

A Transradial Approach of Cardiac Catheterization for Patients on Dialysis
Abstract: Background. Periprocedural bleeding is associated with increased risk of early mortality during percutaneous coronary intervention (PCI), especially in patients on dialysis. A transradial approach (TRA) should be considered for these patients; however, PCI operators avoid this approach because of the risk of radial artery occlusion (RAO). The aim of this study is to construct a TRA system and clarify its safety in patients on dialysis. Methods. Eighty-eight consecutive patients on dialysis who underwent cardiac catheterization were prospectively included in this study and divided according to the access site into either the TRA group or the transfemoral approach (TFA) group. Radial access was limited in the opposite side of arteriovenous fistula. The study endpoints were in-hospital and 30-day mortality rates, puncture-site related bleeding complications, and other complications. The study safety endpoints were procedure success rate and RAO rate in the TRA group. Results. Mean patient age was 70.4 ± 8.5 years. PCI was performed in 43 patients (48.9%). The TRA and TFA groups included 62 patients (70.5%) and 26 patients (29.5%), respectively. In-hospital and 30-day mortality rates were 0.0% in both groups. Puncture-site bleeding rates were 3.8% in the TFA group and 0.0% in the TRA group (P=.12). Procedural success rate in the TRA group was 98.4%. Crossover to TFA was necessary in 1 patient due to radial artery spasm. RAO occurred in 4 patients (6.5%). Conclusions. Constructed TRA can be safely used in patients on dialysis. Our study could lead to an increase in TRA in these patients, which would lead to better prognosis and patient comfort.
J INVASIVE CARDIOL 2018;30(6):212-217. Epub 2018 January 15.
Key words: radial approach, hemodialysis, puncture-site bleeding, radial artery occlusion, coronary artery disease, arteriovenous fistula
Periprocedural bleeding is the most common complication of percutaneous coronary intervention (PCI) and is associated with an increased risk of early mortality.1-4 Bleeding avoidance strategies, such as a transradial approach (TRA), should be considered especially for patients with high bleeding risk, because previous studies demonstrated a decreased rate of bleeding complications after PCI performed with TRA.4-6 However, PCI operators hesitate to choose conventional TRA because of the increased risk of radial artery occlusion (RAO) and general tendency to preserve possible hemodialysis access points for the future.7
Previous studies demonstrated that 2-year primary and secondary patency rates of arteriovenous fistula (AVF) were 51% and 64%, respectively, and RAO rates were 1%-10%.8-14 On the other hand, preservation of possible hemodialysis access points for the future is questionable because 5-year survival rate of patients on dialysis is poor (approximately 50%).15,16 Therefore, we considered that TRA would be beneficial for patients on dialysis despite the risk of RAO, because it can reduce bleeding complications and early mortality rates.
The aims of this study were to construct a TRA system and to clarify the feasibility of TRA for patients on dialysis.
Methods
Study design. This study was an ongoing, prospective, cohort study designed to collect clinical background and outcome data related to cardiac catheterization in patients on dialysis. The institutional review board approved the study design. Additionally, a nephrologist (KH) from our institute approved the study design. This study complied with the Declaration of Helsinki. All patients provided written informed consent, including a statement regarding possible RAO, prior to inclusion. Data of approximately 100 patient variables were collected from medical records. Any coronary device could be used to perform PCI. The decision to perform PCI was based on patient clinical assessment by the attending physician. The physician was not restricted to specific interventional or surgical techniques, such as vascular access site (TRA or transfemoral approach [TFA]), sheath size, or use of a specific stent or closure device.
