

The Impact and Pathophysiologic Consequences of Coronary Artery Calcium Deposition in Percutaneous Coronary Interventions
Abstract: The presence of coronary artery calcium is indicative of advanced coronary artery disease and is a predictor of clinical events including stroke, myocardial infarction, and cardiac arrest. Recognition of the risk factors and the clinical implications associated with coronary artery calcium is vital in identifying both preventative measures as well as treatment options. Non-invasive and invasive strategies can help quantify these calcified lesions and aid in appropriate patient selection for possible use of atheroablative devices. While mild to moderately calcified lesions can be predilated with balloon angioplasty, severely calcified vessels may be resistant to adequate predilatation and preclude stent delivery and optimal expansion, potentially increasing the risk of early and late complications. The use of atherectomy devices is an invaluable treatment option for these complex lesions, given the ability for plaque modification and changing the compliance of heavily calcified vessels, increasing procedural success rates.
J INVASIVE CARDIOL 2016;28(4):160-167. Epub 2015 August 25.
Key words: atherectomy, coronary artery disease, calcium, percutaneous coronary intervention
_____________________________________________________
The presence of coronary artery calcium (CAC) is indicative of advanced coronary artery disease and can hinder successful stent delivery and optimal expansion, leading to increased risks of short-term and long-term complications after percutaneous coronary intervention (PCI), including stent thrombosis and death.1-4 We discuss the implications of CAC on outcomes during and after PCI as well as interventional strategies used for the successful treatment of these complex lesions.
Pathophysiology of Coronary Calcium Deposition
Calcification is a hallmark sign of advanced atherosclerosis, and the degree of calcification correlates highly with plaque burden.5 Atherosclerosis begins to develop at the stage of fatty streaks often at a young age and occurs in multiple complex stages. The driving principle in plaque formation is a chronic inflammatory process, resulting in endothelial injury. Risk factors such as hypertension, hyperlipidemia, smoking, and hemodynamic perturbations cause endothelial dysfunction as a response to this injury.6 First, endothelial injury leads to cell dysfunction. This dysfunction causes both leukocytes and vascular smooth muscle cells to accumulate and grow within the intimal arterial wall. Subsequent macrophage activation occurs as smooth muscle cells move from the media to the intima. The formation of fatty streaks occurs above the endothelium, where both macrophages and smooth muscle cells engulf lipids. Small amounts of crystalline calcium are present in the lipid particles within the lipid cores.7 Large amounts of connective tissue matrix are formed, ultimately leading to the formation of a mature fibrous plaque.6,8 This chronic and repetitive injury leads to progressive atherosclerosis and the formation of complex calcified lesions.
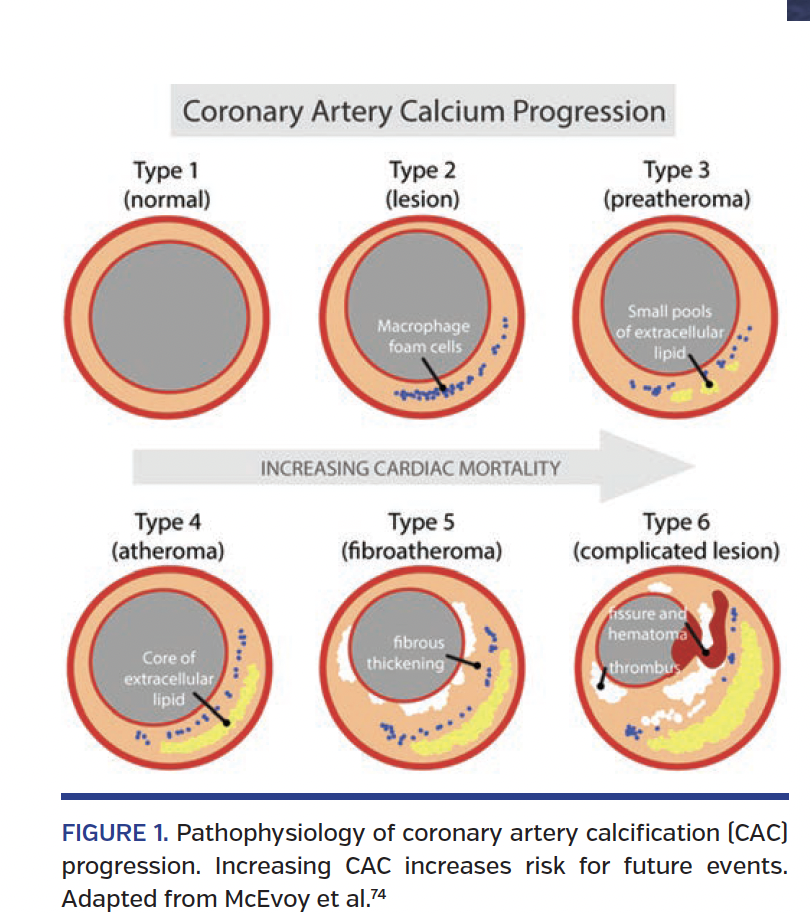
The American Heart Association classifies atherosclerotic lesions into six different types (Figure 1).13 Beginning with isolated foam cells, lesions develop into fatty streaks and subsequently atheroma. Calcification begins to occur in fibroatheroma formations all the way to complicated lesions such as thrombi.9,10 It is at this point that patients enter the clinical phase of atherosclerosis where there is risk of plaque rupture, leading to either thrombotic occlusion or severe stenosis.
Calcification can occur at multiple levels of the arterial wall. The two types of CAC include intimal and medial calcium. The difference between these two types of calcifications may help identify different treatment options. Intimal-layer calcification is characteristic of “classical atherosclerosis” with mineralization occurring in response to inflammation, cell necrosis, lipid deposition with secondary osteogenesis, and vascular calcification.12 In contrast, medial-layer calcification results from elastin fiber mineralization with vascular smooth muscle cellular degeneration and upregulation of osteogenic factors, such as in diabetes mellitus and chronic kidney disease.11 Medial calcification is often associated with arterial stiffness, pulse pressure elevation, and left ventricular hypertrophy, making this type of calcification of clinical relevance. Intimal and medial calcifications often occur together, but can be seen independent of the other.
