

Comparison of Hemostasis Times With a Kaolin-Based Hemostatic Pad (QuikClot Radial) vs Mechanical Compression (TR Band) Following Transradial Access: A Pilot Prospective Study
Abstract: Background. Hemostasis following transradial access (TRA) is usually achieved by mechanical compression. We investigated use of the QuikClot Radial hemostasis pad (Z-Medica) compared with the TR Band (Terumo Medical) to shorten hemostasis after TRA. Methods. Thirty patients undergoing TRA coronary angiography and/or percutaneous coronary intervention were randomized into three cohorts post TRA: 10 patients received mechanical compression with the TR Band, 10 patients received 30 min of compression with the QuikClot Radial pad, and 10 patients received 60 min of compression with the QuikClot Radial pad. Times to hemostasis and access-site complications were recorded. Radial artery patency was evaluated 1 hour after hemostasis by the reverse Barbeau’s test. Results. There were no differences in patient characteristics, mean dose of heparin (7117 ± 1054 IU), or mean activated clotting time value (210 ± 50 sec) at the end of procedure among the three groups. Successful hemostasis was achieved in 100% of patients with both the 30-min and 60-min compression groups using the QuikClot pad. Hemostasis failure occurred in 50% of patients when the TR Band was initially weaned at the protocol-driven time (40 min after sheath removal). Mean compression time for hemostasis with the TR Band was 149.4 min compared with 30.7 min and 60.9 min for the 30-min and 60-min QuikClot groups, respectively. No radial artery occlusion occurred in any subject at the end of the study. Conclusions. Use of the QuikClot Radial pad following TRA in this pilot trial significantly shortened hemostasis times when compared with the TR Band, with no increased complications noted.
J INVASIVE CARDIOL 2017;29(10)328-334. Epub 2017 August 15.
Key words: transradial access, hemostasis, kaolin, QuikClot Radial, TR Band
Transradial access (TRA) is being increasingly used for both diagnostic coronary angiography and percutaneous coronary intervention (PCI) due to its lower risk of vascular complications, early ambulation, reduced duration of hospital stay, and decreased mortality after ST-elevation myocardial infarction (STEMI) PCI compared with femoral access.1-4 Access-site hemostasis is a critical component of a successful transradial intervention.5,6 Manual compression of the radial artery after TRA has been replaced by mechanical compression devices because of the length of compression time needed to achieve hemostasis with current antiplatelet and anticoagulant therapies. Multiple mechanical compression hemostatic devices have been developed and introduced into clinical practice, with the aim of improving TRA access-site hemostasis and limiting local complications.7-11
The TR Band radial compression device (Terumo Medical) is currently the most widely used mechanical compression device after TRA in the United States. It has been widely studied, with protocols using shorter compression times and patent hemostasis reducing the most common complication post TRA – radial artery occlusion (RAO), with near 100% success rates of radial artery hemostasis. There is no standard protocol for total time of radial artery compression/weaning using a TR Band, with most published protocols using compression/weaning times of 2 to 3 hours to obtain hemostasis.9-13
Pancholy et al showed that shorter compression times with the TR Band result in less RAO.11 Rashid et al in a recent meta-analysis of 31,345 TRA patients reported that shorter compression times and higher doses of heparin were associated with lower rates of RAO.14 With mechanical compression, the lower limit of compression/wean times for successful hemostasis post PCI appears to be 2 to 2.5 hours.9-11,13 Can compression times for radial artery hemostasis post TRA be shortened with a pro-hemostatic pad, possibly further reducing RAO and shortening the time and resources required post TRA? There is very little in the literature to support this strategy post TRA. Compression times and earlier ambulation have been reduced with pro-hemostatic pads after femoral arterial procedures.15-17 With this in mind, a small pilot trial using a commercially available hemostatic pad (QuikClot Radial; Z-Medica) was developed, with a primary endpoint assessing hemostasis times.
QuikClot Radial is a hemostatic device that is composed of a kaolin-impregnated gauze pad. Kaolin initiates the clotting cascade when exposed to blood by activating factor XII.18 Kaolin-impregnated gauze (QuikClot Combat Gauze) significantly reduced bleeding compared with standard gauze in a femoral artery injury model in swine.19 QuikClot hemostatic pads achieved faster femoral artery hemostasis and allowed for earlier ambulation and shorter hospital stays when compared with manual compression after PCI.15,20 A recent study showed a trend toward reduced RAO with the QuikClot pad compared with conventional radial artery gauze compression.21 This study did not conclusively demonstrate shortened hemostasis times, but used a very short compression time of 15 minutes vs 120 minutes with the QuikClot pad. There are no studies comparing the use of the TR Band vs the QuikClot Radial pad to assess hemostasis times and the risk of complications related to transradial access. Herein, we report our experience with use of the QuikClot Radial pad after transradial diagnostic coronary angiography and/or PCI compared with use of the TR Band in a small cohort of consecutive patients.