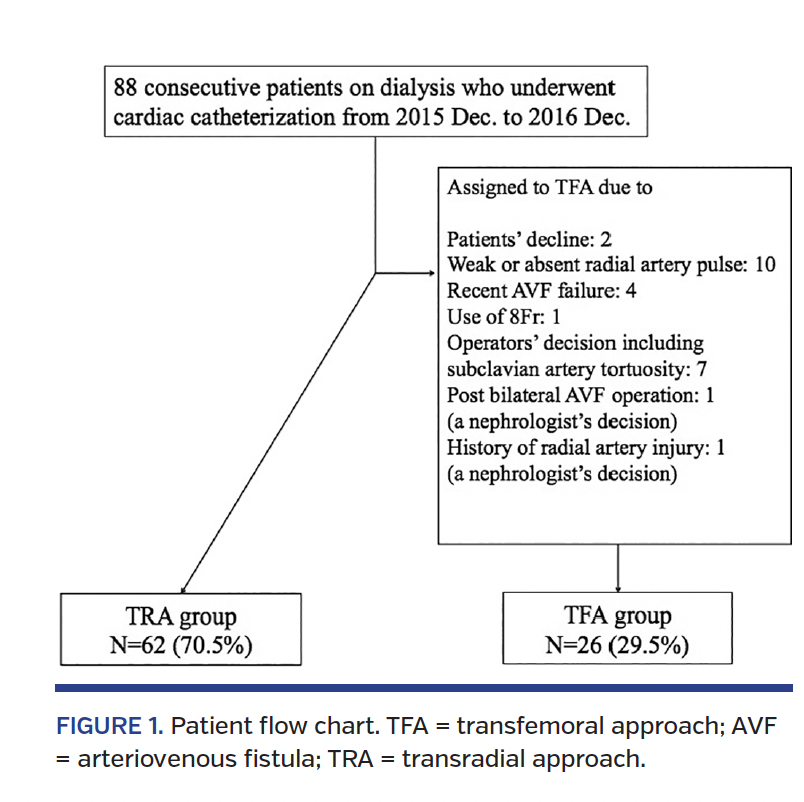
Case selection. Data of 88 consecutive patients on dialysis who underwent cardiac catheterization (diagnostic angiography [DA] or PCI) between December 2015 and December 2016 were analyzed (Figure 1). All patients were divided into two groups according to the access site (TRA group or TFA group). In addition to patients on hemodialysis, patients on peritoneal dialysis were also included, because they usually receive AVF placement within several years.17 Radial access was limited in the opposite side of AVF. The following patients were excluded from the TRA group: (1) patients who did not sign informed consent; (2) patients with weak or absent radial artery pulse; (3) patients on peritoneal dialysis with weak or absent radial artery pulse on one side in order to preserve the other side for future access; (4) recent AVF failure (within 6 months); (5) TFA preferred by operator (eg, for 8 Fr sheath); and (6) nephrologist decision against TRA (Figure 1). Allen’s test was not routinely performed because it was found not to affect hand ischemic complications after the procedure.18 Baseline characteristics and clinical outcomes of patients from both groups were analyzed. The majority of the clinical variables were defined according to the National Cardiovascular Data Registry by the American College of Cardiology.19,20
Procedural information. All patients received periprocedural anticoagulation with heparin. For DA, a bolus of 5000 U was administered. For PCI, additional heparin doses were used to maintain activated clotting time >300 sec.21 At our institute, 6-8 Fr sheaths are used to perform PCI. Sheath size was chosen by the operator; however, smaller sizes (4 Fr) were found favorable,22 especially for DA with TRA. Severe arterial tortuosity was reported by operators when catheter manipulation was affected.23
For the TRA study protocol, Glidesheath Slender (Terumo) was used for 6 Fr and 7 Fr sheaths due to their low profile (the outer diameter of the 6 Fr Glidesheath Slender is close to the 5 Fr sheath) and low RAO rate.24 Before the procedure, radial artery diameter was assessed by ultrasonography (Affiniti 70; Philips). After sheath insertion, 5000 U unfractionated heparin and 0.5–1.0 mg nitroglycerin were administered intra-arterially. All sheaths were removed after the procedures. Radial artery spasm was defined as the inability to advance the arterial sheath or to manipulate the catheters, or spasm resulting in patient discomfort requiring access-site crossover.25
A Bleedsafe hemostatic device (Medikit) was placed around the wrist. The study attempted to achieve “patent hemostasis,” and to decrease RAO rates if possible.13 A pulse oximeter sensor was placed over the index finger, and subsequently the device band was tightened with the inflation of 15 cm3 of air after sheath removal. The ipsilateral ulnar artery was occluded and the band was loosened until plethysmographic signal returned, or bleeding occurred.13 If bleeding occurred, the band was tightened until bleeding stopped. The band was loosened gradually over several hours (DA, 5 hours; PCI, 7 hours). RAO was assessed by Barbeau’s test.13 A pulse-oximeter sensor was placed over the index finger. Radial and ulnar arteries were compressed; subsequently, the radial artery was released. When plethysmographic signal returned, radial artery patency was confirmed. This test was performed 24 hr after the procedure. If RAO was suspected, ultrasonography with duplex Doppler was performed to observe the absence of blood flow, after which RAO was confirmed. These patients were examined at 30 days post procedure because RAO rates at 30 days were reportedly lower than those detected at 24 hours.13
The recommended antiplatelet therapy was long-term aspirin 81 mg daily for ischemic heart disease, combined with a thienopyridine (75 mg clopidogrel or 200 mg ticlopidine daily) if PCI was performed. In general, the loading dose of clopidogrel was 300 mg. By the study protocol, prasugrel was not used due to high bleeding risks in patients on dialysis.26
Outcome measures. The study endpoints were in-hospital and 30-day mortality rates, puncture-site related bleeding complications, and other complications. The study safety endpoints were procedural success rate and RAO rate in the TRA group. Procedural success was defined as completion of a procedure without crossover to other access sites. Puncture-site bleeding consisted of significant external bleeding that occurred at the access or percutaneous entry site that was associated with any of the following: hemoglobin drop >3.0 g/dL;27 need for transfusion; procedural intervention/surgery at the bleeding site to reverse/stop or correct the bleeding; and acute anemia with a reduction in hemoglobin > 3.0 g/dL without other obvious sources or intraprocedural blood loss. Puncture site hematoma was defined as hematoma with a diameter >10 cm for femoral access and >2 cm for radial access. Bleeding criteria were consistent with the Bleeding Academic Research Consortium grades 3A to C.28 Other complications included heart failure, cardiogenic shock, severe coronary dissection or perforation, myocardial infarction after PCI, cardiogenic shock or heart failure, cerebral bleeding or stroke, retroperitoneal bleeding, gastrointestinal bleeding, genitourinary bleeding, or other bleedings.