Impact of Coronary Artery Calcium
In intermediate-risk patients, CAC is a predictor of clinical events including stroke, myocardial infarction, and cardiac arrest.12 The degree of CAC correlates with the risk of cardiovascular events, and is an independent risk factor for cardiovascular disease. In addition, the degree of calcification within an artery correlates with the risk of PCI-related adverse clinical events.13
Quantification of calcium is difficult, but modalities such as angiography and intravascular ultrasound (IVUS) help in its identification. Through these techniques, definitions of calcification severity have been standardized. While moderate calcification is defined as densities seen only during the cardiac cycle prior to contrast injection, severe calcification is defined as densities seen without cardiac motion and usually involves both sides of the arterial wall.14 The difference in severity plays a pivotal role in determining treatment options and risks with PCI. In patients who have mild to moderate disease, predilatation with balloon angioplasty may be sufficient to facilitate stent delivery and optimal expansion.15 However, severe CAC may preclude adequate predilatation with balloon angioplasty and lead to an increased risk of periprocedural complications like dissection and abrupt vessel closure. Repeated predilatation at high pressures in heavily calcified vessels may lead to catastrophic consequences like coronary artery dissection or perforation. Suboptimal stent expansion increases the rate of adverse clinical events, including in-stent restenosis and stent thrombosis.16-19
In a pooled analysis of 6855 patients who underwent PCI in the HORIZONS and ACUITY trials, moderate/severe calcification was associated with older age, more complex disease, and a higher number of stents implanted.19 The unadjusted rates of death, cardiac death, ischemic target-lesion revascularization (TLR) and target-vessel revascularization (TVR), and definite stent thrombosis were significantly increased in the group with moderate/severe calcification at 1 year. By multivariate analysis, the presence of moderate/severe calcification was a strong independent predictor of ischemic TLR and definite stent thrombosis.
The increased risk of myocardial infarction is a known complication during PCI of severely calcified vessels. In a retrospective analysis of PCI in calcified native coronary arteries, 20.9% of patients with 271°-360° of calcium had periprocedural non-Q wave myocardial infarction versus 8.0% of patients with 0°-90° of calcium as measured by IVUS.20 Likewise, stent expansion has an inverse correlation with the arc of the calcium (r = -0.8; P<.001).21
IVUS-defined significant dissection or plaque fracture occurred in 76% of patients directly following balloon dilatation.22 Dissections were significantly larger in calcified lesions when compared with non-calcified lesions (P<.01). Arterial dissections were more common in calcified plaques (73% vs 21%; P=.02) at the site of angioplasty, whereas arterial expansion occurred more often in the plaques that were non-calcified (29% vs 86%; P=.01).23 Dissection occurred more frequently after balloon dilatation compared with rotational atherectomy (77% vs 26%; P=.01).24
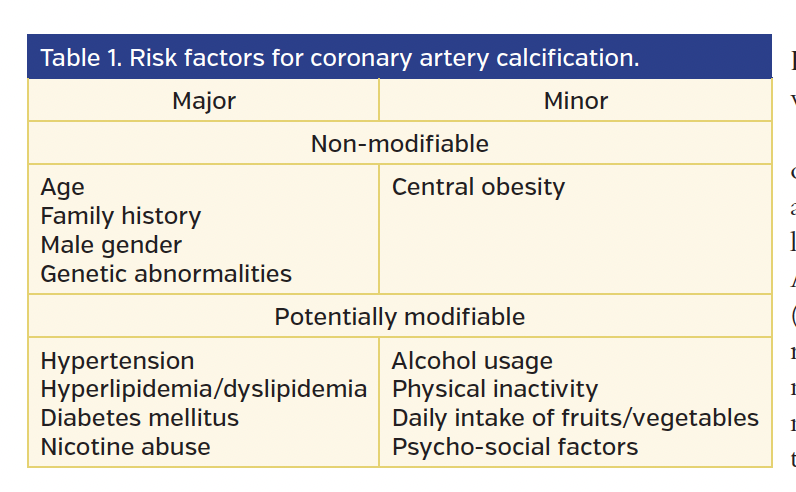
Risk Factors for Coronary Artery Calcium
Understanding the risks associated with CAC and the factors that predispose patients to calcified arteries are vital in identifying both preventative measures as well as treatment options. Risk factors fall under two categories: non-modifiable or potentially modifiable (Table 1).
