

Novel Crossing System for the Recanalization of Complex Chronic Total Occlusions: Ex vivo Proof of Concept of the SoundBite Crossing System
Abstract: Chronic total occlusion (CTO) lesions are frequent in patients with peripheral and coronary artery disease, and associated with a higher risk of adverse events, including mortality, decreased quality of life, and increased health-care costs. Percutaneous intervention of CTO lesions has been associated with a lower procedural success rate, and current dedicated CTO devices may be of limited use for the non-CTO expert, and associated with increased intraprocedural complication rates. The SoundBite Crossing System (SoundBite Medical Solutions, Inc) is a newly developed device using shockwaves (short-duration, high-amplitude pressure pulses) to facilitate penetration of the proximal cap and crossing of the occlusion. The current report describes the first use of the SoundBite Crossing System in the recanalization of human ex vivo occluded arteries below the knee during a simulated procedure performed under fluoroscopy. Microcomputed tomography and histologic evaluation of the occluded and recanalized segment are provided to support therapeutic mechanism.
J INVASIVE CARDIOL 2017;29(4):E47-E50.
Key words: new device, chronic total occlusion
Chronic total occlusion (CTO) lesions are frequent in patients with peripheral and coronary artery disease, representing between 20% and 50% of treated lesions by transcatheter technique.1,2 Percutaneous intervention of CTO lesions has been associated with a lower procedural success rate; however, leaving these lesions untreated is associated with a higher risk of adverse events, including increased mortality, decreased quality of life, and increased health-care costs.3,4 Despite recent advancements in endovascular techniques and the development of dedicated devices to facilitate wire crossing of CTO lesions, procedural failure remains high.1,5 More importantly, most of these devices are challenging to use, and these techniques are associated with higher rates of procedural complications (eg, perforation, tamponade), precluding their wide adoption by operators who are not CTO experts, pointing toward the need for more intuitive, safe, and user-friendly devices.
The SoundBite Crossing System (SoundBite Medical Solutions, Inc) is a newly developed device using shockwaves (short-duration, high-amplitude pressure pulses) to facilitate penetration of the proximal cap and crossing of the occlusion. The system comprises two main components: a disposable wire (ShockWire) and a console (SoundBite Console) that generates shockwaves. Shockwaves have successfully been used in various medical therapies (kidney stone lithotripsy, treatment of chronic joint disorder, bone healing, and treatment of bone necrosis) and have shown the ability to selectively break calcium deposits without damaging surrounding healthy elastic tissue.
The current report describes the first use of the SoundBite Crossing System in the recanalization of human ex vivo occluded arteries below the knee during a simulated procedure performed under fluoroscopy.
SoundBite Crossing System Characteristics. The SoundBite Crossing System uses a novel generator to produce shockwaves that are initially concentrated in the proximal end of a guidewire-like device. The shockwaves are then propagated to the distal tip of the ShockWire, resulting in a “micro jackhammer” effect (short distal tip displacement), which facilitates the passage of the device across the CTO.
The SoundBite Console converts electric power into pressure waves through the use of broadband piezoelectric transducers. Multiple amplification stages are used to increase the wave amplitude. The shockwave emission is pulsed at a low repetition rate (<50 Hz), which limits heat generation. The ShockWire is similar in design to commercially available guidewires, but has the ability to transmit shockwaves across its length. The ShockWire is currently available in 0.014˝ and 0.018˝ platforms to treat CTO lesions in both coronary and peripheral vessels.
Previous bench testing using a vascular model and surrogate materials has demonstrated the efficacy and technical performance of the SoundBite Crossing System. This energy form has also been shown to be safe when used in vivo on healthy tissue [data on file at SoundBite Medical]. Preliminary data using an earlier version of the device in an ex vivo setting under direct visualization showed that the SoundBite Crossing System was successful in crossing short CTO segments obtained from lower-limb amputations when held still by external means. These segments could not be crossed by a stiff wire or the inactivated ShockWire (Video 1).