Statistical analysis. Continuous variables were expressed as means and standard deviations, or median (interquartile range), and categorical variables were expressed as percentages. Continuous variables were compared using the Student’s t-test or Mann-Whitney U-test, and differences between categorical variables were examined using a Chi-square test or Fisher’s exact test. All statistical calculations and analyses were performed using SPSS version 22 (SPSS, Inc), and P<.05 was considered statistically significant.
Results
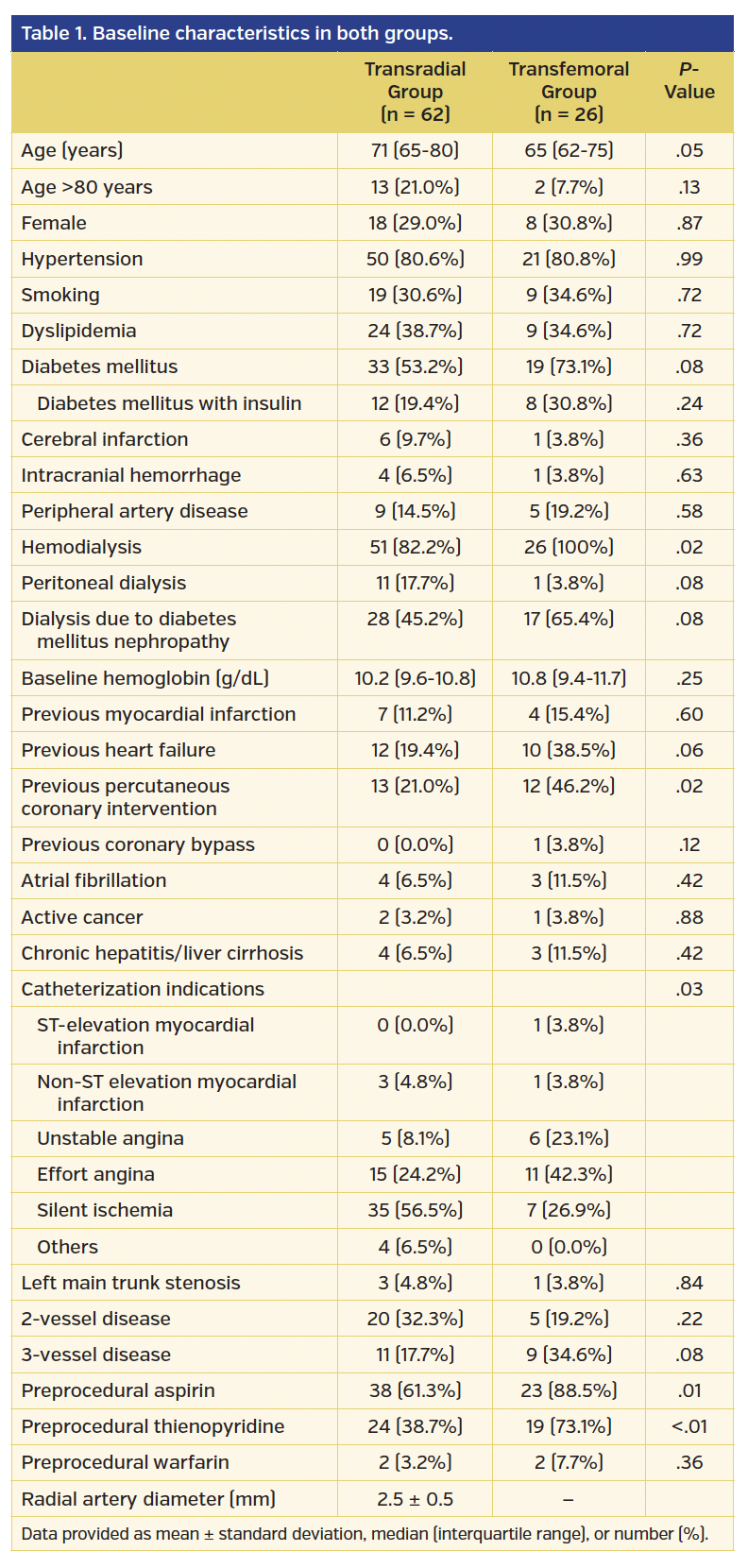
Baseline characteristics. Overall, mean age was 70.4 ± 8.5 years, and 26 patients (29.5%) were female. Of these patients, 11 patients (11.4%) had acute coronary syndromes and PCI was performed in 43 patients (48.9%). The TRA group included 62 patients (70.5%), whereas the TFA group included 26 patients (29.5%). Baseline clinical data for both groups are detailed in Table 1. No significant differences in sex, age, and comorbidities were noted. However, the rates of PCI history, catheterization indications, and applied preprocedural antiplatelet therapies were significantly different between the groups (Table 1).
