

An Isolated Single L-I type Coronary Artery with Severe LAD Lesions Treated by Transradial PCI
 ABSTRACT: Cases of coronary arteries with anomalous aortic origin are rare. An isolated single coronary artery is a congenital anomaly occurring in approximately 0.024–0.066% of the population. Atherosclerosis of these arteries is not infrequent with potentially severe consequences, but interventional procedures are rarely performed. We report an acute coronary syndrome case due to a subtotal paraostial left anterior descending (LAD) occlusion of a single L-I type coronary artery. Another severe stenosis was also present at mid-LAD. The patient was successfully treated with transradial percutaneous coronary intervention (PCI). Our case shows that when the anatomy is suitable, complex PCI can be performed successfully in single coronary arteries.
ABSTRACT: Cases of coronary arteries with anomalous aortic origin are rare. An isolated single coronary artery is a congenital anomaly occurring in approximately 0.024–0.066% of the population. Atherosclerosis of these arteries is not infrequent with potentially severe consequences, but interventional procedures are rarely performed. We report an acute coronary syndrome case due to a subtotal paraostial left anterior descending (LAD) occlusion of a single L-I type coronary artery. Another severe stenosis was also present at mid-LAD. The patient was successfully treated with transradial percutaneous coronary intervention (PCI). Our case shows that when the anatomy is suitable, complex PCI can be performed successfully in single coronary arteries.
J INVASIVE CARDIOL 2011;23:E216–E218
Key words: acute coronary syndrome, single coronary artery
______________________________________
 Case Report. A 68-year-old male patient was admitted with progressive effort dyspnea. He was dyslipidemic and hypertensive with a family history of coronary artery disease and otherwise unremarkable medical history. His ECG showed normal sinus rhythm with negative T waves on leads I, aVL, V4-V6. On echocardiography, the left ventricle had anteroseptal and apical hypokinesia, ejection fraction 35%, and pseudonormalized filling.
Case Report. A 68-year-old male patient was admitted with progressive effort dyspnea. He was dyslipidemic and hypertensive with a family history of coronary artery disease and otherwise unremarkable medical history. His ECG showed normal sinus rhythm with negative T waves on leads I, aVL, V4-V6. On echocardiography, the left ventricle had anteroseptal and apical hypokinesia, ejection fraction 35%, and pseudonormalized filling.
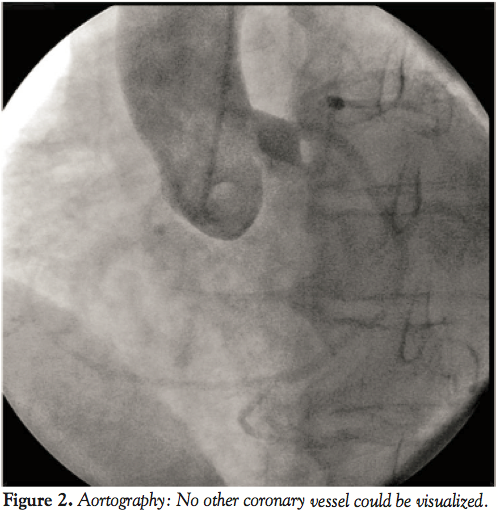
Coronary angiography performed via a right radial artery approach revealed a single coronary artery (SCA) originating from the left sinus of Valsalva (L-I type) (Figure 1). No other coronary artery was noted on aortography (Figure 2). The left main was very short; the LAD and circumflex had separate ostia. The LAD had a paraostial subtotal occlusion and another focal 80% stenosis at its mid segment (Figures 3 and 4). A superdominant circumflex artery, after supplying the posterior descending branch, continued its course along the right posterior atrioventricular groove providing branches for the right ventricle and right atrium.
revealed a single coronary artery (SCA) originating from the left sinus of Valsalva (L-I type) (Figure 1). No other coronary artery was noted on aortography (Figure 2). The left main was very short; the LAD and circumflex had separate ostia. The LAD had a paraostial subtotal occlusion and another focal 80% stenosis at its mid segment (Figures 3 and 4). A superdominant circumflex artery, after supplying the posterior descending branch, continued its course along the right posterior atrioventricular groove providing branches for the right ventricle and right atrium.