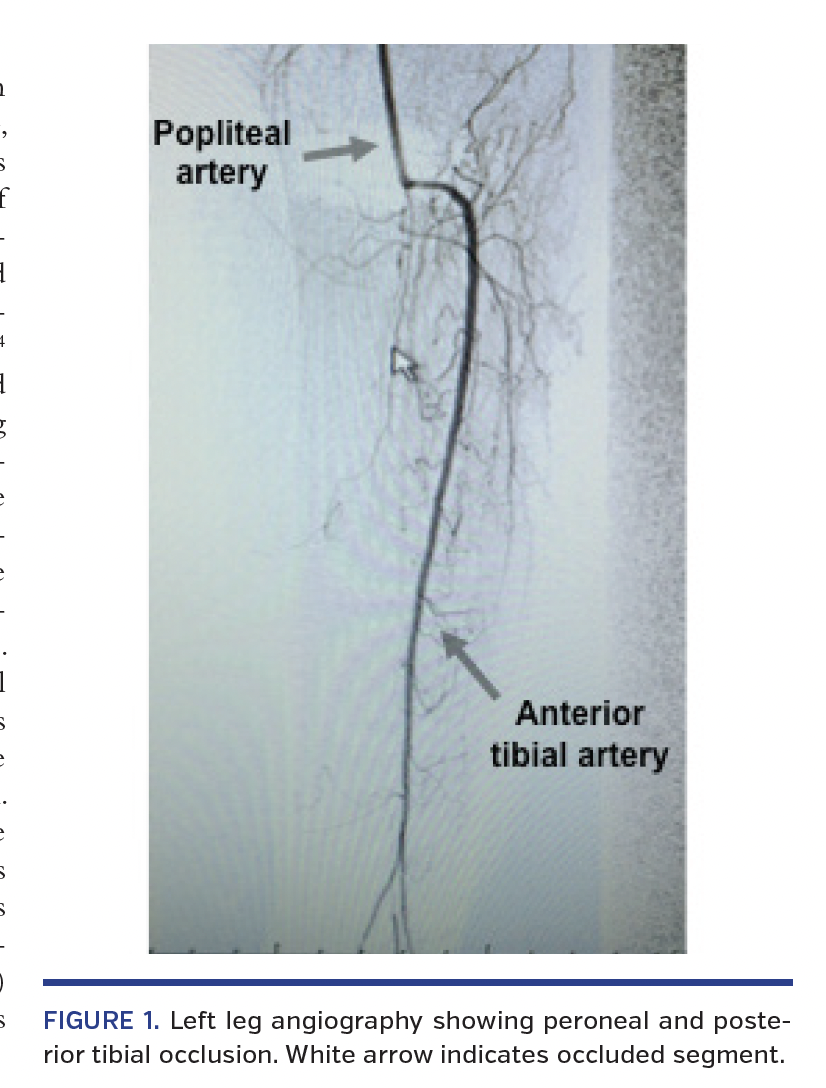
 Ex vivo case simulation description. The aim of the current study was to demonstrate the capacity of the SoundBite Crossing System to penetrate and successfully cross an occluded artery segment of an amputated leg. This case study was approved by the institutional research board and ethics committee of the Centre de recherche du Centre Hospitalier Universitaire de Sherbrooke in Québec, Canada. In this ex vivo case simulation, the occluded arterial segment was harvested from an 88-year-old woman who presented with stage IV arterial insufficiency and who initially underwent a failed angioplasty and subsequently underwent an amputation of her left leg above the knee. The angiogram at the time of presentation demonstrated complete occlusion of the peroneal and posterior tibial arteries (Figure 1).
Ex vivo case simulation description. The aim of the current study was to demonstrate the capacity of the SoundBite Crossing System to penetrate and successfully cross an occluded artery segment of an amputated leg. This case study was approved by the institutional research board and ethics committee of the Centre de recherche du Centre Hospitalier Universitaire de Sherbrooke in Québec, Canada. In this ex vivo case simulation, the occluded arterial segment was harvested from an 88-year-old woman who presented with stage IV arterial insufficiency and who initially underwent a failed angioplasty and subsequently underwent an amputation of her left leg above the knee. The angiogram at the time of presentation demonstrated complete occlusion of the peroneal and posterior tibial arteries (Figure 1).