Methods
Patient population. All consecutive patients undergoing transradial diagnostic coronary angiography and/or interventional coronary procedures from March 31, 2016 to May 13, 2016, who signed informed consent to participate in the study, were enrolled prospectively. Patients were included in the study if they were at least 18 years old and able to give informed consent. Patient exclusion criteria included STEMI, pregnancy, oral anticoagulation therapy, liver failure, and inability to give informed consent. Thirty patients were included in the study and randomized into three different strategies of radial closure (n = 10 per group). Subjects were randomized by the sequentially numbered opaque sealed envelope method.22 Clinical characteristics were obtained by review of hospital charts and patient interview. Data on antiplatelet and anticoagulant therapy were recorded. All procedures were performed by two interventional cardiologists at a single catheterization laboratory under similar operating conditions. The study protocol was approved by Memorial Healthcare System’s Institutional Review Board and all study participants signed written informed consent.
Procedures. All transradial procedures were performed using ultrasound guidance for vascular access as described previously.23-25 A 5 Fr sheath was used if the baseline radial artery diameter was ≤2.0 mm and a 6 Fr sheath was used if the diameter was >2.0 mm. A 7 Fr sheath was used for complex interventions if the radial artery diameter was ≥2.5 mm. After sheath insertion, all patients received 2.5 mg of intraarterial verapamil via the sheath. All patients received intravenous heparin after sheath insertion, using 70 U/kg, with a minimum of 4000 U and a maximum of 7000 U for diagnostic procedures. Additional heparin was given for PCI if needed, to achieve an activated clotting time (ACT) of 250-300 seconds. An ACT was measured in all patients at the end of the procedure from the arterial introducer sheath using the i-STAT system (Abbott Vascular).
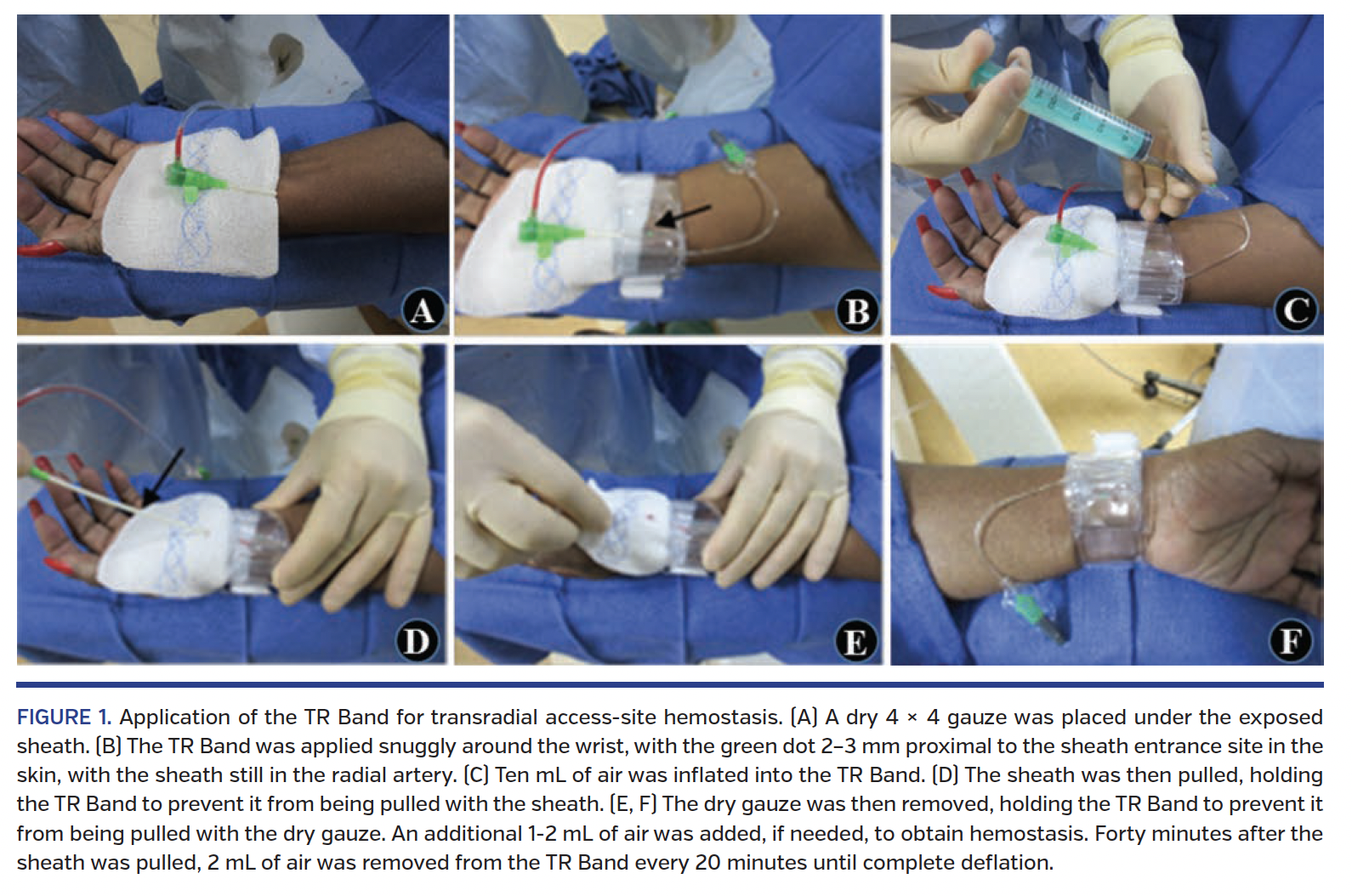
Hemostatic device application. At the end of the procedure, consented subjects were randomized in the cardiac cath lab upon completion of their procedure to one of three hemostasis protocols: (1) 120-minute TR Band compression/weaning; (2) 30-minute QuikClot Radial compression; or (3) 60-minute QuikClot Radial compression. In the TR Band group, the TR Band was applied very snuggly and inflated with 10 mL air with the sheath still in the radial artery; the sheath was then pulled (Figure 1). In 9/10 patients, there was no evidence of bleeding from the puncture site. In 1/10 patients, an additional 3 mL of air was needed for hemostasis. Forty minutes after the sheath was pulled, 2 mL of air was removed from the TR Band every 20 minutes until complete deflation. If any bleeding occurred during deflation, 2 mL of air was re-injected, and weaning was recommenced in 20 minutes. After complete deflation, the TR Band was removed and hemostasis was confirmed. A BandAid adhesive bandage (Johnson & Johnson) was then applied to the puncture site.