Diabetes mellitus leads to an advanced rate of CAC and is considered a coronary artery “equivalent” in the evaluation of the Framingham risk score.25,26 Diabetes increases the incidence of myocardial infarction two-fold, making it an important risk factor for cardiovascular disease.6 CAC scoring is one method used to help risk stratify individuals to determine their need for interventions. Interestingly enough, the survival rates of diabetic and non-diabetic patients were not different if they had an absent CAC score (98.8% vs 99.4%; P=.50).27 Thus, individuals without CAC on screening scores had a lower short-term risk of death regardless of the presence of diabetes.27
Chronic kidney disease accelerates CAC similarly to diabetes. The most common cause of end-stage renal disease in the United States is diabetes mellitus.26 Patients with end-stage renal disease were found not only to have larger arterial reference segment and lumen areas and volumes, but they also had larger arterial lumen and plaque areas, with greater calcium arcs on IVUS (P<.05).28 Patients who were transitioning to dialysis also had larger lesion plaque areas and progressive calcific atherosclerosis.28 Coronary artery calcification was a strong predictor of both coronary artery disease and all-cause mortality in both hemodialysis and peritoneal dialysis patients.29
Hypertension is another potentially modifiable risk factor that, without adequate control, can lead to worsening CAC. Of all the metabolic syndrome components, hypertension was the only one associated with retinopathy, nephropathy, and the presence of CAC.30 In patients with type-1 diabetes, hypertension was more associated with CAC than metabolic syndrome itself.30
Multiple risk calculators have been used to help quantify an individual’s probability of developing coronary artery disease. In a multicenter comparison of certain risk markers in the establishment of cardiovascular risk in intermediate-risk patients with the Multi-ethnic Study of Atherosclerosis (MESA) population, CAC scores, ankle-brachial index, C-reactive protein, and family history were all independent risk predictors of cardiovascular and cerebrovascular disease.12 In addition, CAC scores had superior discriminatory capacity and risk reclassification when compared with other markers such as the Framingham risk score. On further analysis of the MESA cohort, the addition of the CAC score to the prediction model based on traditional risk factors allowed an additional 8% of patients in the intermediate-risk group to be separated into either low-risk or high-risk categories.31
Multiple risk factors such as elevated body mass index and low high-density lipoprotein (HDL) in childhood also predicted a relatively higher amount of CAC in adulthood.32 A graded relationship was noted between the total CAC score and the number of risk factors.33 Individuals with metabolic syndrome have a higher prevalence and degree of CAC and a subsequent increased likelihood of myocardial infarction.34
Assessment and Diagnosis of Coronary Artery Calcification
There are several imaging modalities to help assess the presence of CAC, quantify the degree of calcium, and further assess treatment options. The first acute coronary artery disease-related events typically occur in individuals with evidence of mild to moderate CAC.35 Extensive CAC does not typically manifest as acute coronary syndrome (ACS), but often presents as chronic coronary artery disease-related events.35
Non-invasive modalities. Coronary artery calcium scoring is a tool that has been shown to be beneficial in risk stratification for low-risk, intermediate-risk, and high-risk patients. The CAC score on electron-beam computed tomography (CT) predicted angiographically significant coronary artery disease with a sensitivity of 95% and specificity of 66%.36 The specificity increased with higher CAC scores. The absence of a CAC score predicted a <1% likelihood of having angiographically significant coronary artery disease in 1764 symptomatic individuals with suspected coronary artery disease.38 The sensitivity and specificity using ultrafast CT were 94% and 72%, respectively. 39 Thus, it is clear that the clinical utility of CAC scoring for risk stratification of coronary artery disease/ACS is greatest in symptomatic low-risk to intermediate-risk patients. The use of CAC scoring in high-risk patients lacks sensitivity, and thus provides limited information on whether PCI or other interventions are necessary. Modalities such as IVUS are thus necessary to quantify calcium.40
CAC scores detected through the use of CT imaging are graded into four separate categories.41 A calcium score of 0-10 is considered very low risk, 11-100 is moderate risk, 101-400 is moderately high risk, and >400 is considered high risk. These scores are standardized to the age and sex of the individual. A graded relationship was noted between the CAC score and future cardiovascular events, with an exponentially increased risk of myocardial infarction and coronary artery disease resulting in death between relative scores.33,42 In a study that examined all-cause mortality in 25,253 asymptomatic patients with an average follow-up of 6.8 years, CAC scoring showed that the prognostic value was incremental to the Framingham risk model.37
The relative risk (RR) of obstructive coronary artery disease seen on angiography was higher (RR, 4.53) for patients with a CAC score measured by electron-beam CT compared to stress testing alone (RR, 1.72-1.96).43 Coronary artery calcium score had higher sensitivity and specificity over electrocardiogram and thallium stress testing for the presence of obstructive coronary artery disease.44 Thus, in people with intermediate risk, CAC scoring may be beneficial and even superior in coronary artery disease detection compared with stress testing.
In the CONFIRM trial, a total of 24,775 symptomatic patients without known coronary artery disease who were referred for coronary CT angiography and stenoses were graded as no, mild, moderate, or severe.45 Patients with no coronary artery disease seen on CT angiography had a survival rate of 99.7% during a follow-up of 2.3 years, whereas mortality risk increased for non-obstructive, 1-vessel, 2-vessel, and 3-vessel obstructive (>50% stenosis) disease. CT angiography demonstrated independent predictive significance of major adverse cardiac event (MACE) as well as incremental prognostic value of coronary artery disease burden beyond traditional risk factors when compared with other non-invasive modalities.45
Invasive modalities. Invasive modalities such as IVUS or optical coherence tomography (OCT) are better able to quantify calcium deposition when compared with angiography alone. While angiography provides high diagnostic yield, it often underestimates the amount of CAC. The diffuse nature of atherosclerosis in combination with the complex luminal shapes limit angiography in calcium assessment.46 Furthermore, CAC may not be visible on fluoroscopy and thus hinders identification of both calcium distribution and quantity. Hazy angiographic sites may represent irregular plaque, distorted lumen, thrombus, or dissection.47-49 This makes quantification of calcium difficult and thus impedes the determination of an appropriate intervention.