Procedural information and outcome data. Procedural information and clinical outcomes are shown in Table 2. Arterial sheath sizes and PCI rates were significantly different between the groups. In PCIs, rotational atherectomy was used in 30.2% of patients and significantly more often in the TFA group compared to the TRA group (47.4% vs 16.7%, respectively; P=.03). In-hospital and 30-day mortality rates were both 0.0%. Puncture-site bleeding occurred in 1 patient (3.8%) from the TFA group and coil embolization was required for pseudoaneurysm closure. On the other hand, no puncture-site bleeding occurred in the TRA group (P=.12). In the TRA group, 1 patient (1.6%) had puncture-site hematoma, but no surgical procedure or transfusion was necessary. No other puncture-site related complications (such as AVF, neurological injury, collagen-plug embolization, or puncture-site infection) were observed in either group. Other complications are shown in Table 2.
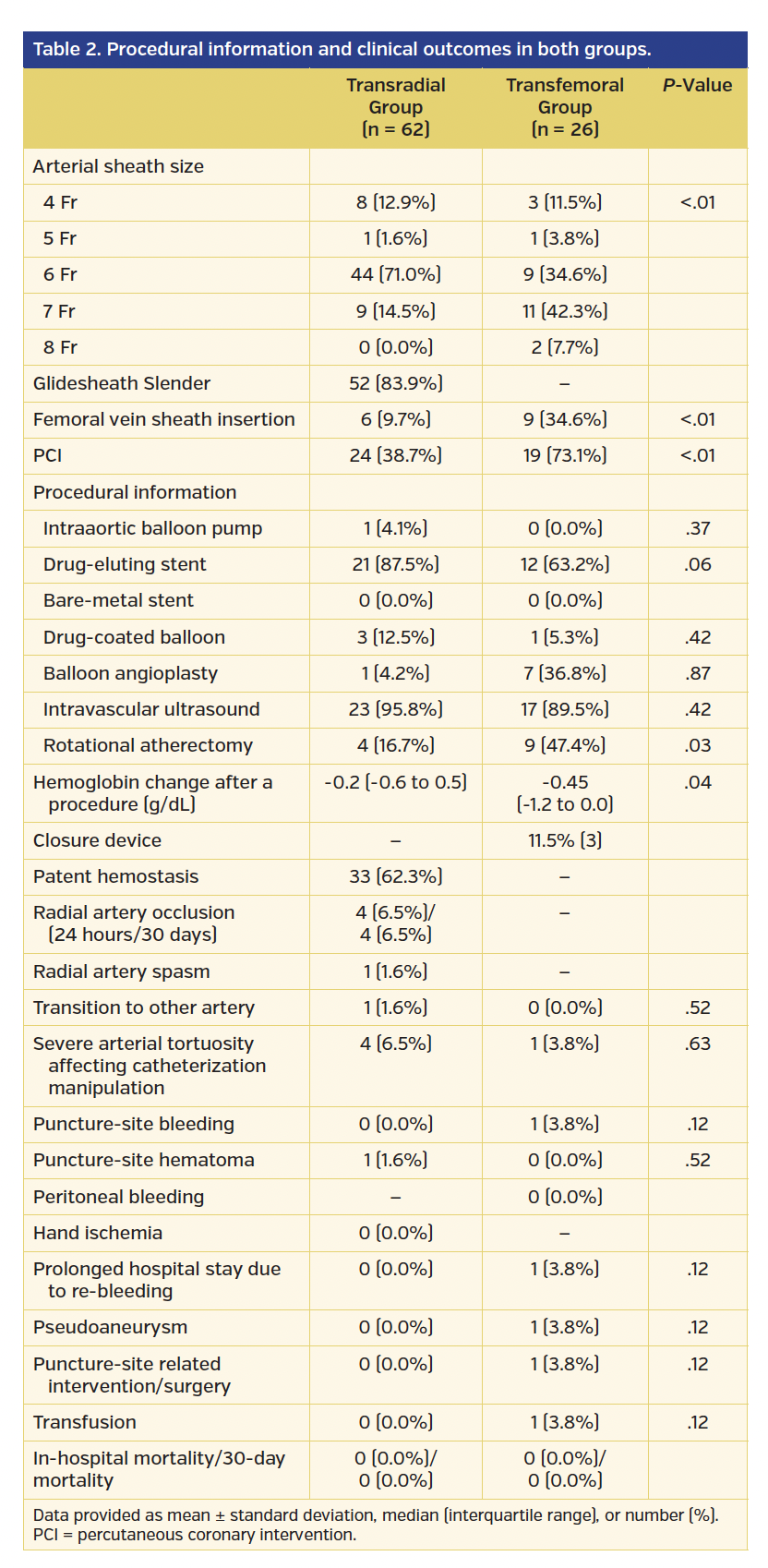
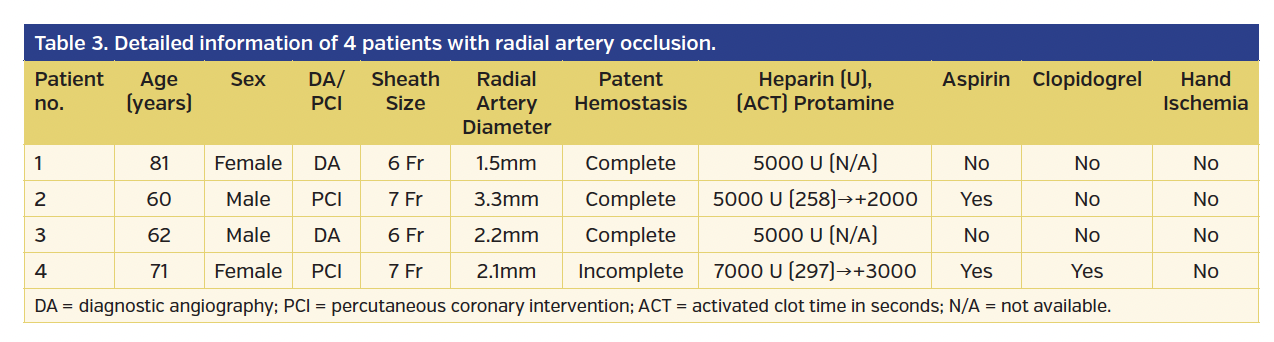
In the TRA group, mean radial artery diameter was 2.5 ± 0.5 mm and procedural success rate was 98.4%. One patient experienced radial artery spasm after sheath insertion and crossover to TFA was necessary. Patent hemostasis was achieved in 62.3% of patients and RAO occurred in 4 patients (6.5%). Of these, 2 patients underwent PCI with 7 Fr Glidesheath Slender and radial artery diameters were 2.1 mm and 3.3 mm. In the other 2 patients, 6 Fr Glidesheath Slender was inserted for DA and radial artery diameters were 1.5 mm and 2.2 mm. Patent hemostasis was achieved in 3 of these patients. None of the 4 patients had symptoms of RAO. Detailed information for all RAO patients is provided in Table 3.