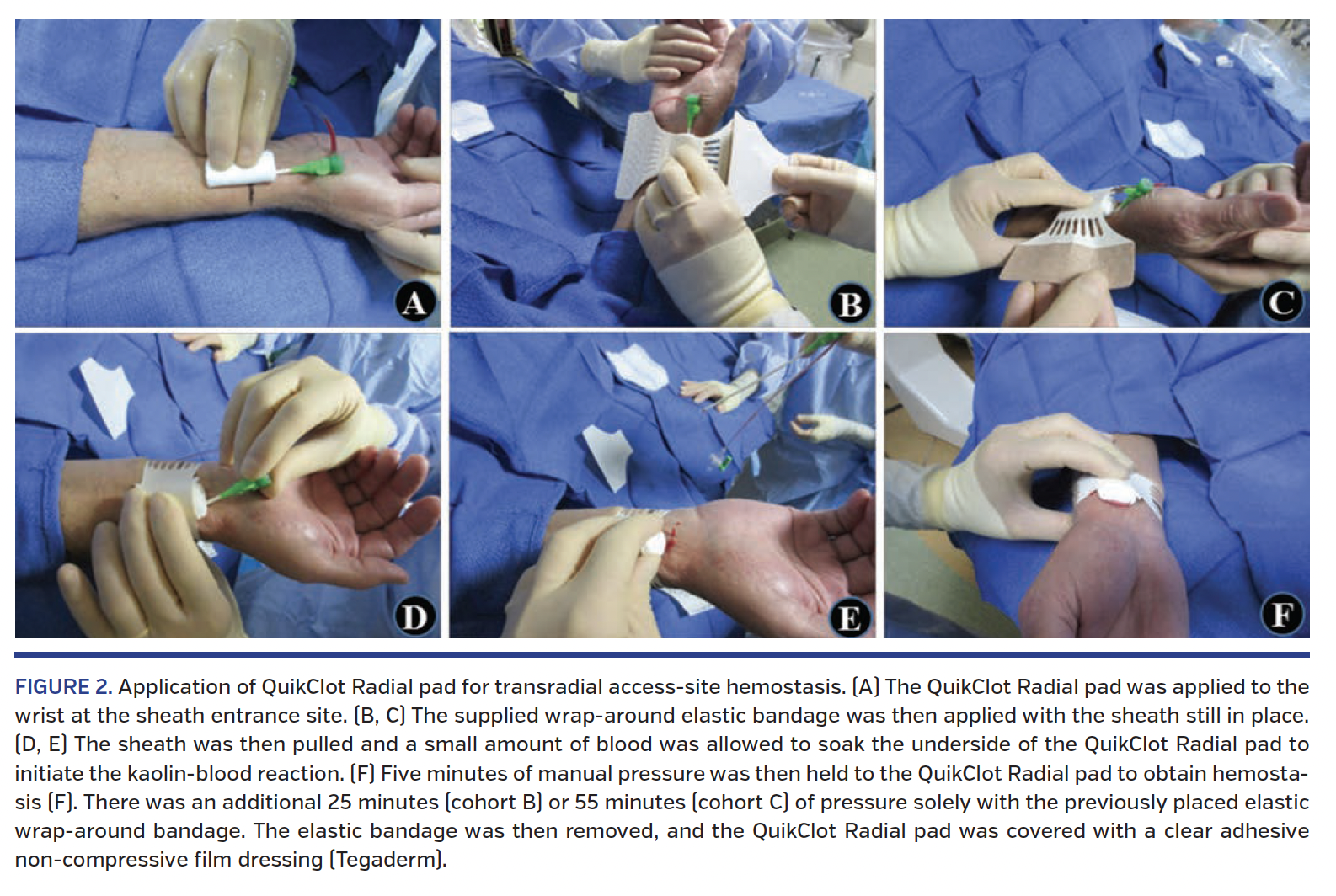
For the 30-minute QuikClot group, the QuikClot Radial pad was secured to the wrist at the sheath entrance site with the supplied wrap around elastic bandage with the sheath still in place (Figures 2A, 2B, 2C). The sheath was then pulled and a small amount of blood was allowed to soak the underside of the QuikClot Radial pad to initiate the kaolin-blood reaction (Figures 2D, 2E). Manual pressure was then held to the QuikClot Radial pad for 5 minutes to obtain hemostasis (Figure 2F). There was an additional 25 minutes of pressure solely with the previously placed elastic wrap around the bandage (Figure 2D). The elastic bandage was then removed, leaving the QuikClot Radial pad undisturbed over the puncture site. The QuikClot Radial pad was then covered with a clear adhesive non-compressive film dressing (Tegaderm; 3M Medical), to be removed the following morning by the patient. For the 60-minute QuikClot group, the procedure was the same as in the 30-minute group, except the wrap around the elastic bandage was left in place for 55 minutes after the 5 minutes of manual compression.