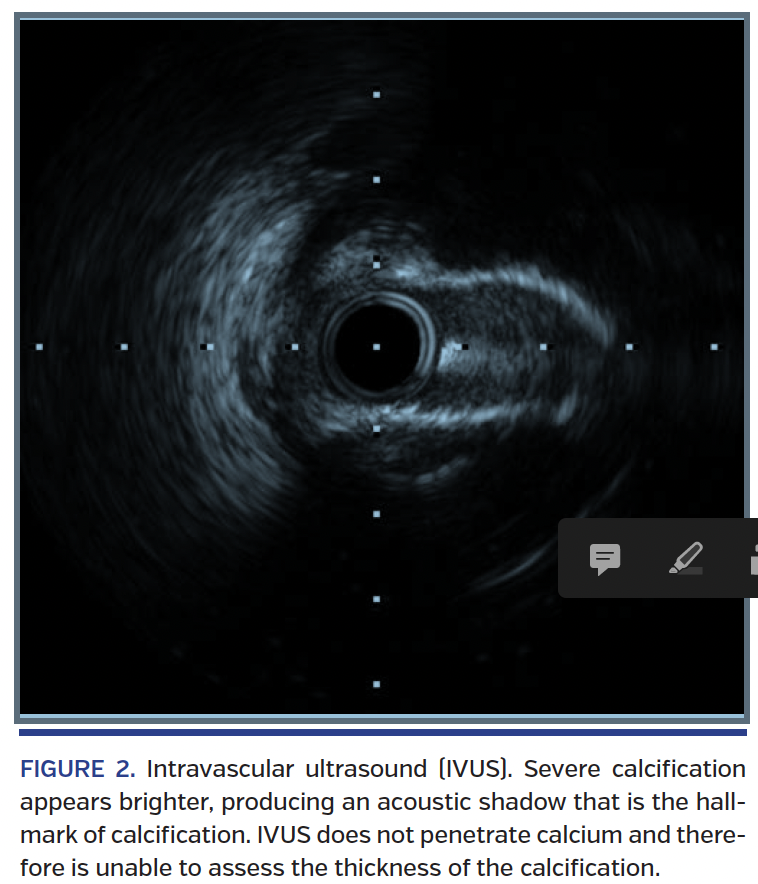
\When CAC is seen on fluoroscopy, it is severe and often superficial. IVUS allows visualization of the coronary wall and is able to successfully delineate plaque extent, composition, morphology and distribution.50,51 Dense material (calcium) will appear brighter on IVUS, producing an acoustic shadow that is the hallmark of calcification (Figure 2). “Soft” plaques can also be identified on ultrasound, as they often appear less echodense because of the collagen-rich adventitia. Techniques using IVUS are better at quantifying calcification through usage of arc and length measurements, but not thickness or mass, because IVUS does not penetrate calcium. Therefore, it is assumed that superficial calcium is thicker than deep calcium. IVUS is thus better at detecting superficial calcium. IVUS was superior to angiography in detecting coronary artery calcium (73% vs 38%; P<.001).14 The clinical utility of IVUS lies in its ability to directly visualize and delineate coronary artery calcium from soft plaque on the arterial wall, which is necessary for patients who undergo PCI. This is effective in the moderate-risk to high-risk patients, as this may influence and guide the appropriate interventional approaches and possible need for atheroablative devices.
OCT uses fiber-optic technology, thereby increasing the resolution compared with IVUS. OCT resolution (10-20 µm) is roughly 10 times higher then the resolution of IVUS (100-150 µm).52 OCT is able to characterize the extent and structure of coronary disease in a much higher plane of view than IVUS. Due to artifacts, IVUS tends to overestimate the CAC that is present. OCT has increased accuracy, because it is able to visualize calcification without significant artifacts.53,54 However, the maximum wall depth penetration is lower with OCT (1-2 mm) compared with IVUS (4-8 mm). OCT also has a strong attenuation of light by blood, thus blood must be removed during OCT examination to prevent scattering of light by red blood cells. This leads to a more technically difficult procedure, requiring balloon occlusion of flow and vessel irrigation by saline.52 In a multicenter study that compared OCT with IVUS, OCT was found to have no serious complications. In addition, poor lumen visibility occurred more often in IVUS than OCT (17.3% vs 6.1%; P=.04).55 It is clear that while this novel technology provides high-quality imaging, its place in the invasive detection of CAC has not been firmly established in the community.
Treatment Options In Calcified Coronary Arteries
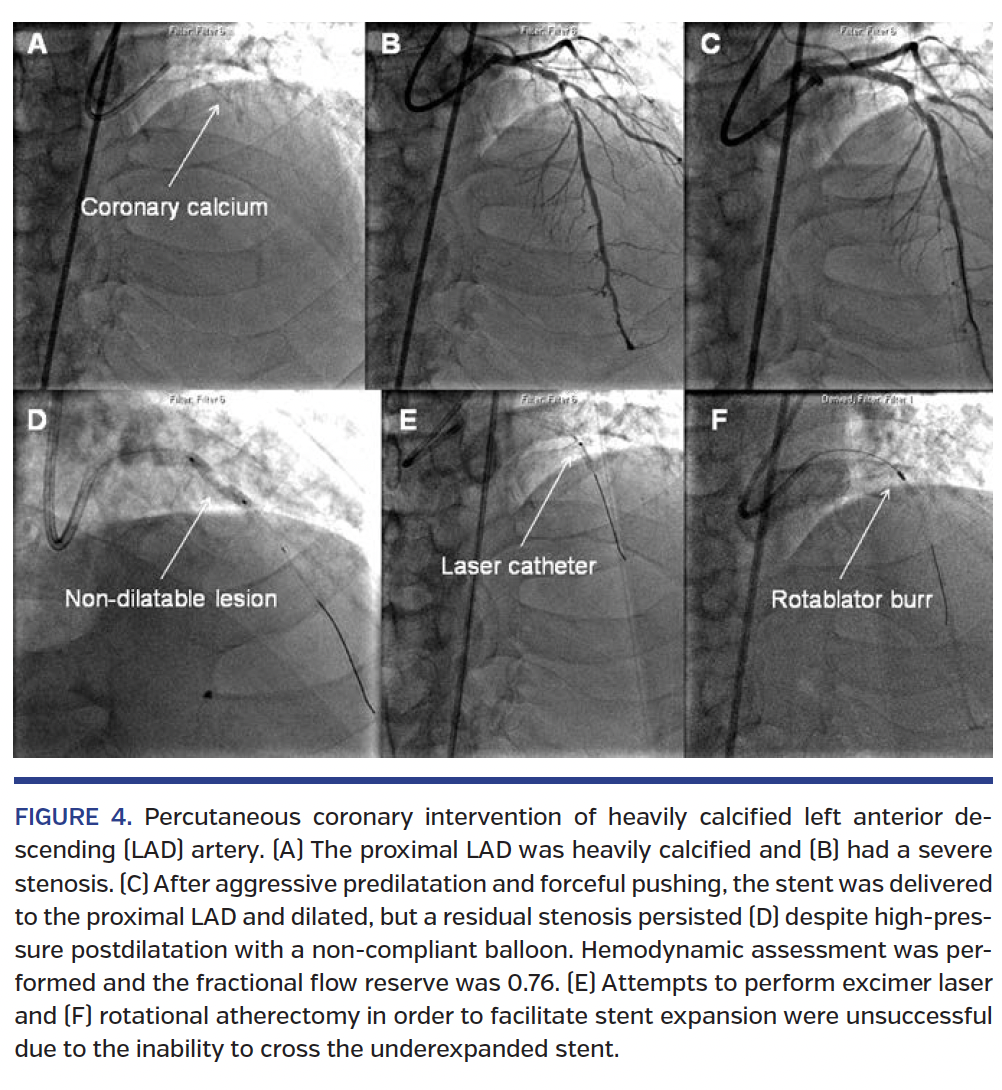
Identification of lesion quantity and quality is important for interventional cardiologists, as they are able to determine patients who may be good candidates for PCI (Figure 3). As previously mentioned, multiple complications may arise in heavily calcified lesions, making PCI technically difficult. Treatment options vary based on the difficulty of PCI and range between the use of balloon angioplasty prior to stent implantation, to scoring/cutting balloons and atherectomy. Inadequate lesion preparation may lead to dissection after balloon angioplasty or the inability to fully expand the stent after inflation (Figure 4). In this section, we outline the different forms of treatment, and emphasize the benefits provided by atherectomy.