Discussion
The main advantages of TRA are patient comfort and reduced rate of bleeding complications. Although this approach raised concerns about possible RAO and loss of future access site for AVF, we attempted TRA in patients on dialysis and constructed a system for TRA. Our study could lead to a prevalence of TRA in these patients, which would lead to better prognosis and increased patient comfort.
In the current practice, bleeding avoidance strategies are necessary, especially for patients with high bleeding risk. Previous studies have proven that TRA reduced bleeding complications and mortality rates,5,6,29 whereas the current American Heart Association statement includes a class III recommendation for the routine use of vascular closure devices to reduce the incidence of vascular complications.30 Importantly, a previous study reported that patients on dialysis have a high bleeding risk.31 However, operators hesitate to choose TRA because they wish to preserve the radial artery for a future AVF. This could lead to a very difficult adaptation of operators to TRA for these patients.7 In addition, access-point preservation for possible hemodialysis in the future is questionable because low 5-year survival rates of patients on dialysis were reported.15,16,32 Moreover, since recent angioplasties for AVF stenosis increased, we may increase AVF patency using a cutting balloon and other related devices, which could decrease the influence of RAO.33,34 Because no puncture-site bleeding occurred in the TRA group in our study, we considered TRA to be beneficial in reducing the incidences of bleeding complications and early mortality, regardless of RAO risk.
