. doi:10.1007/s11934-018-0822-z
50. APM Measurement: Progress of Alternative Payment Models. 2019 Methodology and Results Report. Health Care Payment Learning and Action Network. 2019. Accessed June 14, 2021. https://hcp-lan.org/workproducts/apm-methodology-2019.pdf.
51. US Preventive Services Task Force, Davidson KW, Mangione CM, et al. Collaboration and Shared Decision-Making Between Patients and Clinicians in Preventive Health Care Decisions and US Preventive Services Task Force Recommendations. JAMA. 2022;327(12):1171-1176. doi:10.1001/jama.2022.3267
52. Explore Measures and Activities. Centers for Medicare and Medicaid Services. Quality Payment Program. 2020. Accessed June 14, 2021. https://qpp.cms.gov/mips/explore-measures?tab=qualityMeasures&py=2020#measures.
53. Medicare Program; CY 2021 Payment Policies Under the Physician Fee Schedule and Other Changes to Part B Payment Policies; Medicare Shared Savings Program Requirements; Medicaid Promoting Interoperability Program Requirements for Eligible Professionals; Quality Payment Program; Coverage of Opioid Use Disorder Services Furnished by Opioid Treatment Programs; Medicare Enrollment of Opioid Treatment Programs; Electronic Prescribing for Controlled Substances for a Covered Part D Drug Under a Prescription Drug Plan or an MA-PD Plan; Payment for Office/Outpatient Evaluation and Management Services; Hospital IQR Program; Establish New Code Categories; and Medicare Diabetes Prevention Program (MDPP) Expanded Model Emergency Policy. Federal Register. 2020. Accessed June 14, 2021. https://www.federalregister.gov/documents/2020/08/17/2020-17127/medicare-program-cy-2021-payment-policies-under-the-physician-fee-schedule-and-other-changes-to-part.
54. Patient decision aids (PDAs). Washington State Health Care Authority. Accessed June 14, 2021. https://www.hca.wa.gov/about-hca/making-informed-health-care-decisions/patient-decision-aids-pdas.
55. Terrell G. Value-Based Care: Promote the Triple Aim. AMA Ed Hub. 2016. Accessed June 14, 2021. https://edhub.ama-assn.org/steps-forward/module/2702555.
56. Heath S. Value-Based Care Drives Preventive Care, Care Management. PatientEngagementHIT. 2019. Accessed June 14, 2021. https://patientengagementhit.com/news/value-based-care-drives-preventive-care-care-management.
57. Chapter 12: Synthesizing and presenting findings using other methods. Cochrane Training. Accessed January 14, 2022. https://training.cochrane.org/handbook/current/chapter-12.
58. Bomhof-Roordink H, Gartner FR, Stiggelbout AM, Pieterse AH. Key components of shared decision making models: a systematic review. BMJ Open. 2019;9(12):1-11. doi: 10.1136/bmjopen-2019-031763.