Hemostasis was defined as no bleeding at the puncture site with no evidence of expanding forearm hematoma. Time to hemostasis was defined as the elapsed time between sheath removal and successful hemostasis.
Postoperative access-site outcomes. Access-site hemostasis and complications were assessed after hemostatic device application. The first access-site check was performed in the cardiac cath lab by the interventional cardiologist before patients were transferred to the recovery unit. In the recovery unit, there was near-continuous access-site observation by the research nurse coordinator and/or the recovery nurse. A reverse Barbeau’s test26 was performed by the research nurse coordinator 1 hour after hemostasis was confirmed in all patients to evaluate radial artery patency. A verbal numeric analog pain scale (zero for no pain, through 10 for the worst pain) was also administered 1 hour after hemostasis was obtained. Device failure was defined as the inability to use the device or the persistence of bleeding despite proper application of the device. Major complications were defined as: major bleeding (reduction in hemoglobin of ≥3 g/dL related to TRA-site bleeding or forearm hematoma); hematoma of the forearm with any neurovascular compromise of the hand; blood transfusion within 48 hours of the procedure related to bleeding from the access site; pseudoaneurysm; surgical intervention of the hand, wrist or forearm related to TRA compression complication; and ipsilateral hand ischemia. Minor complications were defined as: re-bleeding only requiring further compression; hematoma >6 cm without neurovascular compromise of the hand; RAO without ischemia of the hand; ecchymosis >6 cm; or skin reaction (ie, rash, severe pruritus) to either device.
All patients were followed 1 day post procedure by the research nurse coordinator, either in person for inpatients or by telephone for outpatients. Patients were questioned about access-site pain or perceived complications.
Statistical analysis. Continuous parametric variables were presented as mean ± standard deviation unless otherwise noted. Categorical variables were presented as counts and percentages. The analysis was performed using GraphPad Prism software 5.0. A two-tailed P-value of <.05 was considered statistically significant.
Results
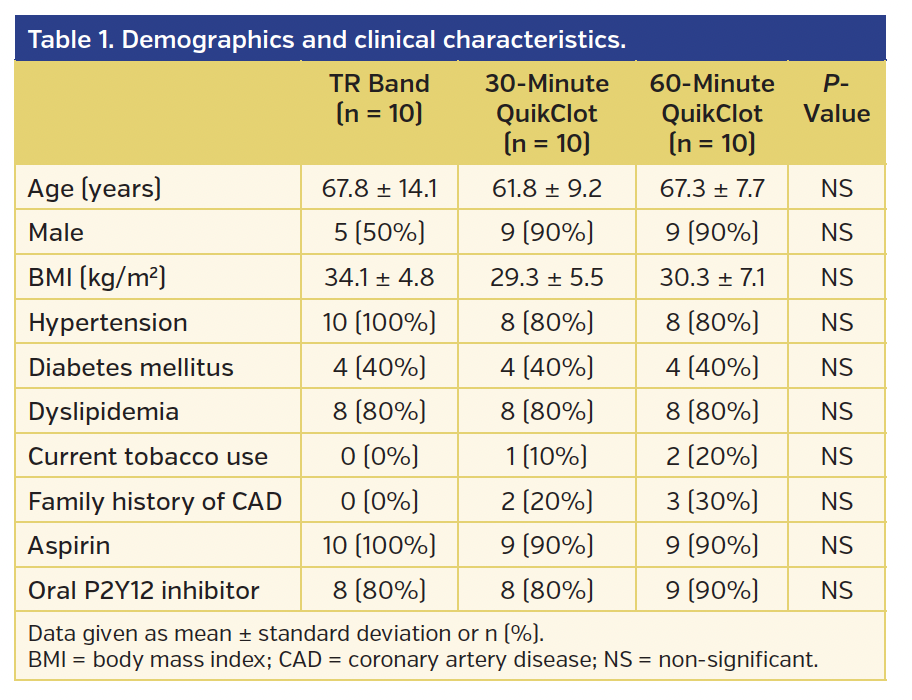
Sixty-seven percent of the 30 patients enrolled in the study were men. The average age of the study population was 65.6 ± 6.1 years. The average body mass index was 31.2 ± 3.8 kg/m2. The 30 patients studied were randomized into three equal groups, and the patients’ demographics and clinical characteristics by group are shown in Table 1. Eighty-seven percent of patients had arterial hypertension, 40% were diabetics, and 80% had dyslipidemia. Prior to the procedure, 93% of all patients were receiving aspirin, and 83% were on oral P2Y12 receptor antagonists. There were no significant differences in demographic and clinical characteristics between the TR Band and QuikClot groups (Table 1).