Attempting TRA in dialysis patients is challenging. The current consensus recommends access-site preservation for future AVF and to avoid TRA in these patients.35 Recently, Shouwen et al36 reviewed the advantages and disadvantages of TRA for patients on dialysis and noted the following: (1) using TRA for patients on dialysis or with chronic kidney disease stage 4 or 5 is not conventionally recommended; (2) however, the potential benefit of TRA should be evaluated on a case-by-case basis (such as a case with high bleeding risk or too-small forearm veins for future creation of AVF); (3) TRA should be considered only on the contralateral side of AVF; (4) the transbrachial approach may be associated with a higher risk than TRA; and (5) even when RAO occurs, the proximal radial artery can be used if it is patent.37 RAO rates were 1%-10% in previous studies.8-14 This variability can be attributed to these studies having different patient characteristics. The proportions of a large-sized sheath and patients with a small radial artery could affect the RAO rates.8 In our study, the rate of RAO was 6.5%, which was relatively high, but within the range of previous studies.8-14 Arterial intimal thickening in patients on dialysis may be suspected as RAO can be caused by arterial tears.38-40 Fortunately, we did not have symptomatic hand ischemia complications due to RAO in the present study; however, it is at high risk for patients on dialysis.41 To the best of our knowledge, there is a paucity of data in terms of RAO in patients on dialysis. Thus, showing the rate of RAO in these patients has great value. Further study is necessary to evaluate RAO for patients on dialysis, and the clinical benefit of TRA.
We considered that written informed consent that included a statement regarding the possibility of RAO and nephrologist approval was essential for this study to attempt TRA. Moreover, because TRA could improve patient comfort, but increase the risk of RAO and future AVF problems, patients needed to decide if TRA or TFA should be used.42 Furthermore, minimizing the risk of RAO is necessary.40 Although we used the Glidesheath Slender and tried to obtain the best possible patent hemostasis, patient still experienced RAO.13,24 We should make every effort to decrease RAO rates, such as prophylactic ulnar compression, while banding the radial artery or ulnar compression to recanalize RAO after band removal.12,43 The long compression time could be one of the reasons behind RAO in the current study,11 as we could not change conventional compression time due to the lack of experience with short-term compression and concern over compartment syndrome due to the high bleeding risk profile of these patients.31,44 Another reason for RAO occurrence could be the large size of the sheaths used.40 Sheath size was operator dependent and study protocol did not mandate smaller sheath sizes. The higher rate of rotational atherectomy use (30.2%) in patients on dialysis compared to other populations required larger sheath sizes.21
Study limitations. This study has several limitations. First, it was an observational clinical trial and not a randomized trial. The use of TRA depended on the operator’s decision. Therefore, we could not conclude the benefit of TRA. Second, the proportion of patients with acute coronary syndromes was small, and TRA has shown particular benefit in such patients.5,6 Moreover, we did not include patients with ST-elevation myocardial infarction in the TRA group, and obtaining written informed consent with a statement of possible RAO for emergency PCI might be challenging. Finally, we did not perform PCI with 5 Fr sheaths. Because patients on dialysis have more complicated lesions,45 at least 6 Fr sheaths were usually used for PCI. Sheathless guiding with 6.5 Fr devices (SheathLess; Asahi Intecc) would be another option because of smaller dimensions than conventional 5 Fr sheaths and lower the risk of RAO.40
Conclusion
Our data showed the feasibility of TRA for dialysis patients. Our study could lead to the use of more TRA in these patients, which would lead better prognosis and patient comfort. Further studies are necessary to investigate the RAO rate, bleeding complications, and mortality rate with TRA use in dialysis patients.
Acknowledgment. The authors thank the staff of the cardiology wards and catheterization laboratory at Japanese Red Cross Ashikaga Hospital.
References
1. Manoukian SV, Feit F, Mehran R, et al. Impact of major bleeding on 30-day mortality and clinical outcomes in patients with acute coronary syndromes: an analysis from the ACUITY trial. J Am Coll Cardiol. 2007;49:1362-1368.
2. Kwok CS, Khan MA, Rao SV, et al. Access and non-access site bleeding after percutaneous coronary intervention and risk of subsequent mortality and major adverse cardiovascular events: systematic review and meta-analysis. Circ Cardiovasc Interv. 2015;8(4).
3. Mamas MA, Anderson SG, Carr M, et al; for the British Cardiovascular Intervention Society and National Institute for Cardiovascular Outcomes Research. Baseline bleeding risk and arterial access site practice in relation to procedural outcomes after percutaneous coronary intervention. J Am Coll Cardiol. 2014;64:1554-1564.
4. Dauerman HL, Rao SV, Resnic FS, Applegate RJ. Bleeding avoidance strategies. Consensus and controversy. J Am Coll Cardiol. 2011;58:1-10.
5. Karrowni W, Vyas A, Giacomino B, et al. Radial versus femoral access for primary percutaneous interventions in ST-segment elevation myocardial infarction patients: a meta-analysis of randomized controlled trials. JACC Cardiovas Interv. 2013;6:814-823.
6. Bernat I, Horak D, Stasek J, et al. ST-segment elevation myocardial infarction treated by radial or femoral approach in a multicenter randomized clinical trial: the STEMI-RADIAL trial. J Am Coll Cardiol. 2014;63:964-972.