The popliteal, posterior tibial, and peroneal arteries were dissected from the leg by a vascular surgeon immediately after the amputation. The specimen was preserved in saline at -4°C until the day of the recanalization procedure and then thawed at room temperature for at least 6 hours. The patent popliteal artery was attached to a luer connector at its proximal end, and its principal side branches were sealed using suture and surgical glue. It was then incorporated into a f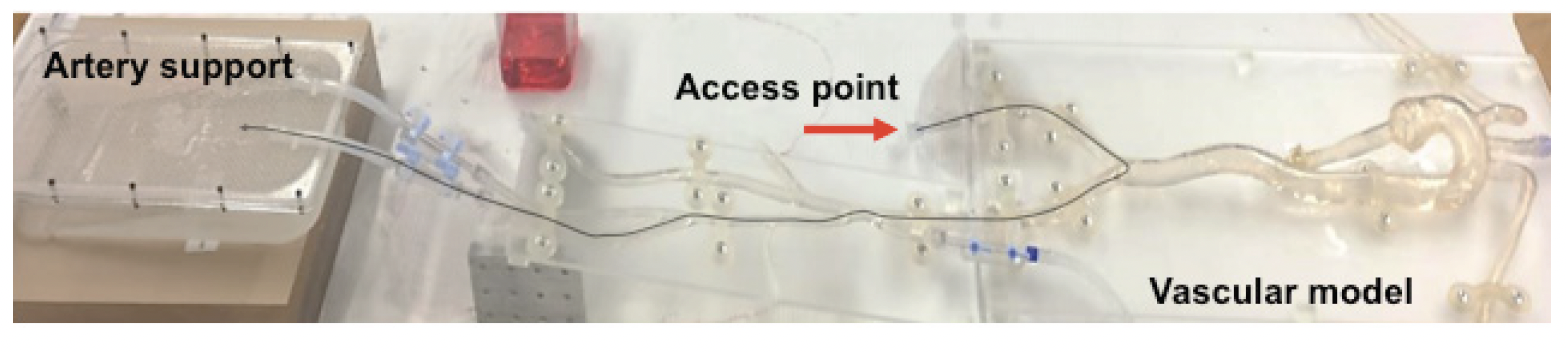
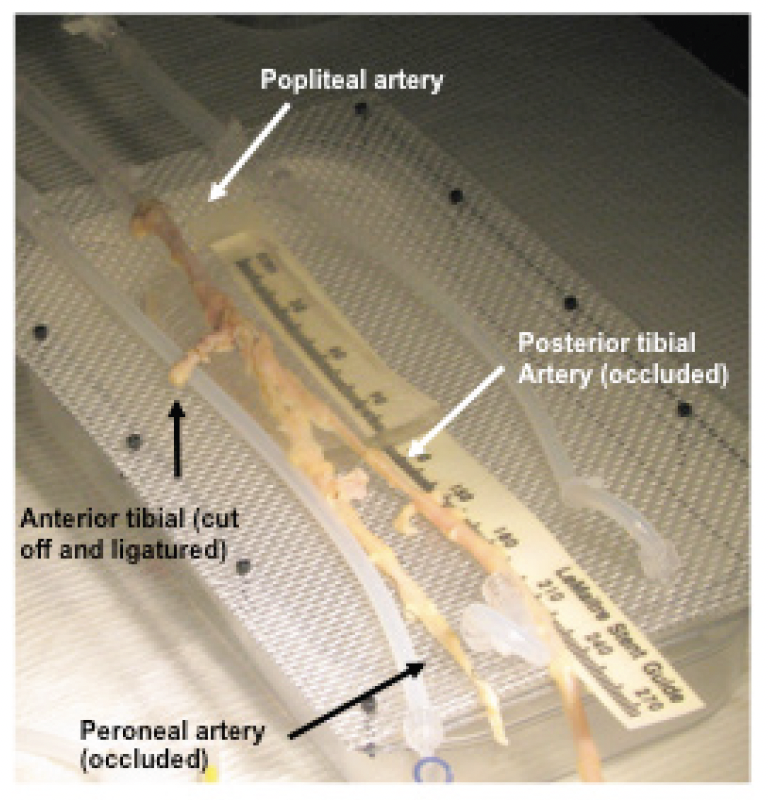
 (Figure 2).
(Figure 2).