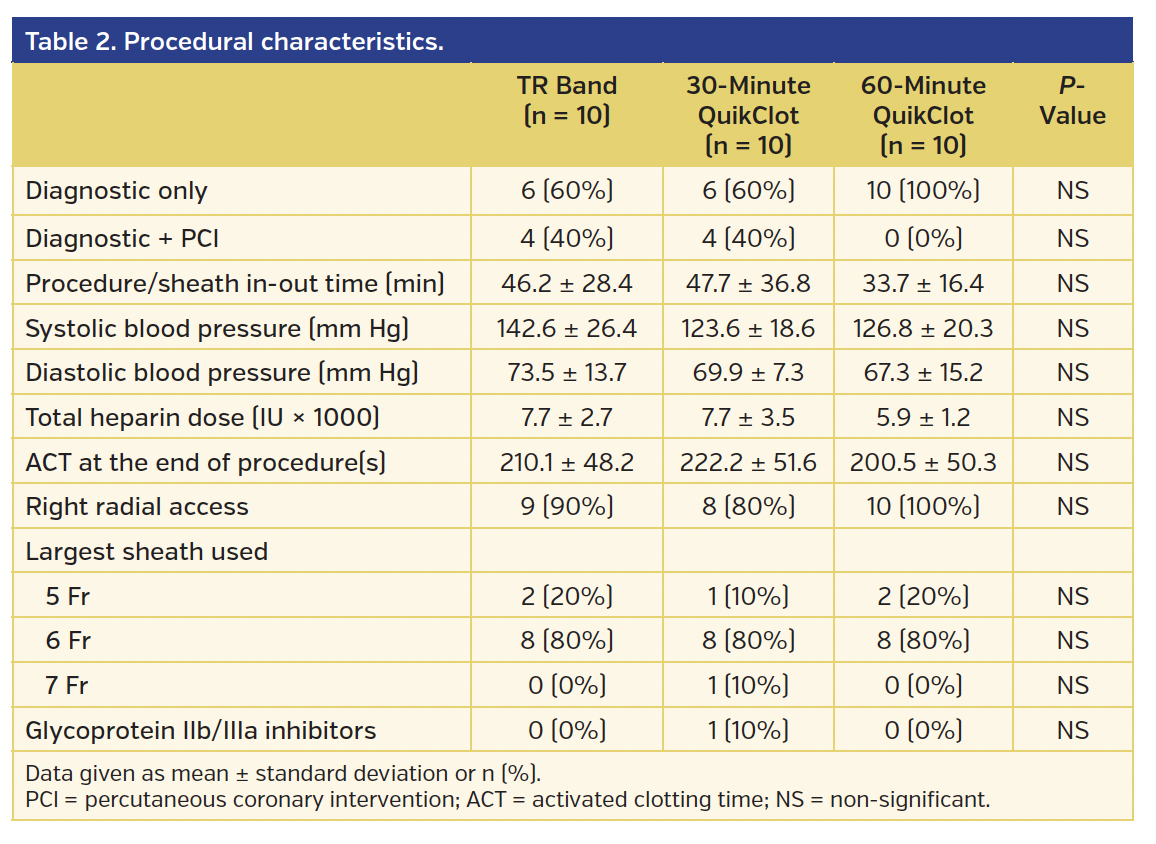
Procedural characteristics are presented in Table 2. Access was obtained via the right radial artery in 90% of cases. A 6 Fr sheath was used in 24 patients, a 5 Fr sheath in 5 patients, and a 7 Fr sheath in 1 patient. Diagnostic coronary angiography was performed in all cases, of which 8 patients had ad hoc PCI. Heparin was the only anticoagulant used for all procedures. One patient (in the 30-minute QuikClot cohort) received an intravenous glycoprotein IIb/IIIa inhibitor (eptifibatide). The average amount of heparin used was 7116 ± 1054 U. No significant differences were found in the amount of heparin used between the TR Band and QuikClot groups (Table 2). At the end of the procedure, there were no differences in the ACT values between the TR Band and QuikClot groups (Table 2). Blood pressure was measured when the sheath was pulled, and no differences were found between the TR Band and QuikClot groups (Table 2). Procedure time was calculated as sheath insertion until sheath removal, and no differences were found among the groups (Table 2).
