


The Impact of Social Determinants of Health Beyond Race on Survival in Metastatic Prostate Cancer: A Systematic Literature Review
Abstract
The impact of social determinants of health (SDOH) has become a focus of cancer research, including metastatic prostate cancer (mPC), as patients with mPC face a particularly poor prognosis. Our systematic literature review (SLR) summarized the current evidence relating to SDOH and survival in mPC. Embase, MEDLINE, and Cochrane Database were searched from January 2012 to July 2022 using Ovid. Key congresses were also searched. From this SLR, we previously reported on the association between race and survival. Thus, here we report on SDOH beyond race. The majority of the 22 identified studies reported significant differences in survival by income, socioeconomic status (SES), marital status, treatment facility type, insurance status, and location. For education, however, most studies reported no association with survival. Higher income and SES, private insurance, academic facility type, and being married were associated with better survival. Although surprisingly few studies were identified, our findings suggest that disparities in mPC survival by SDOH beyond race remain. Further research is needed to better understand the reasons for these associations to improve survival for all mPC patients.
Background
Prostate cancer (PC) accounts for 7% of newly diagnosed cancers in men globally and is the fifth most common cause of male cancer mortality.1,2 Incidence rates of PC vary greatly worldwide, ranging from 6.3 to 83.4 per 100 000 people, with higher incidences seen in nations with higher life expectancies and gross domestic products, such as the US and UK.2,3 Although recent years have seen a decline in overall cancer death rates worldwide,4 socioeconomic inequalities in cancer mortality continue to increase,5-7 and patients with metastatic prostate cancer (mPC) face a particularly poor prognosis.8 In an effort to mitigate inequalities in cancer outcomes, social determinants of health (SDOH), or the nonmedical factors that can influence health outcomes, are increasingly at the forefront of cancer research, including PC.5,9 Understanding the impact of SDOH on survival in mPC presents an important opportunity for improving patient outcomes.
Race is one SDOH that has been extensively investigated in mPC, including in a prior report by our team.10 However, recent evidence has shown that SDOH beyond race also contribute to disparities in mPC survival.11 Currently, available reviews examining the impact of non-race SDOH on PC outcomes are narrative in nature or focus on PC generally, as opposed to mPC.12-16 The diverse characteristics of PC, which can vary from indolent to aggressive, may lead to conflicting conclusions. Hence, research focusing on a more narrowly defined group of patients, all with potentially fatal disease (ie, those with mPC), is required.17 We conducted a systematic literature review (SLR) to identify and summarize evidence on the relationships between SDOH (defined herein as income, socioeconomic status [SES], marital status, type of treatment facility, insurance status, location, and education) and survival outcomes in patients with mPC.
Methods
Literature Search
The SLR adhered to the Cochrane guidelines18 and the Preferred Reporting Items for Systematic Review and Meta- Analysis (PRISMA) statement.19,20 Study eligibility criteria followed the population, intervention, comparator, outcome, study design (PICOS) framework (Supplementary Table 1).18 A medical information specialist designed and implemented the search strategy (Supplementary Table 2), which was peer reviewed using the Peer Review of Electronic Search Strategies (PRESS) checklist.21 Embase, MEDLINE (Epub Ahead of Print, In-Process & Other Non-Indexed Citations, and Daily), and the Cochrane Database of Systematic Reviews were searched using the Ovid platform on July 7, 2022. Retrieval was limited to full-text studies published in English from 2012 onward, which was considered by expert clinical input to reflect the modern mPC treatment landscape. Conference abstracts from 2019 onward were eligible for inclusion to capture studies not yet published as full texts. A supplemental search for relevant conference abstracts from key congresses was also conducted (Supplementary Table 3). The full study protocol was registered with PROSPERO international prospective register of systematic reviews (registration number CRD42022350888).
Study Selection and Data Synthesis
The titles and abstracts of retrieved records were screened for inclusion and then assessed in full-text form against the eligibility criteria (Supplementary Table 1) by two independent reviewers using a systematic literature review software.22 A third independent reviewer was consulted when consensus could not be achieved. Although the search strategy was designed to identify studies reporting on the impact of SDOH (including race) on a variety of clinical outcomes in patients with mPC, the focus of the present article was studies reporting on income, SES, marital status, type of treatment facility, insurance status, location, and education on survival outcomes. Data extraction and quality assessment was performed by a single reviewer and confirmed by a second reviewer. A standardized data extraction form in a spreadsheet-based software was used. Clinical judgment was employed by an experienced prostate cancer clinician and researcher (SJF) to assess the castration sensitivity status of patient populations (metastatic castration-sensitive prostate cancer [mCSPC], metastatic castration-resistant prostate cancer [mCRPC], or mixed [both mCSPC and mCRPC]) when not explicitly stated.