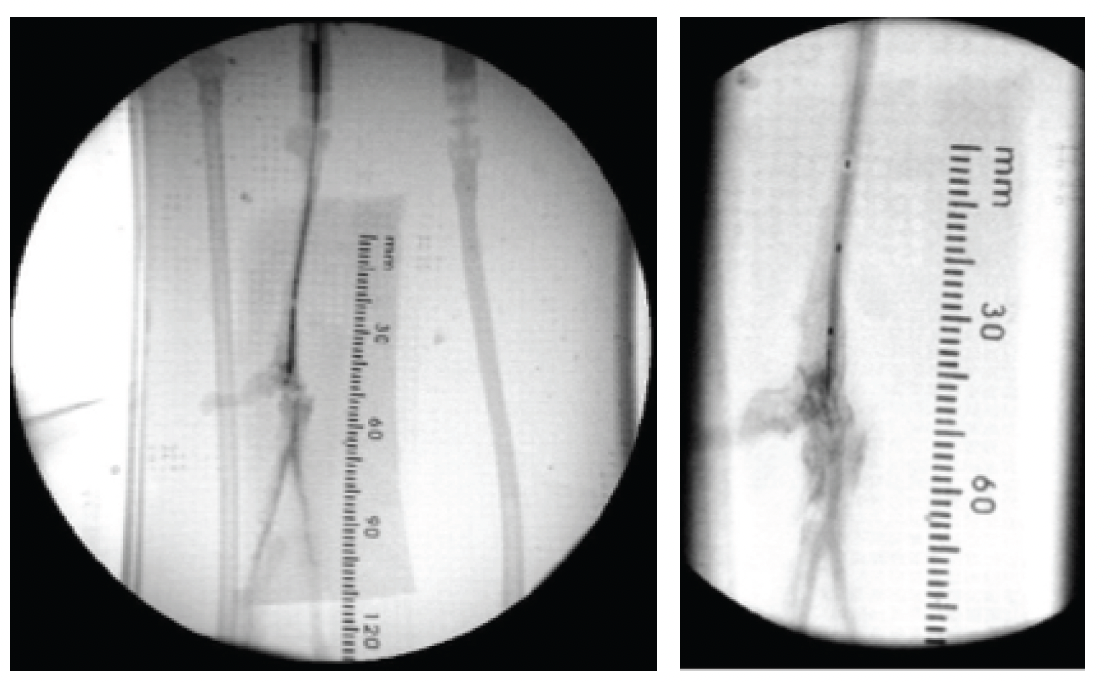
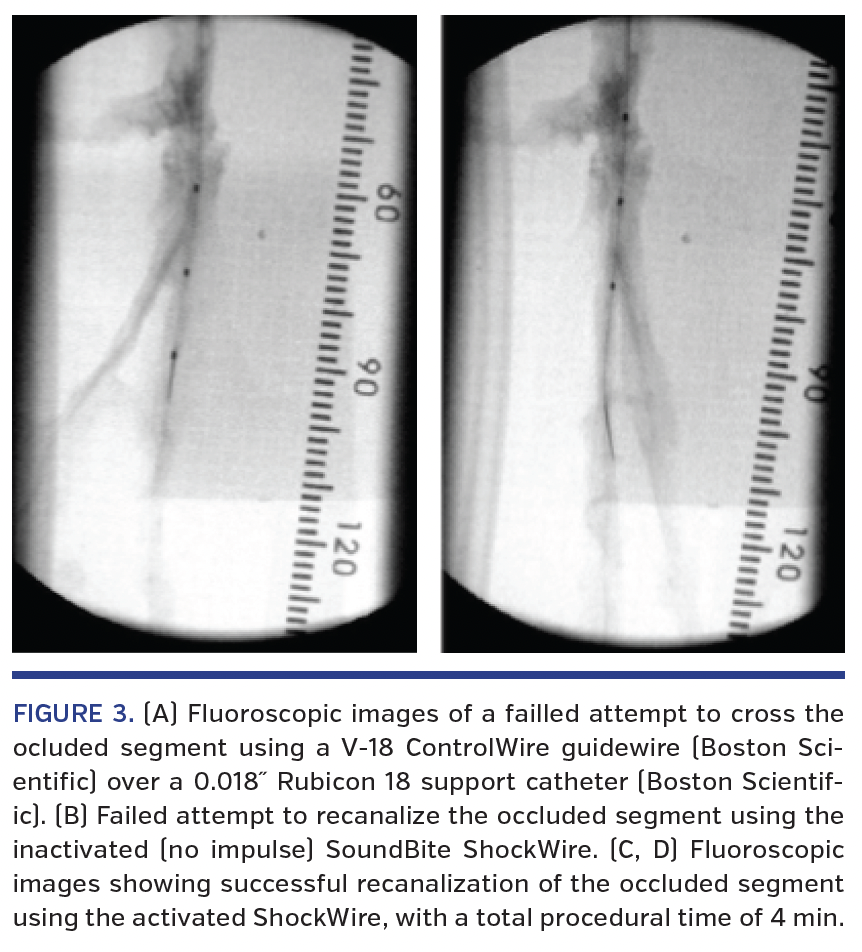
The access site used for the procedure simulated a contralateral approach from the right femoral artery. A guiding catheter was brought through the access site over to the left femoral artery up to the connection point between the vascular model and the connected popliteal artery. Under fluoroscopy and using contrast injection, an attempt to cross the occlusion was  performed without success using a V-18 ControlWire guidewire (Boston Scientific) over an 0.018˝ Rubicon 18 support catheter (Boston Scientific) (Figure 3A). A second unsuccessful attempt was made with the SoundBite Crossing System without activation (no shockwave transmitted; Figure 3B).