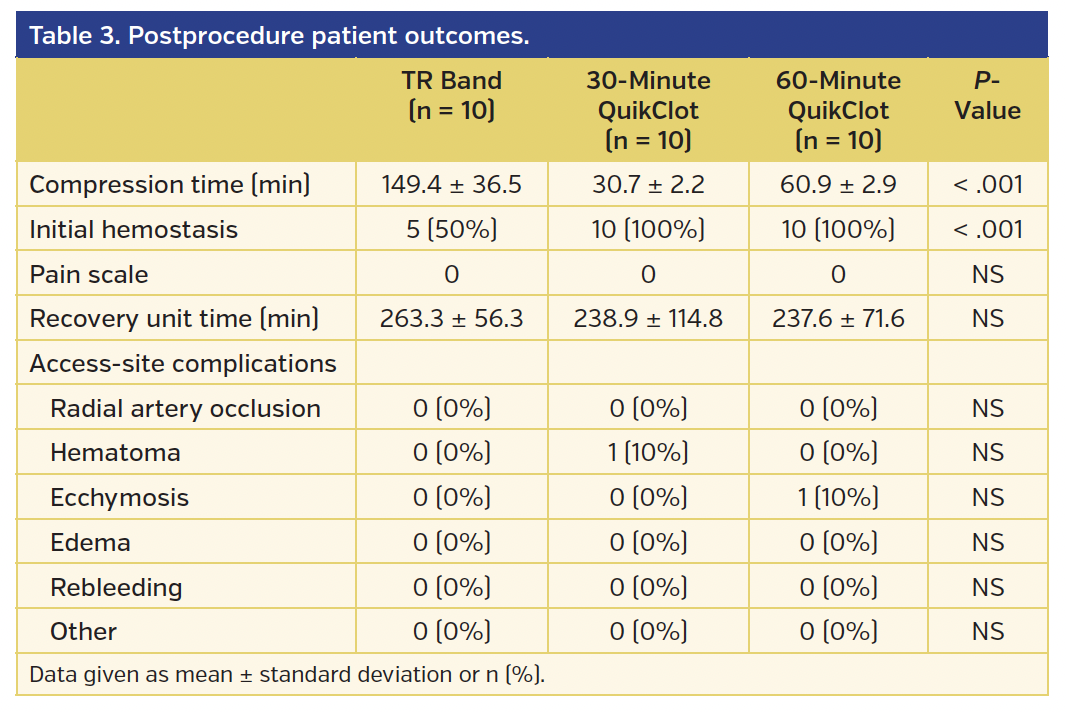
As shown in Table 3, successful initial access-site hemostasis was achieved in all cases with use of QuikClot and failed in 5 cases (50%) with use of TR Band (P<.001). This “failure” was oozing when the TR Band was initially weaned at the protocol-driven 40 minutes after sheath removal, by removing 2 mL of air. All oozing stopped with reinstitution of 2 mL of air. No further oozing was noted during further protocol-driven weaning of the TR Band. The mean compression times were significantly shorter in the QuikClot groups vs the TR Band group (149.4 minutes in the TR Band group vs 30.7 minutes in the 30-minute QuikClot group and 60.9 minutes in the 60-minute QuikClot group; P<.001) (Table 3). In addition, the average recovery unit stays in the QuikClot groups were slightly shorter, but did not reach statistical significance vs the TR Band group (Table 3). One patient in the 30-minute QuikClot group developed a forearm hematoma proximal to the access site while the compressive bandage was still in place. This resolved with 7 minutes of manual compression, and did not interfere with the 30 minutes for hemostasis at the access site. One patient in the 60-minute QuikClot group developed minor ecchymosis after the QuikClot pad was removed. There was no RAO in any subject, assessed at 1 hour post hemostasis by the reverse Barbeau’s test. No rebleeding, edema, pain, and other immediate or delayed complications occurred in any other case.
Discussion
To the best of our knowledge, this is the first randomized prospective study to investigate the efficacy and safety of the QuikClot Radial hemostatic pad in comparison to mechanical compression with the TR Band in a series of consecutive patients undergoing transradial diagnostic coronary angiography and/or PCI. In this small pilot trial, time to hemostasis was significantly shorter with use of the QuikClot Radial pad compared with the TR Band. No RAOs or major complications occurred in any subject at the end of this study. The small number of patients in this underpowered pilot trial limit the conclusions that can be made. Larger studies are needed to determine if the QuikClot Radial pad can safely shorten hemostasis times after transradial procedures.
The potential benefits of shorter compression times post TRA are numerous. For the patient, there may be less discomfort by shortening the amount of time with a compression device on their wrist. There may also be fewer RAOs.11,14 Although RAO is a clinically silent event, it may limit use of the wrist for future procedures. For the health-care system, there may be less resource utilization. Patients undergoing outpatient diagnostic-only catheterizations could go home earlier. PCI patients and all inpatients could potentially be moved out of the cath lab recovery area earlier, to a less resource-intensive area. Many cath labs develop a bottle neck in the afternoon in the recovery area. All recovery beds may be full, thereby blocking completed procedures in the cath lab from quickly going into the recovery area, which leads to a delay in completing additional cath lab cases. This may lead to increased overtime pay to the cath lab staff to get the cases completed, further increasing costs to the system. If an hour or more could be reliably reduced in obtaining TRA hemostasis, there would be less resource utilization needed post TRA, which could result in costs savings to the health-care system.