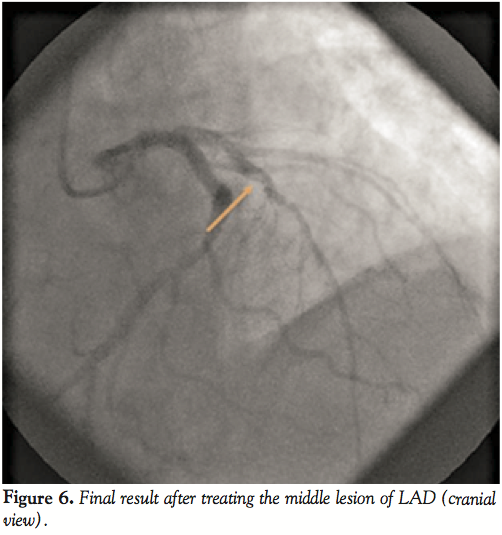
 Ad hoc percutaneous coronary intervention (PCI) was performed maintaining the right radial approach. A 6 French (Fr) JL 3.5 guiding catheter (Cordis Europa NV) was chosen. The LAD lesions were crossed with a Pilot 50 guidewire (Abbott Vascular). The LAD paraostial lesion was predilated with a Sprinter 2 x 10 mm balloon (Medtronic) and an Endeavor Resolute 4 x 18 mm stent (Medtronic) was successfully implanted at 16 atm (Figure 4). Better visualization of the mid-LAD lesion was achieved and permitted direct implantation of a Nobori 3 x 14 mm stent (Terumo) at 16 atm to achieve an excellent angiographic result (Figure 5). The patient had no troponin elevation post-procedure and was discharged uneventfully after 2 days. One month later he reported symptomatic improvement (no effort dyspnea) and his ejection fraction increased from 35% to 45%. Six months after the procedure he was completely asymptomatic.
Ad hoc percutaneous coronary intervention (PCI) was performed maintaining the right radial approach. A 6 French (Fr) JL 3.5 guiding catheter (Cordis Europa NV) was chosen. The LAD lesions were crossed with a Pilot 50 guidewire (Abbott Vascular). The LAD paraostial lesion was predilated with a Sprinter 2 x 10 mm balloon (Medtronic) and an Endeavor Resolute 4 x 18 mm stent (Medtronic) was successfully implanted at 16 atm (Figure 4). Better visualization of the mid-LAD lesion was achieved and permitted direct implantation of a Nobori 3 x 14 mm stent (Terumo) at 16 atm to achieve an excellent angiographic result (Figure 5). The patient had no troponin elevation post-procedure and was discharged uneventfully after 2 days. One month later he reported symptomatic improvement (no effort dyspnea) and his ejection fraction increased from 35% to 45%. Six months after the procedure he was completely asymptomatic.
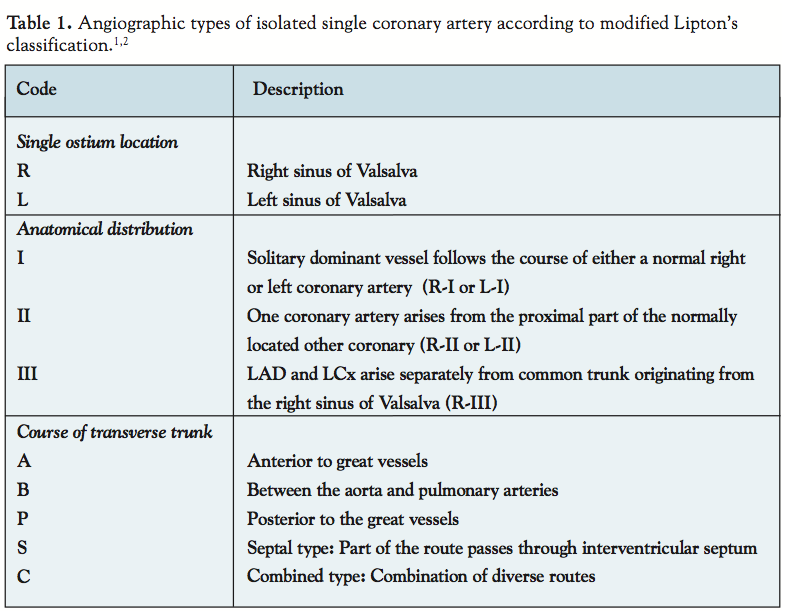
 Discussion. A SCA is a rare congenital anomaly, being an isolated finding in 0.024% to 0.066% of adults undergoing coronary angiography.1,2,3 Isolated SCA angiographic subtypes are categorized by modified Lipton’s classification (Table 1).1,2 Their clinical presentation may be anginal chest pain or syncope, especially with exercise, cardiomyopathy, and myocardial infarction.1,2,3 Unfortunately, the initial manifestation may be sudden death, particularly in young athletes, with the R-II-B subtype being mostly notorious for such events.4 According to Shirani’s review, 15% of patients with isolated SCA had evidence of myocardial ischemia without significant atherosclerotic stenosis.5 When atherosclerotic disease develops, its consequences can be much more severe. Disease location, morphology, and extent, along with the extent of jeopardized myocardium must be considered to select the appropriate revascularization method. The affected anomalous vessels are technically difficult to perform surgical grafting. Performing PCI of a SCA has an additional risk for serious complications. Occlusion of the ballooning site due to dissection or thrombus could provoke ischemia to a significant amount of myocardium, while dissection of the single ostium (e.g., guiding-catheter induced) may be catastrophic.6