Quality Assessment
The Newcastle-Ottawa Quality Assessment Scales for cohort studies were used to evaluate the study quality of full-text publications.23 Studies were given a total score between 0 and 9 and classified as low quality/high risk of bias (<5), moderate quality (5 to ≥7), or high quality/low risk of bias (≥7).24
Results
Overview of Included Studies
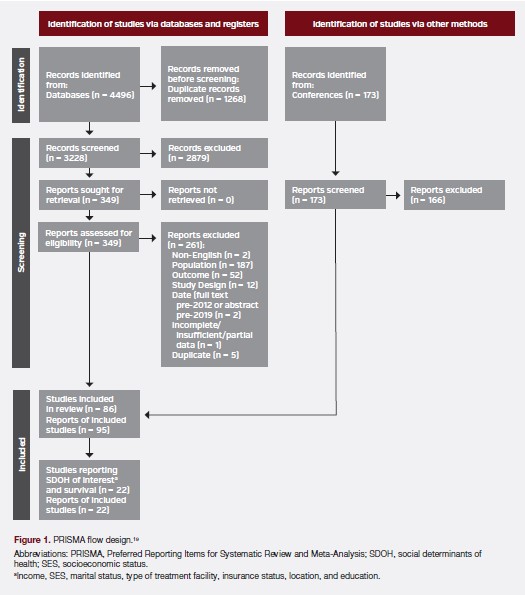
Database searches identified 3228 records after deduplication, with an additional 173 conference abstracts identified in the supplemental congress search. Following screening, 22 records (20 full texts25-44 and 2 conference abstracts45,46) representing 22 unique studies reporting on the impact of SDOH beyond race on survival outcomes were included (Figure 1). See Supplementary Table 4 for the list of included citations.
Study Characteristics
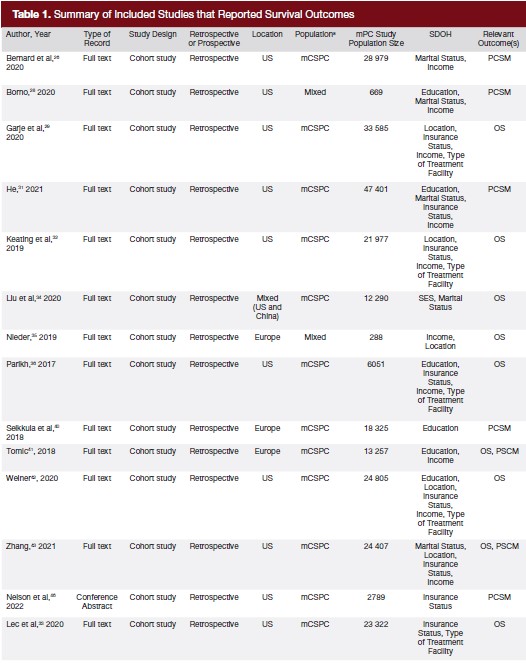
Characteristics of the 22 included studies are summarized in Table 1. All were retrospective cohort studies25-46 and reported on mCSPC (n = 18)25-27,29-34,36,37,40-46 or mixed mCSPC/mCRPC populations (n = 4).28,35,38,39 Study locations included the US (n = 17),26-33,36-39,42-46 Europe (n = 4),25,35,40,41 and one study conducted in both the US and China.34 Studies investigated income (n = 13),26-29,31,32,35,36,39,41-43,45 SES (n = 2),25,34 marital status (n = 8),26-28,30,31,34,43,44 type of treatment facility (n = 8),29,32,33,36- 39,42 insurance status (n = 12),29,31-33,36-39,42,43,45,46 location (n = 8),27,29,32,35,38,39,42,43 and education (n = 7).27,28,31,36,40-42 Some studies reported results for multiple SDOH. A total of 14 studies reported results for overall survival (OS) only,25,29,30,32-39,42,44,45 6 reported on PC-specific mortality (PCSM) only,26-28,31,40,46 and 2 reported both outcomes.41,43
Assessment of Study Quality
Overall, 95% of studies (19 out of 20) published as full-text articles were determined to be of high quality/low risk of bias (score ≥7) (Supplementary Table 5).24,25-34,36-44
SDOH Results
The results of each SDOH are summarized in a separate subsection below. The described results reflect findings for which two or more applicable studies reported a specific comparison (eg, OS between private insurance vs uninsured, PCSM between married vs unmarried, etc). Studies must also have allowed for the impact of a single SDOH to be discerned (eg, SDOH X must have been considered as a single variable, rather than as a composite of SDOH X + SDOH Y). Results not meeting these criteria were uncommon but were included in Supplementary Table 6 for completeness.