Angioplasty, cutting balloon, and laser atherectomy. Balloon angioplasty has often been used to dilate calcified coronary vessels prior to stent implantation. In a meta-analysis of randomized trials that compared balloon angioplasty with laser atherectomy, cutting balloons, and coronary atherectomy, ablative devices increased the risk of restenosis (odds ratio [OR], 1.25), myocardial infarction at 30 days (OR, 2.18), and MACE at 1 year (OR, 1.52).15 While angioplasty may prove feasible in minimally to moderately calcified lesions, there is a higher risk of dissection, increased procedural difficulty, increased stent malposition, and high restenosis rates with greater coronary calcification.1
The cutting balloon contains 3-4 longitudinal atherotome blades mounted on the surface of the balloon to “score” the lesion by producing longitudinal incisions.56 These balloons are ineffective at improving the compliance in heavily calcified vessels and have a higher rate of dissection in moderately to heavily calcified lesions.56 Laser has been associated with high rates of both dissection and perforation and is also ineffective in lesions with severe CAC.57
Rotational atherectomy. Since its introduction in 1988, rotational atherectomy (RA) has been an invaluable tool to modify heavily calcified plaque, but is uncommonly used for these complex lesions.58-61 The device contains a rapidly rotating burr that is coated with microscopic diamond chips, which debulks the calcified plaque by grinding the calcified atheroma into small particles so they may pass through distal capillary beds and smooth the inner-vessel lumen. This facilitates stent delivery and subsequent expansion (Figure 5).58
Initially, RA fell out of favor because it failed to show consistent clinical benefit and resulted in high restenosis rates. It was beneficial in lesions where angioplasty and stenting failed to provide optimal expansion of the vessel. RA improved expansion of bare-metal stents, but had high levels of TLR. The use of drug-eluting stent implantation after RA has shown a significant improvement in TLR rates and overall improved outcomes.62-64
The ERBAC trial showed that while the initial procedural success rate was the greatest with RA as compared with excimer laser and balloon angioplasty (89% vs 77% vs 80%, respectively; P=.01), TLR was significantly higher in the RA group at 1 year.1 The COBRA trial demonstrated that while RA provided higher procedural success rates compared with balloon angioplasty in complex coronary artery disease (85% vs 78%; P<.05), there was no difference seen at 6-month follow-up when comparing restenosis, TLR, or symptomatic outcomes.2
The ROTAXUS trial demonstrated that RA did not reduce late lumen loss after PCI with drug-eluting stents at 9 months.65 In-stent restenosis, TLR, and MACE rates were similar between the RA group and balloon angioplasty group. Possible explanations for this include device-related thermal injury and subsequent platelet activation. However, the angioplasty group had a stent loss rate of 2.5% and crossover rate of 12.3%, compared with a crossover rate of 4.2% in the RA group, resulting in a higher success rate in the RA group (92.5% vs 83.3%; P=.03).65 Drug-eluting stent implantation after RA had relatively low TLR rates (3.4%), which was thought to be one of the limiting factors in the bare-metal stent era.58
Complications associated with RA range from device-related issues to periprocedural problems such as myocardial infarction, dissection, vasospasm, and slow flow/no reflow from distal embolization. Periprocedural myocardial infarction (CK-MB elevation >3x upper limit of normal) after RA occurs in 4%-6% of cases.66,67 Dissection of the coronary vessel is associated with a lower success rate, greater amount of residual stenosis, and greater need for coronary artery bypass grafting, along with decreased coronary blood flow (less than TIMI-3 flow).65,68 In a composite of 3985 lesions, dissection was seen in 10.9% of patients after RA.69 Transient myocardial hypoperfusion from either no or slow blood flow can lead to ischemic complications such as myocardial infarction and distal embolization.70 Device-related complications include burr entrapment in the calcified segment.71 Procedural techniques to decrease the risk of these complications include the use of smaller atherectomy burr sizes, lower speed (rotations per minute), and slower and shorter runs (<15 seconds). Vasodilators may decrease the risk of vasospasm or no/slow reflow.70 In addition to these mechanical-related problems, the procedural time, fluoroscopy time, and need for a staff that is competent with RA usage are all important factors. As these procedures are more difficult and require a more involved staff, there is often some degree of “roto-regret.”