Discussion. A SCA is a rare congenital anomaly, being an isolated finding in 0.024% to 0.066% of adults undergoing coronary angiography.1,2,3 Isolated SCA angiographic subtypes are categorized by modified Lipton’s classification (Table 1).1,2 Their clinical presentation may be anginal chest pain or syncope, especially with exercise, cardiomyopathy, and myocardial infarction.1,2,3 Unfortunately, the initial manifestation may be sudden death, particularly in young athletes, with the R-II-B subtype being mostly notorious for such events.4 According to Shirani’s review, 15% of patients with isolated SCA had evidence of myocardial ischemia without significant atherosclerotic stenosis.5 When atherosclerotic disease develops, its consequences can be much more severe. Disease location, morphology, and extent, along with the extent of jeopardized myocardium must be considered to select the appropriate revascularization method. The affected anomalous vessels are technically difficult to perform surgical grafting. Performing PCI of a SCA has an additional risk for serious complications. Occlusion of the ballooning site due to dissection or thrombus could provoke ischemia to a significant amount of myocardium, while dissection of the single ostium (e.g., guiding-catheter induced) may be catastrophic.6
 In the largest series examining coronary anomalies in 126,595 patients submitted to coronary angiography, the L-I subtype had an incidence of 0.016%, 1.2% consisting of all coronary anomalies.2 The L-I subtype is generally considered benign and usually treated medically.2 The L-I SCA subtype has been rarely reported.7 Chou et al reported one and reviewed 11 previous cases.7 Coronary atherosclerosis existed in 9 out of 12 cases (75%) and CABG was advocated in 4 (33.3%), while the rest were treated medically.7 Another case treated medically was reported recently.8 Few reports have described PCI in patients with isolated SCAs, the majority concerning R subtypes.9 Takano et al reported PCI for a mid-LAD lesion of a SCA arising from the left sinus of Valsalva, where the right coronary artery originated from the mid-LAD through the transverse branch.10 To the best of our knowledge, our case is the first report of a successful PCI for an L-I type SCA. In our patient the left main was short and had a very large caliber. This rendered guide catheter positioning and lesion crossing technically challenging, but the risk of guiding catheter-induced damage was low. The superdominant circumflex had a practically separate ostium with a low probability of compromise during PCI.
In the largest series examining coronary anomalies in 126,595 patients submitted to coronary angiography, the L-I subtype had an incidence of 0.016%, 1.2% consisting of all coronary anomalies.2 The L-I subtype is generally considered benign and usually treated medically.2 The L-I SCA subtype has been rarely reported.7 Chou et al reported one and reviewed 11 previous cases.7 Coronary atherosclerosis existed in 9 out of 12 cases (75%) and CABG was advocated in 4 (33.3%), while the rest were treated medically.7 Another case treated medically was reported recently.8 Few reports have described PCI in patients with isolated SCAs, the majority concerning R subtypes.9 Takano et al reported PCI for a mid-LAD lesion of a SCA arising from the left sinus of Valsalva, where the right coronary artery originated from the mid-LAD through the transverse branch.10 To the best of our knowledge, our case is the first report of a successful PCI for an L-I type SCA. In our patient the left main was short and had a very large caliber. This rendered guide catheter positioning and lesion crossing technically challenging, but the risk of guiding catheter-induced damage was low. The superdominant circumflex had a practically separate ostium with a low probability of compromise during PCI.