7. Wimmer NJ, Resnic FS, Mauri L, et al. Risk-treatment paradox in the selection of transradial access for percutaneous coronary intervention. J Am Heart Assoc. 2013;2:e000174.
8. Brancati MF, Burzotta F, Coluccia V, Trani C. The occurrence of radial artery occlusion following catheterization. Expert Rev Cardiovasc Ther. 2012;10:1287-1295.
9. Dharma S, Kedev S, Patel T, Kiemeneij F, Gilchrist IC. A novel approach to reduce radial artery occlusion after transradial catheterization: postprocedural/prehemostasis intra-arterial nitroglycerin. Catheter Cardiovasc Interv. 2015;85:818-825.
10. Al-Jaishi AA, Oliver MJ, Thomas SM, et al. Patency rates of the arteriovenous fistula for hemodialysis: a systematic review and meta-analysis. Am J Kidney Dis. 2014;63:464-478.
11. Pancholy SB, Patel TM. Effect of duration of hemostatic compression on radial artery occlusion after transradial access. Catheter Cardiovasc Interv. 2012;79:78-81.
12. Pancholy SB, Bernat I, Bertrand OF, Patel TM. Prevention of radial artery occlusion after transradial catheterization: the PROPHET-II randomized trial. JACC Cardiovas Interv. 2016;9:1992-1999.
13. Pancholy S, Coppola J, Patel T, Roke-Thomas M. Prevention of radial artery occlusion-patent hemostasis evaluation trial (PROPHET study): a randomized comparison of traditional versus patency documented hemostasis after transradial catheterization. Catheter Cardiovasc Interv. 2008;72:335-340.
14. Pancholy SB, Bertrand OF, Patel T. Comparison of a priori versus provisional heparin therapy on radial artery occlusion after transradial coronary angiography and patent hemostasis (from the PHARAOH study). Am J Cardiol. 2012;110:173-176.
15. Marui A, Kimura T, Nishiwaki N, et al; for the CREDO-Kyoto PCI/CABG Registry Cohort-2 Investigators. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with end-stage renal disease requiring dialysis (5-year outcomes of the CREDO-Kyoto PCI/CABG Registry Cohort-2). Am J Cardiol. 2014;114:555-561.
16. Biesenbach G, Hubmann R, Grafinger P, et al. 5-year overall survival rates of uremic type 1 and type 2 diabetic patients in comparison with age-matched nondiabetic patients with end-stage renal disease from a single dialysis center from 1991 to 1997. Diabetes Care. 2000;23:1860-1862.
17. Kolesnyk I, Dekker FW, Boeschoten EW, Krediet RT. Time-dependent reasons for peritoneal dialysis technique failure and mortality. Perit Dial Int. 2010;30:170-177.
18. Valgimigli M, Campo G, Penzo C, et al. Transradial coronary catheterization and intervention across the whole spectrum of Allen test results. J Am Coll Cardiol. 2014;63:1833-1841.
19. Roe MT, Messenger JC, Weintraub WS, et al. Treatments, trends, and outcomes of acute myocardial infarction and percutaneous coronary intervention. J Am Coll Cardiol. 2010;56:254-263.
20. Anderson HV, Shaw RE, Brindis RG, et al. Risk-adjusted mortality analysis of percutaneous coronary interventions by American College of Cardiology/American Heart Association guidelines recommendations. Am J Cardiol. 2007;99:189-196.
21. Numasawa Y, Kohsaka S, Ueda I, et al. Incidence and predictors of bleeding complications after percutaneous coronary intervention. J Cardiol. 2017;69:272-279.
22. Takeshita S, Asano H, Hata T, et al; for the NAUSICA Trial Investigators. Comparison of frequency of radial artery occlusion after 4Fr versus 6Fr transradial coronary intervention (from the Novel Angioplasty USIng Coronary Accessor Trial). Am J Cardiol. 2014;113:1986-1989.
23. Freixa X, Trilla M, Feldman M, et al. Right versus left transradial approach for coronary catheterization in octogenarian patients. Catheter Cardiovasc Interv. 2012;80:267-272.
24. Aminian A, Dolatabadi D, Lefebvre P, et al. Initial experience with the Glidesheath Slender for transradial coronary angiography and intervention: a feasibility study with prospective radial ultrasound follow-up. Catheter Cardiovasc Interv. 2014;84:436-442.
25. Abdelaal E, Brousseau-Provencher C, Montminy S, et al. Interventional Cardiologists at Quebec Heart-Lung I: Risk score, causes, and clinical impact of failure of transradial approach for percutaneous coronary interventions. JACC Cardiovasc Interv. 2013;6:1129-1137.