Income
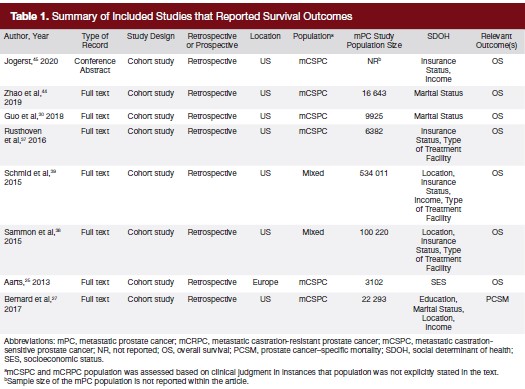
Among the studies that reported on income and OS (Figure 2A), the majority (7 of 8 studies) reported that higher income was associated with improved OS,29,32,36,41-43,45 whereas only one study found no significant differences between income levels.35,39 Regarding PCSM, 3 of 6 studies reported that higher income was associated with improved PCSM31,41,43 while the other three found no association.26-28
Socioeconomic Status
Both studies (2 of 2 studies) investigating the impact of SES reported that higher SES was associated with improved OS (Figure 2B).25,34 No studies investigating the association between SES and PCSM were identified.
Marital Status
Being married was associated with improved OS (4 of 4 studies)30,34,43,44 and improved PCSM (3 of 4 studies)26,27,43 compared to unmarried patients (Figure 2C).
Type of Treatment Facility
Most studies (4 of 7 studies) reported that treatment in an academic facility was associated with improved OS compared to nonacademic and/or community facilities (Figure 2D).29,32,37,42 Additionally, no association in OS was found between patients treated in a comprehensive facility (ie, defined as those that treat 500 or more cancer patients each year)47 compared to a community facility, in 2 of 2 studies.36,42 No studies investigating the association between treatment facility and PCSM were identified. Specific definitions used for the types of treatment facilities compared are outlined in Supplementary Table 7 and Supplementary Table 8.
Insurance Status
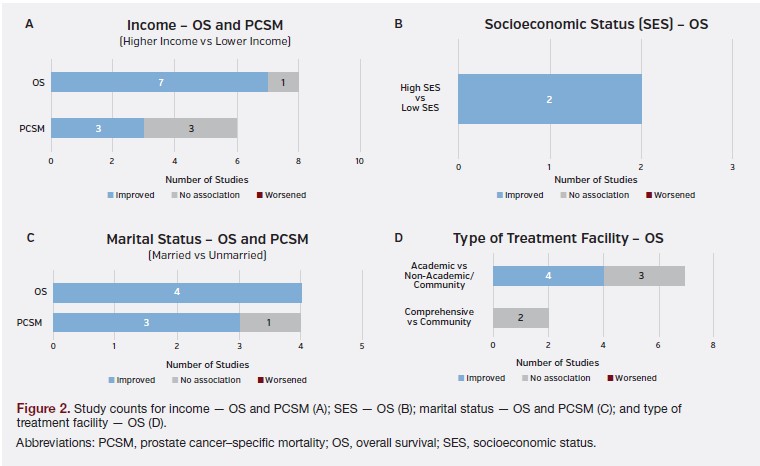
Within the studies that reported on insurance status and OS (Figure 3A), five categories were reported: private insurance, Medicare, Medicaid, uninsured, and insured generally (any form of insurance). Medicare is federal health insurance in the US for patients 65 years of age or older as well as those with certain disabilities or conditions, while Medicaid is joint federal and state insurance administered by each state in the US that covers medical costs for certain patients with limited income and/or resources. Although the federal government sets general rules for state Medicaid programs, variation in eligibility requirements and benefits can exist between states.48 All studies were US-based, and all but one adjusted for various sociodemographic factors in their analyses, including age.
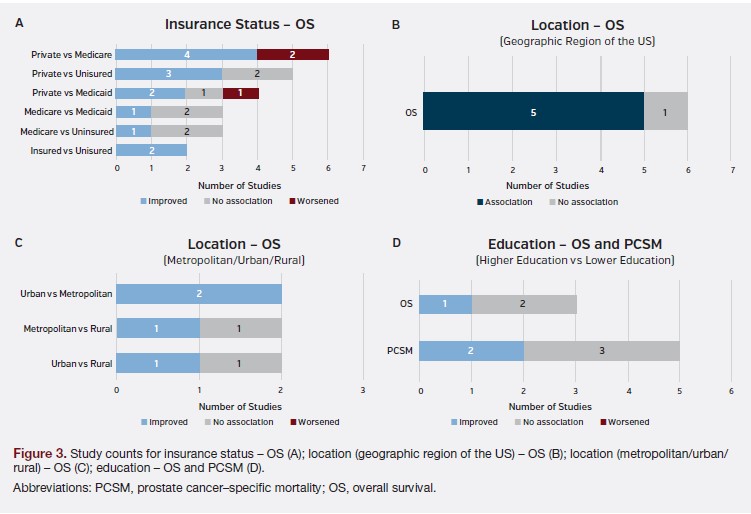
For private insurance, the majority of studies reported that patients with private insurance had improved OS compared to those with Medicare (4 of 6 studies)29,37,42,45 and those who were uninsured (3 of 5 studies).29,39,45 Findings for private vs Medicaid insurance, however, were conflicting: Two studies concluded that patients with private insurance had improved OS compared to patients with Medicaid,29,45 one study found the opposite,39 and one study found no difference in survival.37
For Medicare, the majority of studies reported no difference in OS between patients with Medicare vs Medicaid (2 of 3 studies),33,38 as well as between patients with Medicare vs those who were uninsured (2 of 3 studies).33,36 None of the studies provided additional information regarding the specifications/nuances of the different insurance types considered (eg, coverage, requirements, benefits, eligibility, etc) or whether patients were dually insured.