Orbital atherectomy. Orbital atherectomy (OA) is a novel technology for the treatment of heavily calcified coronary arteries (Figure 6).18 Through the use of bidirectional differential cutting, OA is able to treat lesions forward and backward. The crown of the orbit allows continuous blood flow in the artery, limiting no-reflow and the risk of the myocardial hypoperfusion that often causes periprocedural myocardial infarction. OA is also able to cool the artery and allow particles to flow downstream, decreasing the risk of embolization. While RA only cuts a groove in the calcium, OA permits cutting around the entire calcium arc, thus providing a greater area of calcium breakdown.72,73
Two major trials have evaluated the use of OA in de novo calcified coronary lesions. The ORBIT I trial, a Food and Drug Administration investigational device exemption approved non-randomized prospective study, compared 50 patients with de novo moderate to severe calcification.72,73 The cumulative MACE rate was 4% in hospital, 6% at 30 days, and 8% at 6 months, suggesting that OA is effective in changing the compliance of coronary lesions and aiding optimal stent implantation in complex lesions. The ORBIT II trial, which included 443 patients at 49 different United States centers who had severely calcified de novo coronary artery lesions, reported the primary safety endpoint of 30-day MACE rate to be 10.1%, which was primarily driven by non-Q wave myocardial infarction. The primary efficacy endpoint of procedural success was 89.1%, with a successful stent delivery rate of 97.7%.18 This seminal study was the first atherectomy investigational device exemption trial in history that supported the treatment of severely calcified coronary lesions.
Conclusion
The presence of CAC is associated with more complications during PCI, including dissection, distal embolization, coronary hypoperfusion, and procedural failure. Determination of the degree of CAC is imperative to appropriately identify patients who will benefit from atheroablative devices. Although the data do not support the routine use of atherectomy in calcified vessels, there are clearly scenarios where PCI is not feasible in heavily calcified lesions due to the inability to deliver or fully expand the stent without modifying the plaque and improving the compliance of the calcification with atherectomy. Appropriate identification of CAC and utilization of atheroablative devices may improve short-term and long-term outcomes after PCI.
References
1. Reifart N, Vandormael M, Krajcar M, et al. Randomized comparison of angioplasty of complex coronary lesions at a single center. Excimer Laser, Rotational Atherectomy, and Balloon Angioplasty Comparison (ERBAC) study. Circulation. 1997;96:91-98.
2. Dill T, Dietz U, Hamm CW, et al. A randomized comparison of balloon angioplasty versus rotational atherectomy in complex coronary lesions (COBRA study). Eur Heart J. 2000;21:1759-1766.
3. Hoffmann R, Mintz GS, Popma JJ, et al. Treatment of calcified coronary lesions with Palmaz-Schatz stents. An intravascular ultrasound study. Eur Heart J. 1998;19:1224-1231.
4. Moussa I, Ellis SG, Jones M, et al. Impact of coronary culprit lesion calcium in patients undergoing paclitaxel-eluting stent implantation (a TAXUS-IV substudy). Am J Cardiol. 2005;96:1242-1247.
5. Goel R, Garg P, Achenbach S, et al. Coronary artery calcification and coronary atherosclerotic disease. Cardiol Clin. 2012;30:19-47.
6. Schoen FJ. Blood vessels. In: Robbins and Cotran Pathologic Basis of Disease. 7th ed. Kumar V, Abbas AK, Fausto N, eds. Philadelphia: Elsevier Saunders. 2005;315-326.
7. Wexler L, Brundage B, Crouse J, et al. Coronary artery calcification: pathophysiology, epidemiology, imaging methods and clinical implications. Circulation. 1996;94:1175-1192.
8. Mitchell M, Sidawy A. The pathophysiology of atherosclerosis. Semin Vasc Surg. 1998;11:134-141.
9. Stary HC, Chandler AB, Dinsmore RE, et al. A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis: a report from the Committee on Vascular Lesions of the Council on Arteriosclerosis, American Heart Association. Circulation. 1995;92:1355-1374.
10. McEvoy J, Blaha M, Defilippis A, et al. Coronary artery calcium progression: an important clinical measurement? J Am Coll Cardiol. 2010;56:1613-1622.
11. Amann K. Media calcification and intima calcification are distinct entities in chronic kidney disease. Clin J Am Soc Nephrol. 2008;3:1599-1605.
12. Yeboah J, McCelland R, Polonsky T, et al. Comparison of novel risk markers for improvement in cardiovascular risk assessment in intermediate risk individuals. JAMA. 2012;308:788-795.
13. American Heart Association. Heart and Stroke Statistics. Available at https://www.heart.org. Accessed Jan-Feb 2014.
14. Mintz G, Popma J, Pichard A, et al. Patterns of calcification in coronary artery disease. A statistical analysis of intravascular ultrasound and coronary angiography in 1155 lesions. Circulation. 1995;91:1959-1965.
15. Bittl J, Chew D, Topol E, et al. Meta-analysis of randomized trials of percutaneous transluminal coronary angioplasty versus atherectomy, cutting balloon atherectomy or laser angioplasty. J Am Coll Cardiol. 2004;43:936-942.
16. Cavusoglu E, Kini A, Marmur J, et al. Current status of rotational atherectomy. Catheter Cardiovasc Interv. 2004;62:485-498.
17. Kedia G, Lee MS. Stent thrombosis with drug-eluting stents: a re-examination of the evidence. Catheter Cardiovasc Interv. 2007;69:782-789.
18. Chambers J. Evaluation of the utility and efficacy of orbital atherectomy to treat severely calcified lesions: ORBIT II. Presented at ACC 2013 Scientific Sessions. San Francisco, California.
19. Genereux P. Impact of coronary calcification on one-year outcomes after PCI in STEMI and NSTEMI: pooled analysis from HORIZONS and ACUITY trials. Presented at ACC-i2 2013 Scientific Sessions. San Francisco, California.
20. Mosseri M, Satler L, Pichard A, et al. Impact of vessel calcification on outcomes after coronary stenting. Card Revasc Med. 2005;6:147-153.
21. Vavuranakis M, Toutouzas K, Stefanadis C, et al. Stent deployment in calcified lesions: can we overcome calcific restrain with high-pressure balloon inflations? Catheter Cardiovasc Interv. 2001;52:164-172.