26. Vora AN, Peterson ED, McCoy LA, et al. Factors associated with initial prasugrel versus clopidogrel selection for patients with acute myocardial infarction undergoing percutaneous coronary intervention: insights from the treatment with ADP receptor inhibitors: longitudinal assessment of treatment patterns and events after acute coronary syndrome (TRANSLATE-ACS) study. J Am Heart Assoc. 2016;5(9).
27. Mehta SK, Frutkin AD, Lindsey JB, et al; National Cardiovascular Data Registry. Bleeding in patients undergoing percutaneous coronary intervention: the development of a clinical risk algorithm from the National Cardiovascular Data Registry. Circ Cardiovasc Interv. 2009;2:222-229.
28. Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation. 2011;123:2736-2747.
29. Rao SV, Ou FS, Wang TY, et al. Trends in the prevalence and outcomes of radial and femoral approaches to percutaneous coronary intervention: a report from the National Cardiovascular Data Registry. JACC Cardiovasc Interv. 2008;1:379-386.
30. Patel MR, Jneid H, Derdeyn CP, et al. Arteriotomy closure devices for cardiovascular procedures: a scientific statement from the American Heart Association. Circulation. 2010;122:1882-1893.
31. Numasawa Y, Kohsaka S, Miyata H, et al. Impact of body mass index on in-hospital complications in patients undergoing percutaneous coronary intervention in a Japanese real-world multicenter registry. PLoS One. 2015;10:e0124399.
32. Patel AD, Ibrahim M, Swaminathan RV, et al. Five-year mortality outcomes in patients with chronic kidney disease undergoing percutaneous coronary intervention. Catheter Cardiovasc Interv. 2017;89:E124-E132. Epub 2016 Aug 13.
33. Beathard GA, Urbanes A, Litchfield T. Changes in the profile of endovascular procedures performed in freestanding dialysis access centers over 15 years. Clin J Am Soc Nephrol. 2017;12:779-786.
34. Khawaja AZ, Cassidy DB, Al Shakarchi J, et al. Systematic review of drug eluting balloon angioplasty for arteriovenous haemodialysis access stenosis. J Vasc Access. 2016;17:103-110.
35. Natsuaki M, Morimoto T, Furukawa Y, et al. Comparison of 3-year clinical outcomes after transradial versus transfemoral percutaneous coronary intervention. Cardiovasc Interv Ther. 2012;27:84-92.
36. Wang S, Asif A. Transradial approach for cardiovascular interventions and its implications for hemodialysis vascular access. Semin Dial. 2013;26:E20-E29.
37. Wu CC, Jiang H, Cheng J, et al. The outcome of the proximal radial artery arteriovenous fistula. J Vasc Surg. 2015;61:802-808.
38. Buyukhatipoglu H, Tiryaki O, Tahta K, Usalan C. Inflammation as a risk factor for carotid intimal-medial thickening, a measure of subclinical atherosclerosis in haemodialysis patients: the role of chlamydia and cytomegalovirus infection. Nephrology. 2007;12:25-32.
39. Chin CY, Matsumura M, Maehara A, et al. Coronary plaque characteristics in hemodialysis-dependent patients as assessed by optical coherence tomography. Am J Cardiol. 2017;119:1313-1319.
40. Mamas MA, Fraser DG, Ratib K, et al. Minimising radial injury: prevention is better than cure. EuroIntervention. 2014;10:824-832.
41. Itaya H, Nakamura M. Novel strategy for percutaneous transluminal angioplasty for complex critical hand. Cardiovasc Interv Ther. 2012;27:52-56.
42. Cooper CJ, El-Shiekh RA, Cohen DJ, et al. Effect of transradial access on quality of life and cost of cardiac catheterization: a randomized comparison. Am Heart J. 1999;138:430-436.
43. Bernat I, Bertrand OF, Rokyta R, et al. Efficacy and safety of transient ulnar artery compression to recanalize acute radial artery occlusion after transradial catheterization. Am J Cardiol. 2011;107:1698-1701.
44. Rao SV, Bernat I, Bertrand OF. Clinical update: remaining challenges and opportunities for improvement in percutaneous transradial coronary procedures. Eur Heart J. 2012;33:2521-2526.
45. Aoyama T, Ishii H, Toriyama T, et al. Sirolimus-eluting stents vs bare metal stents for coronary intervention in Japanese patients with renal failure on hemodialysis. Circ J. 2008;72:56-60.
From the 1Department of Cardiology; and 2Department of Nephrology, Japanese Red Cross Ashikaga Hospital, Ashikaga, Japan.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted June 12, 2017, provisional acceptance given July 12, 2017, final version accepted October 19, 2017.
Address for correspondence: Toshiki Kuno, MD, PhD, Department of Cardiology, Japanese Red Cross Ashikaga Hospital, 284-1 Yobe-cho, Ashikaga, Japan. Email: kuno-toshiki@hotmail.co.jp