In the TR Band cohort of our small, underpowered, pilot trial, 5 of 10 patients had oozing at the protocol-specified 40 minutes to initiate weaning of air. We purposely designed a 2-hour TR Band weaning protocol in order to give the shortest compression/weaning time we thought was reasonable. We elected to have a short full compression time of 40 minutes, and a longer weaning time of 80 minutes, to hopefully minimize slower flow through the RA from partial compression, thereby preventing RAO.14 It’s possible that 40 minutes was not enough time to allow a stable clot to form at the RA arteriotomy site. In a future-planned, larger, and adequately powered trial, we will use a full compression time of 60 minutes and then wean over the subsequent 60 minutes to see if we can reliably attain a 120-minute hemostasis time with the TR Band. In our present pilot trial, all oozing was with the initial removal of air at 40 minutes. As there was no further oozing on subsequent weaning of air, we hope that the 60 minutes of full compression, with subsequent weaning over 60 minutes, will be the “sweet spot” to allow for the shortest full compression time, but successful hemostasis at 120 minutes. Possibly, a 90-minute full compression time would be better, with weaning over the next 30 minutes, which may be studied in another future trial. It is interesting that the TR Band has been used for years, but there is no standardized weaning technique.9-13 Each institution seems to have its own protocol. Some institutions use longer full compression, then a rapid weaning of air. Others use shorter full compression times, with longer weaning periods to fully deflate the TR Band.
There are multiple hemostatic pads on the market for femoral hemostasis, and several specifically marketed for TRA.10,27 High-quality data on the use of any of these hemostatic pads after TRA is very limited, though. Our 30-minute and 60-minute QuikClot protocols were developed from the few reports describing its use after TRA and femoral access.15,20,21 In a trial by Politi et al21 failed hemostasis occurred in 20% of QuikClot patients with a 15-minute compression time post TRA. Because of this, we elected to use 30-minute and 60-minute compression times. We are encouraged that there was 100% successful hemostasis in both groups, but this was a small, underpowered study. We were also encouraged that there was successful hemostasis in all QuikClot patients after the initial 5-minute manual hold. No one required repeat manual compression to obtain initial hemostasis in this small, pilot trial.
The 100% successful hemostasis with QuikClot occurred with slightly higher doses of heparin than are typically used. We elected to give 70 U/kg of heparin on all diagnostic studies (up to a maximum of 7000 U), not a standard 5000 U dose. Our average body mass index in this study was 31.2 kg/m2, with an average heparin dose of 7117 U/patient. In the 60-minute QuikClot cohort, by chance, there were no PCIs. The average dose of heparin for these diagnostic-only cases was 5900 U, higher than the standard 5000 U traditionally given. If the conclusion of Rashid et al’s meta-analysis14 that higher-dose heparin with shorter compression times reduces RAO is correct, then use of hemostatic pads after TRA may allow us to achieve this goal. Possibly, though, hemostatic pads may cause more RAO because of their procoagulant effects. This was not observed in this small, pilot trial. Only larger, adequately powered, randomized trials will give us this information.
Conclusion
In this small, pilot trial comparing a kaolin-based hemostatic pad (QuikClot Radial) with mechanical compression (TR Band) after TRA, hemostasis times were significantly shorter with the QuikClot Radial pad, with no increase in complications noted. Potential benefits include less RAO, improved patient comfort, and less resource utilization post TRA. A larger, adequately powered trial, which is presently being planned, is needed to assess the true efficacy and safety of this approach.
References
1. Dobies DR, Barber KR, Cohoon AL. Analysis of safety outcomes for radial versus femoral access for percutaneous coronary intervention from a large clinical registry. Open Heart. 2016;3:e000397.
2. Mitchell MD, Hong JA, Lee BY, Umscheid CA, Bartsch SM, Don CW. Systematic review and cost-benefit analysis of radial artery access for coronary angiography and intervention. Circ Cardiovasc Qual Outcomes. 2012;5:454-462.
3. Romagnoli E, Biondi-Zoccai G, Sciahbasi A, et al. Radial versus femoral randomized investigation in ST-segment elevation acute coronary syndrome: the RIFLE-STEACS (Radial Versus Femoral Randomized Investigation in ST-elevation Acute Coronary Syndrome) study. J Am Coll Cardiol. 2012;60:2481-2489.
4. Mehta SR, Jolly SS, Cairns J, et al. Effects of radial versus femoral artery access in patients with acute coronary syndromes with or without ST-segment elevation. J Am Coll Cardiol. 2012;60:2490-2499.
5. Rao SV, Bernat I, Bertrand OF. Clinical update: remaining challenges and opportunities for improvement in percutaneous transradial coronary procedures. JACC Cardiovasc Interv. 2013;6:99-112.
6. Zwaan EM, Koopman AGMM, Holtzer CAG, et al. Revealing the impact of local access-site complications and upper extremity dysfunction post transradial percutaneous coronary procedures. Neth Heart J. 2015;23:514-524.
7. Chatelain P, Arceo A, Rombaut E, Verin V, Urban P. New device for compression of the radial artery after diagnostic and interventional cardiac procedures. Cathet Cardiovasc Diagn. 1997;40:297-300.