 In general PCI of a SCA is very similar to PCI of unprotected left main. The question remains: Do patients with SCA who underwent PCI need an intra-aortic balloon pump (IABP)? An IABP is used in patients with left main coronary stenosis, cardiogenic shock, refractory ischemia, and mechanical complications of acute myocardial infarction (e.g., ruptured papillary muscle or ventricular septal defect). Despite the reports of no improvement in flow across critical lesions,11 IABP is still associated with clinical benefits, particularly in patients at high risk during angioplasty.12 However, in a work by Vijayalakshmi et al,13 in high-risk, non-shock patients, it was unclear whether IABP provided any benefit to non-shock patients and that the potential benefit of IABP does not appear to be associated with early improvement in angiographically-determined coronary flow. Our patient was stable and the superdominant circumflex had a practically separate ostium, so we did not use prophylactic IABP.
In general PCI of a SCA is very similar to PCI of unprotected left main. The question remains: Do patients with SCA who underwent PCI need an intra-aortic balloon pump (IABP)? An IABP is used in patients with left main coronary stenosis, cardiogenic shock, refractory ischemia, and mechanical complications of acute myocardial infarction (e.g., ruptured papillary muscle or ventricular septal defect). Despite the reports of no improvement in flow across critical lesions,11 IABP is still associated with clinical benefits, particularly in patients at high risk during angioplasty.12 However, in a work by Vijayalakshmi et al,13 in high-risk, non-shock patients, it was unclear whether IABP provided any benefit to non-shock patients and that the potential benefit of IABP does not appear to be associated with early improvement in angiographically-determined coronary flow. Our patient was stable and the superdominant circumflex had a practically separate ostium, so we did not use prophylactic IABP.
Our case demonstrates that PCI may be a credible therapeutic option in SCA cases, particularly when prompt treatment of critical lesions is expected to improve patient outcome.
References
- Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: Diagnosis, angiographic classification, and clinical significance. Radiology 1979;130(1):39-47.
- Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 1990;21(1):28-40.
- Desmet W, Vanhaecke J, Vrolix M, et al. Isolated single coronary artery: A review of 50,000 consecutive coronary angiographies. Eur Heart J 1992;13(12):1637-1640.
- Basso C, Maron BJ, Corrado D, Thiene G. Clinical profile of congenital coronary artery anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive athletes. J Am Coll Cardiol 2000;35(6):1493-1501.
- Shirani J, Roberts WC. Solitary coronary ostium in the aorta in the absence of other major congenital cardiovascular anomalies. J Am Coll Cardiol 1993;21(1):137-143.
- Geyik B, Ozeke O, Deveci B, et al. Single coronary artery presenting with cardiogenic shock due to acute myocardial infarction. Int J Cardiovasc Imaging 2006;22(1):5-7.
- Chou LP, Kao C, Lee MC, Lin SL. Right coronary artery originating from distal left circumflex artery in a patient with an unusual type of isolated single coronary artery. Jpn Heart J 2004;45(2):337-342.
- Valencia J, Ruiz-Nodar JM, Bordes P, Pineda J. Isolated single left coronary artery. Int J Cardiol 2007;122(1):66-67.
- Furbatto F, Esposito G, Piccolo R, et al. Coronary angioplasty with stenting for acute coronary syndrome in patients with isolated single coronary artery: A report of two cases. J Cardiovasc Med (Hagerstown) 2009;10(7):550-553.
- Takano M, Seimiya K, Yokoyama S, et al. Unique single coronary artery with acute myocardial infarction: Observation of the culprit lesion by intravascular ultrasound and coronary angioscopy. Jpn Heart J 2003;44(2):271-276.
- Yoshitani H, Akasaka T, Kaji S, et al. Effects of intra-aorta balloon counterpulsation on coronary pressure in patients with stenotic coronary arteries. Am Heart J. 2007;154:725-731.
- Briguori C, Airoldi F, Chieffo A, et al. Elective versus provisional intraaortic balloon pumping in unprotected left main stenting. Am Heart J 2006;152(3):565-572.
- Vijayalakshmi K, Kunadian B, Whittaker VJ, et al. Intra-aortic counterpulsation does not improve coronary flow early after PCI in a high-risk group of patients: Observations from a randomized trial to explore its mode of action. J Invasive Cardiol 2007;19:339-346.
______________________________________
From the Cardiology Department, Kat General Hospital Athens, Athens, Greece.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. No authors reported conflicts regarding the content herein.
Manuscript submitted December 20, 2010, provisional acceptance given January 6, 2011, final version accepted February 1, 2011.
Address for correspondence: Dr. Nikos Kafkas, MD, 10, Zitsis, Marousi Att. Athens, 151 25. Email: kafkasncard@yahoo.gr