Lastly, both studies that compared patients with any form of insurance vs uninsured patients found that insured patients had improved OS.32,43
With respect to PCSM, no two identified studies reported common comparisons across the various categories of insurance status (Supplementary Table 6).
Location
Six studies compared OS in patients with mPC across different geographical regions or locations within the US (eg, Pacific region, middle Atlantic region, mountain Pacific region, southern region, eastern region, etc). Although the regions that were compared between studies varied, significant differences in OS across geographic regions of the US were found in the majority of studies (5 out of 6 studies) (Figure 3B).29,32,38,39,42
Additionally, a few studies were identified that assessed the impact of metropolitan, urban, or rural location on OS, with variable findings (Figure 3C). Two studies compared rural and urban locations to metropolitan locations, using data from the NCDB.29,32,49 See Supplementary Table 9 for specific definitions based on population size and location. In both studies, urban location was found to be associated with improved OS compared to metropolitan location.29,32 For the rural and metropolitan location comparison, one study found no association,29 while the other concluded that rural location was associated with improved OS compared to metropolitan.32
An additional two studies compared only urban and rural locations,38,39 with both using data from a national sample created by the Agency for Healthcare Research and Quality.50,51 See Supplementary Table 10 for specific definitions based on population density and location. One study found that urban location was associated with improved OS,39 while the other study found no significant differences.38
Regarding PCSM, no two identified studies reported common comparisons across the various categories of location (Supplementary Table 6).
Education
Of the three studies that reported on education level and OS, one study reported that higher education was associated with improved OS,41 while the two remaining studies reported no association (Figure 3D).36,42 Similarly for PCSM, 2 of 5 studies found that higher education was associated with improved PCSM40,41; however, the remaining three studies reported no association.27,28,31
Discussion
The aim of this review was to identify and summarize recent studies investigating the relationship between SDOH beyond race (defined herein as income, SES, marital status, type of treatment facility, insurance status, location, and education) and survival outcomes in patients with mPC. A total of 22 studies were identified, highlighting a dearth of research and evidence in this area. The majority of studies reported significant differences in survival by key SDOH, including income, SES, marital status, type of treatment facility, insurance status, and location, with the exception of education where the majority of studies reported no association with survival outcomes. Higher income and SES, private insurance, treatment in an academic facility, and being married were found to be associated with a survival benefit in patients with mPC.
The overall finding of this SLR, that SDOH are associated with disparities in survival for patients with mPC, is generally consistent with the literature of PC more broadly and oncology in general. The trends and relationships on survival outcomes in mPC seen herein with income/SES, marital status, and location align with previous narrative reviews and reports in PC.12,14,52,53 The finding that survival outcomes are improved when patients are treated at an academic facility is consistent with findings in other oncology areas.54,55 For insurance status, improved outcomes with private insurance have also been previously discussed in the oncology literature, with evidence suggesting that some of this benefit is attributable to earlier detection and treatment.56
With respect to education, however, the inconclusive findings from the current SLR differ with prior reports in the literature. Notably, a recent large-scale study reported that the survival disparity between patients with higher and lower education has been increasing over time for patients with common cancers (including prostate).57 Although inconclusive results were found in the present SLR, education is closely linked to other SDOH examined, such as SES and income, where the majority of studies reported significant survival differences. In fact, SES measures often encompass income and educational attainment, among other factors.58 Prior studies in cancer generally, as well as prostate cancer, have reported that both lower education and income or SES are associated with higher risk of mortality.59,60 A large US study conducted by Singh and Jemal found that men with low education and income were at an increased risk of all-cancer mortality and prostate cancer–specific mortality.59 Similarly, both lower neighborhood SES and lower education were found to be significantly associated with a greater risk of death in a large recent study of prostate cancer patients.60 It is important to note, however, that none of these analyses were specific to the metastatic setting. Further research may be required to clarify this relationship between education and mortality, as well as how this relationship correlates with other related SDOH, such as income and SES.