performed without success using a V-18 ControlWire guidewire (Boston Scientific) over an 0.018˝ Rubicon 18 support catheter (Boston Scientific) (Figure 3A). A second unsuccessful attempt was made with the SoundBite Crossing System without activation (no shockwave transmitted; Figure 3B).
Recanalization was then attempted using the activated SoundBite Crossing System, resulting in recanalization of both the occluded posterior tibial and peroneal arteries (total procedure time, 4 min) (Figures 3C and 3D).
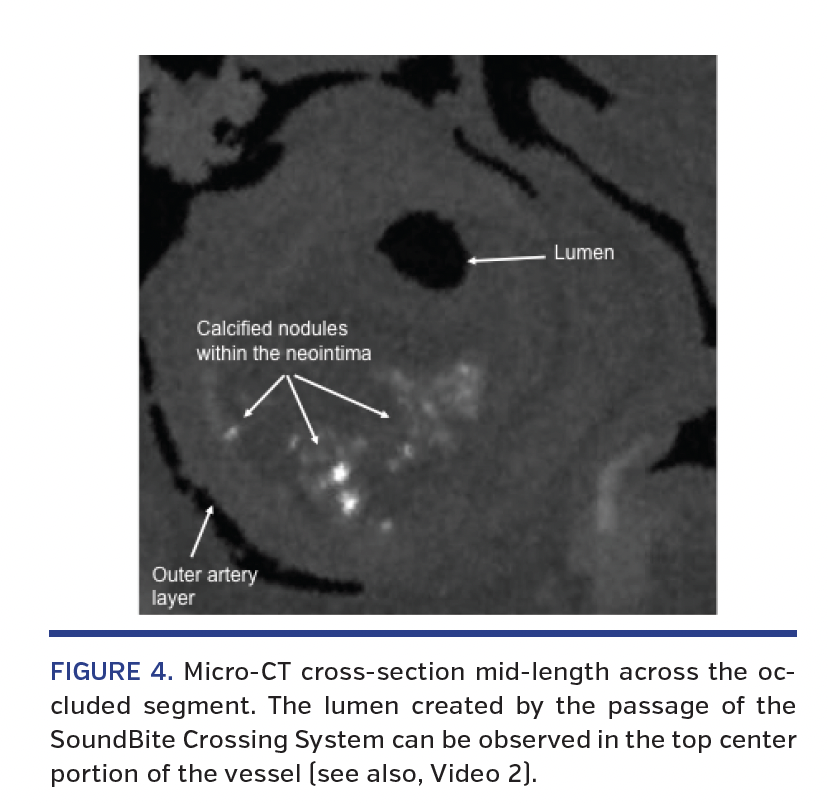
Micro-CT and histologic evaluation of occluded segment. Immediately following the procedure, the arterial segment was preserved (-4°C saline) and micro-CT and histology evaluation were performed. The micro-CT evaluation was done using an XT H 225 micro-CT instrument (Nikon Metrology, Inc) with spatial reconstruction by the CT Pro 3D software (Nikon Metrology, Inc). The images showed an area of important intraluminal stenosis throughout the middle and distal portions of the sample; however, a lumen was visible through most of the studied area associated with the passage of the ShockWire (Figure 4; Video 2). Highly radiodense material suggesting mineralization was also observed scattered along the artery, in and out of the region of interest. Most of it was small and located in the deep neointimal or medial arterial layer. Also, one major homogenous mineralized area appeared just proximal to the occlusion previously described.