22. Fitzgerald P, Ports T, Yock P, et al. Contribution of localized calcium deposits to dissection after angioplasty. An observational study using intravascular ultrasound. Circulation. 1992;86:64-70.
23. Potkin B, Keren G, Mintz G, et al. Arterial responses to balloon coronary angioplasty: an intravascular ultrasound study. J Am Coll Cardiol. 1992;20:942-951.
24. Kovach J, Mintz G, Pichard A, et al. Sequential intravascular ultrasound characterization of the mechanisms of rotational atherectomy and adjunct balloon angioplasty. J Am Coll Cardiol. 1993;22:1024-1032.
25. Karim R, Hodis HN, Detrano R, et al. Relation of Framingham risk score to subclinical atherosclerosis evaluated across three arterial sites. Am J Cardiol. 2008;102:825-830.
26. American Diabetes Association. Facts About Type 2. Available at https://www.diabetes.org. Accessed on August 1, 2013.
27. Raggi P, Shaw LJ, Berman DS, et al. Prognostic value of coronary artery calcium screening in subjects with and without diabetes. J Am Coll Cardiol. 2004;43:1663-1669.
28. Gruberg L, Rai P, Mintz G, et al. Impact of renal function on coronary plaque morphology and morphometry in patients with chronic renal insufficiency as determined by intravascular ultrasound volumetric analysis. Am J Cardiol. 2005;96:892-896.
29. Blacher J, Guerin A. Arterial calcifications, arterial stiffness, and cardiovascular risk in end-stage renal disease. Hypertension. 2001;38:938-942.
30. Rodrigues TC, Canani LH, Schvartzman P, et al. Hypertension is the metabolic syndrome component most strongly associated with microvascular complications and coronary artery calcification in type 1 diabetes. J Endocrinol Invest. 2011;34:58-63.
31. Polonsky TS, McClelland RL, Jorgensen NW, et al. Coronary artery calcium score and risk classification for coronary heart disease prediction. JAMA. 2010;303:1610-1616.
32. Mahoney LT, Burns TL, Stanford W, et al. Coronary risk factors measured in childhood and young adult life are associated with coronary artery calcification in young adults: the Muscatine study. J Am Coll Cardiol. 1996;27:277-284.
33. Wong ND, Kouwabunpat D, Vo AN, et al. Coronary calcium and atherosclerosis by ultrafast computed tomography in asymptomatic men and women: relation to age and risk factors. Am Heart J. 1994;127:422-430.
34. Wong ND, Rozanski A, Gransar H, et al. Metabolic syndrome and diabetes are associated with an increased likelihood of inducible myocardial ischemia among patients with subclinical atherosclerosis. Diabetes Care. 2005;28:1445-1450.
35. Shemesh J, Tenebaum A, Fisman E, et al. Coronary calcium in patients with and without diabetes: first manifestation of acute or chronic coronary events is characterized by different calcification patterns. Cardiovasc Diabetol. 2013;12:2-6.
36. Budoff M, Diamond G, Raggi P, et al. Continuous probabilistic prediction of angiographically significant coronary artery disease using electron beam tomography. Circulation. 2002;105:1791-1796.
37. Budoff MJ, Shaw LJ, Liu ST, et al. Long-term prognosis associated with coronary calcification: observations from a registry of 25,253 patients. J Am Coll Cardiol. 2007;49:1860-1870.
38. Haberl R, Becker A, Leber A, et al. Correlation of coronary calcification and angiographically documented stenoses in patients with suspected coronary artery disease: results of 1,764 patients. J Am Coll Cardiol. 2001;37:451-457.
39. Breen JF, Sheedy PF 2nd, Schwartz RS, et al. Coronary artery calcification detected with ultrafast CT as an indication of coronary artery disease. Radiology. 1992;185:435-439.
40. Joshi P, Blaha M, Blumenthal R, et al. What is the role of calcium scoring in the age of coronary computed tomographic angiography? J Nucl Cardiol. 2012;19:1226-1235.
41. Mettler FA. Computed tomography coronary artery screening and calcium scoring. Chapter 5 – Cardiovascular System. Essentials of Radiology. 3rd ed. Philadelphia; WB Saunders: 2013.
42. Pletcher MJ, Tice JA, Pignone M, et al. Using the coronary artery calcium score to predict coronary heart disease events: a systematic review and meta-analysis. Arch Intern Med. 2004;164:1285-1292.
43. Shavelle DM, Budoff MJ, LaMont DH, et al. Exercise testing and electron beam computed tomography in the evaluation of coronary artery disease. J Am Coll Cardiol. 2000;36:32-38.
44. Kajinami K, Seki H, Takekoshi N, et al. Noninvasive prediction of coronary atherosclerosis by quantification of coronary artery calcification using electron beam computed tomography: comparison with electrocardiographic and thallium exercise stress test results. J Am Coll Cardiol. 1995;26:1209-1221.
45. Min JK, Dunning A, Lin FY, et al. Age- and sex-related differences in all-cause mortality risk based on coronary computed tomography angiography findings. Results from the international multicenter CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter Registry) of 23,854 patients without known coronary artery disease. J Am Coll Cardiol. 2011;58:849-860.
46. Tuzcu EM, Berkalp B, De Franco A, et al. The dilemma of diagnosing coronary calcification: angiography versus intravascular ultrasound. J Am Coll Cardiol. 1996;27:832-838.
47. Higgins CL, Marvel SA, Morrisett JD. Quantification of calcification in atherosclerotic lesions. Arterioscler Thromb Biol. 2005;25:1567-1576.
48. Bezerra HG, Costa MA, Guagliumi G, et al. Intracoronary optical coherence tomography: a comprehensive review clinical and research applications. JACC Cardiovasc Interv. 2009;2:1035-1046.