Our SLR identified several important data gaps. Compared to 54 studies previously identified by our team that reported on race and survival,10 the present analysis identified only 22 studies that reported on SDOH other than race. Thus, most research conducted to date on the impact of SDOH on survival outcomes in mPC has focused on race, with much less attention paid to other important SDOH. Consequently, several SDOH were investigated in only 8 or fewer studies, with very few studies reporting many comparisons (eg, high vs low SES, comprehensive vs community treatment facility, Medicare vs uninsured, etc), making it difficult to identify trends and conclusions. For example, the comparison between urban and rural location was only reported in two studies, with conflicting results, making it unfeasible to discern an overall conclusion or finding for this comparison. Additionally, for 5 of the 7 SDOH of interest, there was insufficient data to assess the impact of these SDOH on PCSM, indicating a paucity of information on PCSM compared to OS. Further research in this area of other SDOH is needed, as these factors can contribute to disparities in PC outcomes as well as imparting influences on their own.13-15
In addition to the relatively small number of studies, there was also substantial heterogeneity in the reference groups and specific categories used to define the various SDOH across the included studies, especially for location (eg, urban/rural/metropolitan), type of treatment facility (academic/teaching facility, community facility, integrated network facility, etc), education (eg, with vs without high school diploma, basic vs higher education, etc), and income (eg, ≥$66 610 vs <$66 610, ≥$68 000 vs <$68 000, etc). For income and education, we simplified and interpreted categories as “high vs low” to enable comparison of findings across studies. Other sources of heterogeneity also included the use of different statistical tests and reporting methodologies, which prevented comparisons of the magnitude of the observed relationships. These factors made it challenging to directly compare findings across studies and points to the need for a more consistent classification and methodology for exploring SDOH in the mPC setting. Furthermore, no identified studies were conducted in an mCRPC population alone, and very few were conducted outside the US, thus highlighting the need for further research on SDOH on survival outcomes in more advanced mPC populations and in ex-US regions.
Several strengths and limitations of this review should be noted. The present SLR provides a comprehensive and thorough assessment of the existing research, concentrating specifically on mPC, as opposed to previous reviews that examined the impact of SDOH on PC as a whole. To incorporate and reflect the growing body of evidence, the review included full-text articles focused on real-world evidence and published within the past 10 years. In an effort to incorporate the most recent research in the field, conference abstracts were also included; however, they often only report limited information. As only articles published in English were included, the findings of non-English articles are not accounted for in our findings. Additionally, although the use of clinical judgment to assess the castration sensitivity status of patient populations when necessary is inherently subjective, this provided unique insight into the populations assessed in the available literature. Lastly, significant heterogeneity was observed between included studies and only qualitative findings are presented within this review. Future studies that quantitatively evaluate the impact of SDOH and survival to better understand and identify the relationships and disparities are needed.
Conclusion
In summary, this study provided a thorough systematic assessment of the impact of SDOH beyond race on survival in the mPC population. Results from this SLR reveal that disparities in mPC survival outcomes by key SDOH continue to exist. Higher income and SES, private insurance, treatment in an academic facility, and being married were associated with a survival advantage for patients with mPC. Despite increased attention on SDOH in recent years, surprisingly few studies investigating SDOH in this area were identified, highlighting the need for additional research to further explore the impacts of SDOH on outcomes and access to care in mPC. Continued focused efforts are needed to further understand these disparities and expand the potential survival benefits to all patients.
This article has supplementary material, which can be accessed at this link.
Author Information
Authors: Stephen J. Freedland, MD1,2; Imtiaz A. Samjoo, MSc, PhD3; Emily Rosta, MSc3; Austin Lansing, MSc3; Alexandra Hall, MPH3; Manvir Rai, BSc3; Alexander Niyazov, PharmD, MPH4; Jonathan L. Nazari, PharmD4; Bhakti Arondekar, PhD, MBA5
Affiliations: 1Division of Urology, Department of Surgery, Cedars-Sinai Medical Center, Los Angeles, CA; 2Urology Section, Durham VA Medical Center, Durham, NC; 3EVERSANA, Burlington, Ontario, Canada; 4Pfizer, Inc, New York, NY; 5Pfizer, Inc, Collegeville, PA.
Address correspondence to:
Stephen J. Freedland
8635 West 3rd Street Suite 1070W
Los Angeles, CA 90048
Email: stephen.freedland@cshs.org
Acknowledgements: The authors thank Kerise Clarke, Amrita Debnath, and Joanna Bielecki for their assistance with the literature review. All were employed by EVERSANA, Canada.
Disclosures: S.J.F. reported serving as a consultant for Pfizer, Astellas, Janssen, Bayer, Merck, AstraZeneca, Myovant, and Sanofi; and serving as a speaker for AstraZeneca and Sanofi. I.A.S., E.R., A.L., A.H., and M.R. reported being employees of EVERSANA, Canada, which was a paid consultant to Pfizer in connection with the development of this manuscript. A.N. and B.A. reported being employees of Pfizer and owning Pfizer stock. J.L.N. reported being an employee of the University of Illinois Chicago, which was a paid contractor to Pfizer in connection with the development of this manuscript through the 2021-2023 University of Illinois at Chicago- Pfizer Fellowship.