8. Ochiai M, Sakai H, Takeshita S, et al. Efficacy of a new hemostatic device, adapty, after transradial coronary angiography and intervention. J Invasive Cardiol. 2000;12:618-622.
9. Pancholy SB. Impact of two different hemostatic devices on radial artery outcomes after transradial catheterization. J Invasive Cardiol. 2009;21:101-104.
10. Cox T, Blair L, Huntington C, Lincourt A, Sing R, Heniford BT. Systematic review of randomized controlled trials comparing manual compression to vascular closure devices for diagnostic and therapeutic arterial procedures. Surg Technol Int. 2015;27:32-44.
11. Pancholy SB, Patel TM. Effect of duration of hemostatic compression on radial artery occlusion after transradial access. Catheter Cardiovasc Interv. 2012;79:78-81.
12. Rathore S, Stables RH, Pauriah M, et al. A randomized comparison of TR Band and Radistop hemostatic compression devices after transradial coronary intervention. Catheter Cardiovasc Interv. 2010;76:660-667.
13. Dai N, Xu DC, Hou L, et al. A comparison of 2 devices for radial artery hemostasis after transradial coronary intervention. J Cardiovasc Nurs. 2015;30:192-196.
14. Rashid M, Kwok CS, Pancholy S, et al. Radial artery occlusion after transradial interventions: a systematic review and meta-analysis. J Am Heart Assoc. 2016;5:e002686.
15. Trabattoni D, Gatto P, Bartorelli AL. A new kaolin-based hemostatic bandage use after coronary diagnostic and interventional procedures. Int J Cardiol. 2012;156:53-54.
16. Balzer JO, Schwarz W, Thalhammer A, Eichler K, Schmitz-Rixen T, Vogl TJ. Postinterventional percutaneous closure of femoral artery access sites using the Clo-Sur PAD device: initial findings. Eur Radiol. 2007;17:693-700.
17. Nguyen N, Hasan S, Caufield L, Ling FS, Narins CR. Randomized controlled trial of topical hemostasis pad use for achieving vascular hemostasis following percutaneous coronary intervention. Catheter Cardiovasc Interv. 2007;69:801-807.
18. Zhu S, Diamond SL. Contact activation of blood coagulation on a defined kaolin/collagen surface in a microfluidic assay. Thromb Res. 2014;134:1335-1343.
19. Johnson D, Westbrook DM, Phelps D, et al. The effects of QuikClot Combat Gauze on hemorrhage control when used in a porcine model of lethal femoral injury. Am J Disaster Med. 2014;9:309-315.
20. Trabattoni D, Montorsi P, Fabbiocchi F, Lualdi A, Gatto P, Bartorelli AL. A new kaolin-based haemostatic bandage compared with manual compression for bleeding control after percutaneous coronary procedures. Eur Radiol. 2011;21:1687-1691.
21. Politi L, Aprile A, Paganelli C, et al. Randomized clinical trial on short-time compression with Kaolin-filled pad: a new strategy to avoid early bleeding and subacute radial artery occlusion after percutaneous coronary intervention. J Interv Cardiol. 2011;24:65-72.
22. Kim J, Shin W. How to do random allocation (randomization). Clin Orthop Surg. 2014;6:103-109.
23. Baumann F, Roberts JS. Real time intraprocedural ultrasound measurements of the radial and ulnar arteries in 565 consecutive patients undergoing cardiac catheterization and/or percutaneous coronary intervention via the wrist: understanding anatomy and anomalies may improve access success. J Interv Cardiol. 2015;28:574-582.
24. Baumann F, Roberts JS. Evolving techniques to improve radial/ulnar artery access: crossover rate of 0.3% in 1,000 consecutive patients undergoing cardiac catheterization and/or percutaneous coronary intervention via the wrist. J Interv Cardiol. 2015;28:396-404.
25. Roberts J, Manur R. Ultrasound-guided radial artery access by a non-ultrasound trained interventional cardiologist improved first-attempt success rates and shortened time for successful radial artery cannulation. J Invasive Cardiol. 2013;25:676-679.
26. Barbeau GR, Arsenault F, Dugas L, Simard S, Larivière MM. Evaluation of the ulnopalmar arterial arches with pulse oximetry and plethysmography: comparison with the Allen’s test in 1010 patients. Am Heart J. 2004;147:489-493.
27. Rao SV, Stone GW. Arterial access and arteriotomy site closure devices. Nat Rev Cardiol. 2016;13:641-650.
From the Memorial Regional Hospital, Memorial Healthcare System, Hollywood, Florida.
Funding: An unrestricted research grant was supplied by Z-Medica LLC.
Disclosures: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no financial relationships or conflicts of interest regarding the content herein.
Manuscript submitted March 13, 2017, provisional acceptance given March 24, 2017, and final version accepted April 4, 2017.
Address for correspondence: Jonathan S. Roberts, MD, Memorial Regional Hospital, 1150 N. 35th Avenue, Suite 605, Hollywood, FL 33021. Email: jonathanroberts@mhs.net