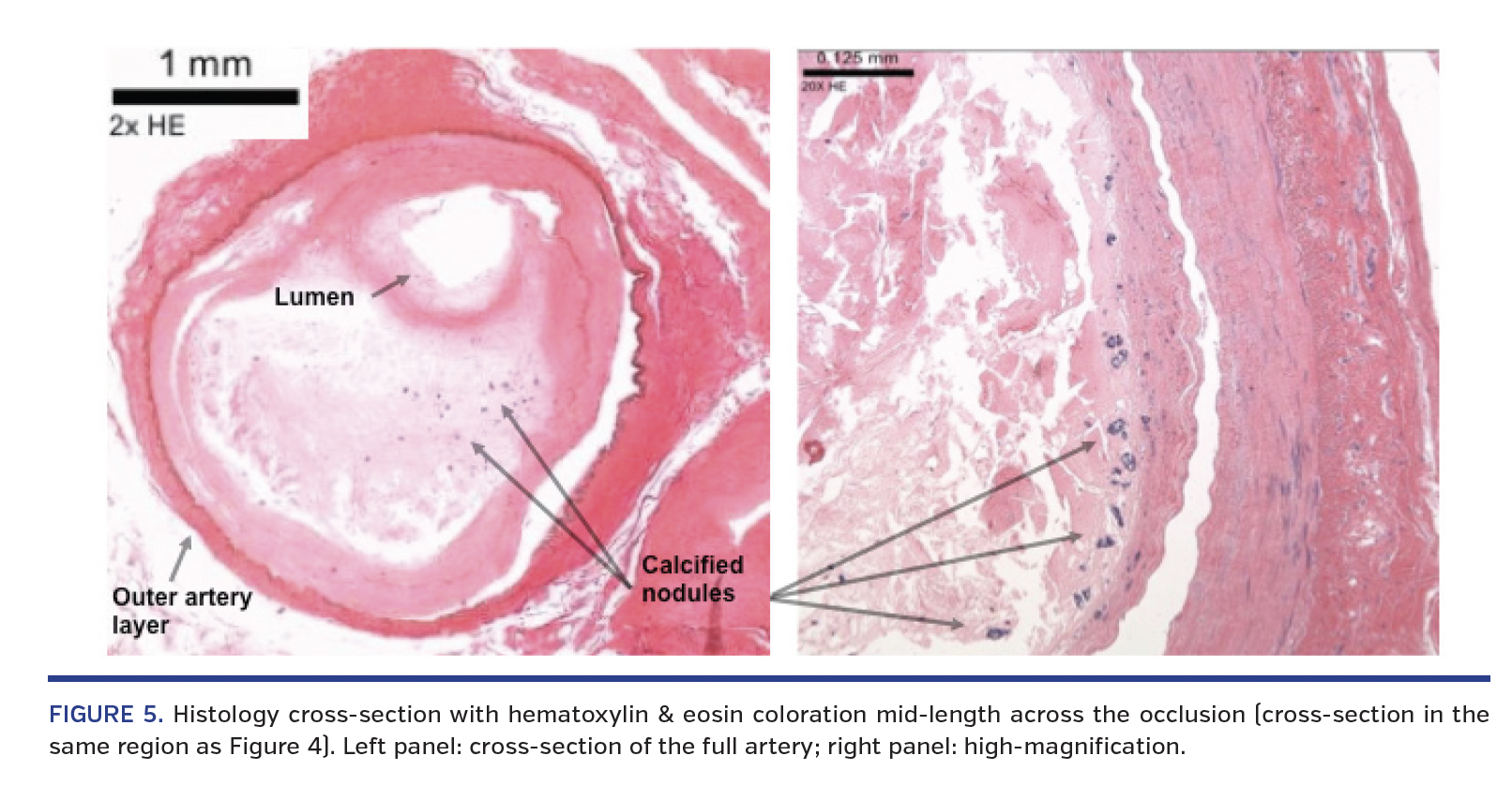
Histologic evaluation was performed on thin sections (approximately 8 µm thick) from the artery prepared and stained with hematoxylin and eosin, Movat pentachrome, and Von Kossa stain. The hematoxylin and eosin stain showed tissue protruding into the lumen mainly composed of neointimal tissue, fibrosis, and area of mineralization (Figure 5). The lumen seen by micro-CT, caused by the device passage, was also found on histologic evaluation confirming a “true to true” recanalization of the occluded vascular segment. Area of mineralization evaluated by Von Kossa stain showed mineralization of the vascular segment, with the most severely mineralized area found just proximal to the bifurcation of the anterior tibial artery from the popliteal artery.