References
1. Barsouk A, Padala SA, Vakiti A, et al. Epidemiology, staging and management of prostate cancer. Med Sci (Basel). 2020;8(3). doi:10.3390/medsci8030028
2. Rebello RJ, Oing C, Knudsen KE, et al. Prostate cancer. Nat Rev Dis Primers. 2021;7(1):9. doi:10.1038/s41572-020-00243-0
3. Giona S. The Epidemiology of Prostate Cancer. In: Bott SRJ, Ng KL, eds. Prostate Cancer. Exon Publications; 2021.
4. Hashim D, Boffetta P, La Vecchia C, et al. The global decrease in cancer mortality: trends and disparities. Ann Oncol. 2016;27(5):926-33. doi:10.1093/annonc/mdw027
5. Alcaraz KI, Wiedt TL, Daniels EC, Yabroff KR, Guerra CE, Wender RC. Understanding and addressing social determinants to advance cancer health equity in the United States: a blueprint for practice, research, and policy. CA Cancer J Clin. 2020;70(1):31-46. doi: 10.3322/caac.21586
6. Williams F, Zoellner N, Hovmand PS. Understanding global cancer disparities: the role of social determinants from system dynamics perspective. Transdiscipl J Eng Sci. 2016;7. doi:10.22545/2016/00072
7. Vaccarella S, Georges D, Bray F, et al. Socioeconomic inequalities in cancer mortality between and within countries in Europe: a population-based study. Lancet Reg Health Eur. Feb 2023;25:100551. doi:10.1016/j.lanepe.2022.100551
8. National Cancer Institute Cancer Stat Facts: Prostate Cancer. National Cancer Institute. 2022. https://seer.cancer.gov/statfacts/html/prost.html
9. Centers for Disease Control and Prevention. Social Determinants of Health at CDC. Updated December 8, 2022. Accessed March 7, 2023. https://www.cdc.gov/about/ sdoh/index.html
10. Freedland SJ, Niyazov A, Nazari J, et al. Social determinants of health (SDOH) and survival among patients with metastatic prostate cancer (mPC): A systematic literature review (SLR). J Clin Oncol. 2023;41(6_suppl):25-25. doi:10.1200/JCO.2023.41.6_ suppl.25
11. Vince RA Jr, Jiang R, Bank M, et al. Evaluation of social determinants of health and prostate cancer outcomes among Black and White patients: a systematic review and meta-analysis. JAMA Netw Open. 2023;6(1):e2250416. doi:10.1001/jamanetworkopen.2022.50416
12. Cackowski FC, Mahal B, Heath EI, Carthon B. Evolution of Disparities in Prostate Cancer Treatment: Is This a New Normal? American Society of Clinical Oncology Educational Book. 2021;41:1-12. doi:10.1200/edbk_321195
13. Hinata N, Fujisawa M. Racial differences in prostate cancer characteristics and cancer-specific mortality: an overview. World J Mens Health. 2022;40(2):217-227. doi:10.5534/wjmh.210070
14. Coughlin SS. A review of social determinants of prostate cancer risk, stage, and survival. Prostate Int. 2020;8(2):49-54. doi:10.1016/j.prnil.2019.08.001
15. Lillard Jr JW, Moses KA, Mahal BA, George DJ. Racial disparities in Black men with prostate cancer: a literature review. Cancer. 2022;128(21):3787-3795. doi:10.1002/ cncr.34433
16. Mahal BA, Gerke T, Awasthi S, et al. Prostate cancer racial disparities: a systematic review by the prostate cancer foundation panel. Eur Urol Oncol. 2021;5(1):18-29. doi: 10.1016/j.euo.2021.07.006
17. Giovannucci E, Liu Y, Platz EA, Stampfer MJ, Willett WC. Risk factors for prostate cancer incidence and progression in the health professionals follow-up study. Int J Cancer. 2007;121(7):1571-1578. doi:10.1002/ijc.22788
18. Higgins JPT TJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA eds. Cochrane handbook for systematic reviews of interventions version 6.2. Cochrane. Updated August 2023. Published online 2021.
19. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
20. Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. doi:10.1136/bmj.n160
21. McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. doi:10.1016/j.jclinepi.2016.01.021
22. DistillerSR. DistillerSR Inc; 2011. Accessed September 21, 2022. https://www.distillersr.com/products/distillersr-systematic-review-software
23. GA Wells BS, D O’Connell, J Peterson, V Welch, M Losos, P Tugwell. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Accessed September 21, 2022. https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
24. Pal R, Banerjee M, Yadav U, Bhattacharjee S. Statin use and clinical outcomes in patients with COVID-19: an updated systematic review and meta-analysis. Postgrad Med J. 2022;98(1159):354-359. doi:10.1136/postgradmedj-2020-139172
25. Aarts MJ, Koldewijn EL, Poortmans PM, Coebergh JWW, Louwman M. The impact of socioeconomic status on prostate cancer treatment and survival in the southern Netherlands. Urology. 2013;81(3):593-599. Comment in: Urology. 2013;81(3):600- 601. doi:10.1016/j.urology.2012.11.011
26. Bernard B, Burnett C, Sweeney CJ, Rider JR, Sridhar SS. Impact of age at diagnosis of de novo metastatic prostate cancer on survival. Cancer. 2020;126(5):986-993. doi:10.1002/cncr.32630
27. Bernard B, Muralidhar V, Chen YH, et al. Impact of ethnicity on the outcome of men with metastatic, hormone-sensitive prostate cancer. Cancer. 2017;123(9):1536- 1544. doi:10.1002/cncr.30503
28. Borno HT, Cowan JE, Zhao S, Broering JM, Carroll PR, Ryan CJ. Examining initial treatment and survival among men with metastatic prostate cancer: An analysis from the CaPSURE registry. Urol Oncol. 2020;38(10):793.e1-793.e11. doi:10.1016/j.urolonc.2020.07.012
29. Garje R, Chennamadhavuni A, Mott SL, et al. Utilization and outcomes of surgical castration in comparison to medical castration in metastatic prostate cancer. Clin Genitourin Cancer. 2020;18(2):e157-e166. doi:10.1016/j.clgc.2019.09.020
30. Guo X, Zhang C, Guo Q, et al. The homogeneous and heterogeneous risk factors for the morbidity and prognosis of bone metastasis in patients with prostate cancer. Cancer Manag Res. 2018;10:1639-1646. doi:10.2147/CMAR.S168579
31. He H, Han D, Xu F, Lyu J. How socioeconomic and clinical factors impact prostate-cancer-specific and other-cause mortality in prostate cancer stratified by clinical stage: competing-risk analysis. Prostate. 2021;82(4):415-424. doi:10.1002/pros.24287
32. Keating MJ, Giscombe L, Tannous T, et al. Age-dependent overall survival benefit of androgen deprivation therapy for metastatic prostate cancer. J Oncol Pharm Pract. 2019;25(8):1927-1932. doi:10.1177/1078155219835597
33. Lec PM, Lenis AT, Brisbane W, et al. Trends in palliative care interventions among patients with advanced bladder, prostate, or kidney cancer: a retrospective cohort study. Urol Oncol. 2020;38(11):854. doi:10.1016/j.urolonc.2020.04.029
34. Liu D, Kuai Y, Zhu R, et al. Prognosis of prostate cancer and bone metastasis pattern of patients: a SEER-based study and a local hospital based study from China. Sci Rep. 2020;10(1) doi:10.1038/s41598-020-64073-6
35. Nieder C, Dalhaug A, Haukland E, Norum J. Management of patients with metastatic prostate cancer (mPC) in a rural part of North Norway with a scattered population: does living near the department of oncology translate into a different pattern of care and survival? Int J Circumpolar Health. 2019;78(1). doi:10.1080/22423982.2 019.1620086
36. Parikh RR, Byun J, Goyal S, Kim IY. Local therapy improves overall survival in patients with newly diagnosed metastatic prostate cancer. Prostate. 2017;77(6):559-572. doi:10.1002/pros.23294
37. Rusthoven CG, Jones BL, Flaig TW, et al. Improved survival with prostate radiation in addition to androgen deprivation therapy for men with newly diagnosed metastatic prostate cancer. J Clin Oncol. 2016;34(24):2835-2842. doi:10.1200/ JCO.2016.67.4788
38. Sammon JD, McKay RR, Kim SP, et al. Burden of hospital admissions and utilization of hospice care in metastatic prostate cancer patients. Urology. 2015;85(2):343-350. doi:10.1016/j.urology.2014.09.053
39. Schmid M, Ghani KR, Choueiri TK, et al. An evaluation of the ‘weekend effect’ in patients admitted with metastatic prostate cancer. BJU Int. 2015;116(6):911-919. doi:10.1111/bju.12891
40. Seikkula HA, Kaipia AJ, Ryynanen H, et al. The impact of socioeconomic status on stage specific prostate cancer survival and mortality before and after introduction of PSA test in Finland. Int J Cancer. 2018;142(5):891-898. doi:10.1002/ijc.31109