49. Witzenbichler B, Maehara A, Weisz G, et al. Relationship between intravascular ultrasound guidance and clinical outcomes after drug-eluting stents: the ADAPT-DES study. Presented at the 2013 American Heart Association Scientific Sessions in Dallas, Texas.
50. Yock P, Fitzgerald P, Popp R. Intravascular ultrasound. Sci Am Science Med. 1995;2:68.
51. Fitzgerald PJ, St. Goar FG, Connolly AJ, et al. Intravascular ultrasound imaging of coronary arteries. Is three layers the norm? Circulation. 1992;86:154-158.
52. Terashima M, Kaneda H, Suzuki T. The role of optical coherence tomography in coronary intervention. Korean J Intern Med. 2012;27:1-12.
53. Mintz GS, Nissen SE, Anderson WD, et al. American College of Cardiology clinical expert consensus document on standards for acquisition, measurement and reporting of intravascular ultrasound studies (IVUS). A report of the American College of Cardiology task force on clinical expert consensus documents. J Am Coll Cardiol. 2001;37:1478-1492.
54. Prati F, Regar E, Mintz GS, et al. Expert review document on methodology, terminology, and clinical applications of optical coherence tomography: physical principles, methodology of image acquisition, and clinical application for assessment of coronary arteries and atherosclerosis. Eur Heart J. 2010;31:401.
55. Yamaguchi T, Terashima M, Akasaka T, et al. Safety and feasibility of an intravascular optical coherence tomography wire system in the clinical setting. Am J Cardiol. 2008;101:562-567.
56. Marti V, Martin V, Garcia J, et al. Significance of angiographic coronary dissection after cutting balloon angioplasty. Am J Cardiol. 1998;81:1349-1352.
57. Litvack F, Eigler N, Margolis J, et al. Percutaneous excimer laser coronary angioplasty: results in the first consecutive 3,000 patients. The ELCA Investigators. J Am Coll Cardiol. 1994;23:323-329.
58. Vaquerizo B, Serra A, Miranda F, et al. Aggressive plaque modification with rotational atherectomy and/or cutting balloon before drug-eluting stent implantation for the treatment of calcified coronary lesions. J Interv Cardiol. 2010;23:240-248.
59. Sharma SK, Kini A, Mehran R, et al. Randomized trial of rotational atherectomy versus balloon angioplasty for diffuse in-stent restenosis (ROSTER). Am Heart J. 2004;147:16-22.
60. Yin W. Rotational atherectomy: an update. J Geriatr Cardiol. 2013;10:211-212.
61. Jiang J, Sun Y, Xiang M, et al. Complex coronary lesions and rotational atherectomy: one hospital’s experience. J Zhejiang Univ-Sci B. 2012;13:645-651.
62. Vidovich M. Drug-eluting stents and rotational atherectomy — “no ‘roto’ regret.” J Invasive Cardiol. 2011;23:140.
63. Schwartz B, Mayeda G, Economides C, et al. Rotational atherectomy in the drug-eluting stent era: a single-center experience. J Invasive Cardiol. 2011;23:133-139.
64. Chen C, Hsieh I. Application of rotational atherectomy in the drug-eluting stent era. J Geriatr Cardiol. 2013;10:213-216.
65. Abdel-Wahab M, Richardt G, Joachim Buttner H, et al. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions – the ROTAXUS trial. JACC Cardiovasc Interv. 2013;6:10-19. Epub 2012 Dec 19.
66. Abdelmeguid AE, Topol EJ, Whitlow PL, et al. Significance of mild transient release of creatine kinase-MB fraction after percutaneous coronary interventions. Circulation. 1996;94:1528-1536.
67. Kong TQ, Davidson CJ, Meyers SN, et al. Prognostic implication of creatine kinase elevation following elective coronary artery interventions. JAMA. 1997;277:461-466.
68. Chiang M, Yi H, Tsao C, et al. Rotablation in the treatment of high-risk patients with heavily calcified left-main coronary lesions. J Geriatr Cardiol. 2013;10:217-225.
69. Reisman M, Harms V, Whitlow P, et al. Comparison of early and recent results with rotational atherectomy. J Am Coll Cardiol. 1997;29:353-357.
70. Matsuo H, Watanabe S, Watanabe T, et al. Prevention of no-reflow/slow-flow phenomenon during rotational atherectomy — a prospective randomized study comparing intracoronary continuous infusion of verapamil and nicorandil. Am Heart J. 2007;154:1-6.
71. Lin CP, Wang JH, Lee WL, et al. Mechanism and management of burr entrapment: a nightmare of interventional cardiologists. J Geriatr Cardiol. 2013;10:230-234.
72. Parikh K, Parikh R, Patel A, et al. Three years follow-up data demonstrate safe and effective treatment of de novo calcified coronary lesions by orbital atherectomy system. JACC Cardiovasc Interv. 2013;6:S41.
73. Parikh K, Chandra P, Choksi N, Khanna P, Chambers J. Safety and feasibility of orbital atherectomy for the treatment of calcified coronary lesions: the ORBIT I trial. Catheter Cardiovasc Interv. 2013;81:1134-1139. Epub 2013 Mar 5.
74. McEvoy J, Blaha M, Defilippis A, et al. Coronary artery calcium progression: an important clinical measurement? J Am Coll Cardiol. 2010;56:1613-1622.
75. Schoen F. Blood vessels. In: Robbins and Cotran Pathologic Basis of Disease. 7th ed. Philadelphia: Elsevier Saunders; 2005:520.
76. Lentini J, Kaka A, Chaudhry H. Atherectomy devices. Digital image. Atherectomy devices — orbital atherectomy. Brown University.
____________________________________________________
From the UCLA Medical Center, Los Angeles, California.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted May 27, 2014, provisional acceptance given June 15, 2014, final version accepted July 29, 2014.
Address for correspondence: Dr Michael S. Lee, 100 Medical Plaza, Suite 630, Los Angeles, CA 90095. Email: mslee@mednet.ucla.edu