Discussion
The SoundBite Crossing System is the first CTO device using a guidewire-like platform to deliver shockwaves to the point of vascular occlusion. This ex vivo case simulation represents the first report regarding the use of the SoundBite Crossing System for recanalization of complex CTO lesions. Although further human in vivo studies are needed to demonstrate the safety and efficacy of this new device, our report provides a strong demonstration of the capability of the shockwave technology to successfully cross occlusions where prior attempts with conventional wires failed. While still speculative, it allows one to believe that shockwave wire technology may have a predominant role in the management of complex CTO lesions in the future. Ongoing feasibility and pilot studies will provide meaningful information regarding the capability of SoundBite technology to improve procedural success, decrease procedural complication, and simplify CTO procedures, both in coronary and peripheral fields.
Study limitations. Despite our effort to reproduce human vascular anatomy and physiology, SoundBite technology efficacy may be different in vivo compared with ex vivo. While we did not confirm with dye injection intraluminal crossing of the wire, histology and micro-CT imaging of the treated segment confirmed intraluminal recanalization of a severely calcified occluded segment.
Acknowledgments. The authors would like to thank Manuel Charlebois Ménard and Steven Dion for their support throughout this study, and the contributions of AccelLAB (Boisbriand, QC, Canada) for the micro-CT and histology studies.
Watch the associated Video Series here.
References
1. Galassi AR, Brilakis ES, Boukhris M, et al. Appropriateness of percutaneous revascularization of coronary chronic total occlusions: an overview. Eur Heart J. 2016;37:2692-2700.
2. Al-Ameri H, Clavijo L, Matthews RV, Kloner RA, Shavelle DM. Devices to treat peripheral chronic total occlusions. J Interv Cardiol. 2012;25:395-403.
3. Sianos G, Werner GS, Galassi AR, et al. Recanalisation of chronic total coronary occlusions: 2012 consensus document from the EuroCTO club. EuroIntervention. 2012;8:139-145.
4. Wijeysundera HC, Norris C, Fefer P, et al. Relationship between initial treatment strategy and quality of life in patients with coronary chronic total occlusions. EuroIntervention. 2014;9:1165-1172.
5. Galassi AR, Sianos G, Werner GS, et al. Retrograde recanalization of chronic total occlusions in Europe: procedural, in-hospital, and long-term outcomes from the multicenter ERCTO registry. J Am Coll Cardiol. 2015;65:2388-2400.
From the 1Université de Sherbrooke, Sherbrooke, Québec, Canada; 2SoundBite Medical Solutions, Inc; 3Medical University Graz, Graz, Austria; 4Centre Hospitalier de l’Université de Montréal, Montreal, Québec, Canada; 5Metro Heart & Vascular, Wyoming, Michigan; 6Morristown Medical Center, Morristown, New Jersey; 7Hôpital du Sacré-Coeur de Montréal, Université de Montréal, Montréal, Québec, Canada; 8Cardiovascular Research Foundation, New York, New York; and 9NewYork-Presbyterian Hospital/Columbia University Medical Center, New York, New York.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Bérubé is a consultant for Astra Zeneca, Bayer and Mylan; shareholder of Soundbite Medical Solutions, Inc. Dr Benko and Dr Despatis are shareholders in Soundbite Medical Solution, Inc. Dr Therasse is a consultant for Soundbite Medical Solutions, Inc. Dr Brouillette and Dr Riel are employees of Soundbite Medical Solutions, Inc. and report pending related patents. Dr Mustapha is a consultant for Abbott Vascular, Bard, Boston Scientific, Cardiovascular Systems, Inc (CSI), Cook Medical, Medtronic, Spectranetics, and Terumo. Dr Généreux reports speaker fees from Abbott Vascular, CSI, and Edwards Lifesciences; reseach grant from Boston Scientific and CSI; consultant for CSI and Soundbite Medical Solutions Inc; shareholder in Soundbite Medical Solutions, Inc.
Manuscript submitted September 9, 2016 and accepted September 15, 2016.
Address for correspondence: Simon Bérubé, MD, 3001 12e Avenue Nord, Sherbrooke, Québec, Canada, J1H 5N4. Email: simon.berube@usherbrooke.ca