41. Tomic K, Ventimiglia E, Robinson D, Haggstrom C, Lambe M, Stattin P. Socioeconomic status and diagnosis, treatment, and mortality in men with prostate cancer. Nationwide population-based study. Int J Cancer. 2018;142(12):2478-2484. doi:10.1002/ijc.31272
42. Weiner AB, Cohen JE, DeLancey JO, Schaeffer EM, Auffenberg GB. Surgical versus medical castration for metastatic prostate cancer: use and overall survival in a national cohort. J Urol. 2020;203(5):933-939. doi:10.1097/JU.0000000000000684
43. Zhang AC, Rasul R, Golden A, Feuerstein MA. Incidence and mortality trends of metastatic prostate cancer: surveillance, epidemiology, and end results database analysis. Can Urol Assoc J. 2021;15(12):E637-E643. doi:10.5489/cuaj.7173
44. Zhao F, Wang J, Chen M, et al. Sites of synchronous distant metastases and prognosis in prostate cancer patients with bone metastases at initial diagnosis: a population-based study of 16,643 patients. Clin Transl Med. 2019;8(1):30. doi:10.1186/ s40169-019-0247-4
45. Jogerst K, Ali-Mucheru M, Chang Y, et al. Disparities in stage IV cancer outcomes: treatment differences and association with overall survival. In: Society of Surgical Oncology SSO 2020 - International Conference on Surgical Cancer Care. Ann Surg Oncol. 2020;27(suppl 1):S93. doi:10.1245/s10434-020-08278-z
46. Nelson TJ, Courtney PT, Klebaner D, et al. Association between health-care system and prostate cancer mortality for African American men with localized and metastatic prostate cancer. J Clin Oncol. 2022;40(suppl 6):27. 2022 ASCO Genitourinary Cancers Symposium. Online. doi:10.1200/JCO.2022.40.6_suppl.027
47. American College of Surgeons. About Cancer Program Categories. Updated NR. Accessed March 22, 2023. https://www.facs.org/quality-programs/cancer-programs/ commission-on-cancer/coc-accreditation/categories/
48. U.S. Department of Health and Human Services. What’s the difference between Medicare and Medicaid? Updated December 8, 2022. Accessed March 10, 2023. https://www.hhs.gov/answers/medicare-and-medicaid/what-is-the-difference-between-medicare-medicaid/index.html
49. American College of Surgeons. National Cancer Database Participant User File: 2020 Data Dictionary. 2022:391. Accessed March 15, 2023. https://www.facs.org/media/ brilfbgu/puf-2020-data-dictionary.pdf
50. Agency for Healthcare Research and Quality. National Inpatient Sample Description of Data Elements. Updated September 16, 2022. Accessed March 15, 2023. https:// hcup-us.ahrq.gov/db/nation/nis/nisdde.jsp
51. United States Census Bureau. 2000 Census Urban and Rural Classification. Updated December 16, 2021. Accessed March 15, 2023. https://www.census.gov/programs-surveys/geography/guidance/geo-areas/urban-rural/2000-urban-rural.html
52. Tyson MD, Andrews PE, Etzioni DA, et al. Marital status and prostate cancer outcomes. Can J Urol. 2013;20(2):6702-6706.
53. Afshar N, English DR, Milne RL. Rural-urban residence and cancer survival in high-income countries: a systematic review. Cancer. 2019;125(13):2172-2184. doi:10.1002/ cncr.32073
54. Merritt RE, Abdel-Rasoul M, Fitzgerald M, D’Souza DM, Kneuertz PJ. The academic facility type is associated with improved overall survival for early-stage lung cancer. Ann Thorac Surg. 2021;111(1):261-268. doi:10.1016/j.athoracsur.2020.05.051
55. Carey RM, Fathy R, Shah RR, et al. Association of type of treatment facility with overall survival after a diagnosis of head and neck cancer. JAMA Netw Open. 2020;3(1):e1919697-e1919697. doi:10.1001/jamanetworkopen.2019.19697
56. Cole AP, Lu C, Krimphove MJ, et al. Comparing the association between insurance and mortality in ovarian, pancreatic, lung, colorectal, prostate, and breast cancers. J Natl Compr Canc Netw. 2019;17(9):1049-1058. doi:10.6004/jnccn.2019.7296
57. Barcelo A, Duffett-Leger L, Pastor-Valero M, Pereira J, Colugnati FA, Trapido E. The role of education on cancer amenable mortality among non-Hispanic blacks & non-Hispanic whites in the United States (1989-2018). BMC Cancer. 2021;21(1):1- 13. doi:10.1186/s12885-021-08633-7
58. Winkleby MA, Jatulis DE, Frank E, Fortmann SP. Socioeconomic status and health: how education, income, and occupation contribute to risk factors for cardiovascular disease. Am J Public Health. 1992;82(6):816-820. doi:10.2105/ajph.82.6.816
59. Singh GK, Jemal A. Socioeconomic and Racial/Ethnic Disparities in Cancer Mortality, Incidence, and Survival in the United States, 1950-2014: Over Six Decades of Changing Patterns and Widening Inequalities. J Environ Public Health. 2017;2017:2819372. doi:10.1155/2017/2819372
60. DeRouen MC, Schupp CW, Koo J, et al. Impact of individual and neighborhood factors on disparities in prostate cancer survival. Cancer Epidemiol. 2018;53:1-11. doi:10.1016/j.canep.2018.01.003




