Body Mass Index and Chronic Total Occlusion Percutaneous Coronary Intervention Outcomes: Is Overweight the New Normal?
Abstract
Background. Although high body mass index (BMI) is a known risk factor for the development of cardiovascular diseases, people who are overweight or obese often have better outcomes after cardiac procedures. Whether this "obesity paradox" is observed in chronic total occlusion (CTO) percutaneous coronary intervention (PCI) is unknown. Therefore, we examined the association of BMI with the outcomes of CTO-PCI in patients from the large, multicenter PROGRESS-CTO registry after stratifying patients into 3 BMI groups.
J INVASIVE CARDIOL 2023;35(3):E126-E127. Epub 2023 January 13.
Key words: BMI, chronic total occlusion, clinical outcomes, percutaneous coronary intervention
While high body mass index (BMI) is a known risk factor for the development of cardiovascular disease, people who are overweight or obese often have better outcomes after cardiac procedures (the obesity paradox).1 A large analysis from the British Cardiovascular Intervention Society registry reported that overweight or obese patients had significantly lower mortality post percutaneous coronary intervention (PCI) for acute coronary syndrome.2 An analysis of the Midwest STEMI Consortium demonstrated that overweight and obese patients had significantly lower 1-year mortality.3
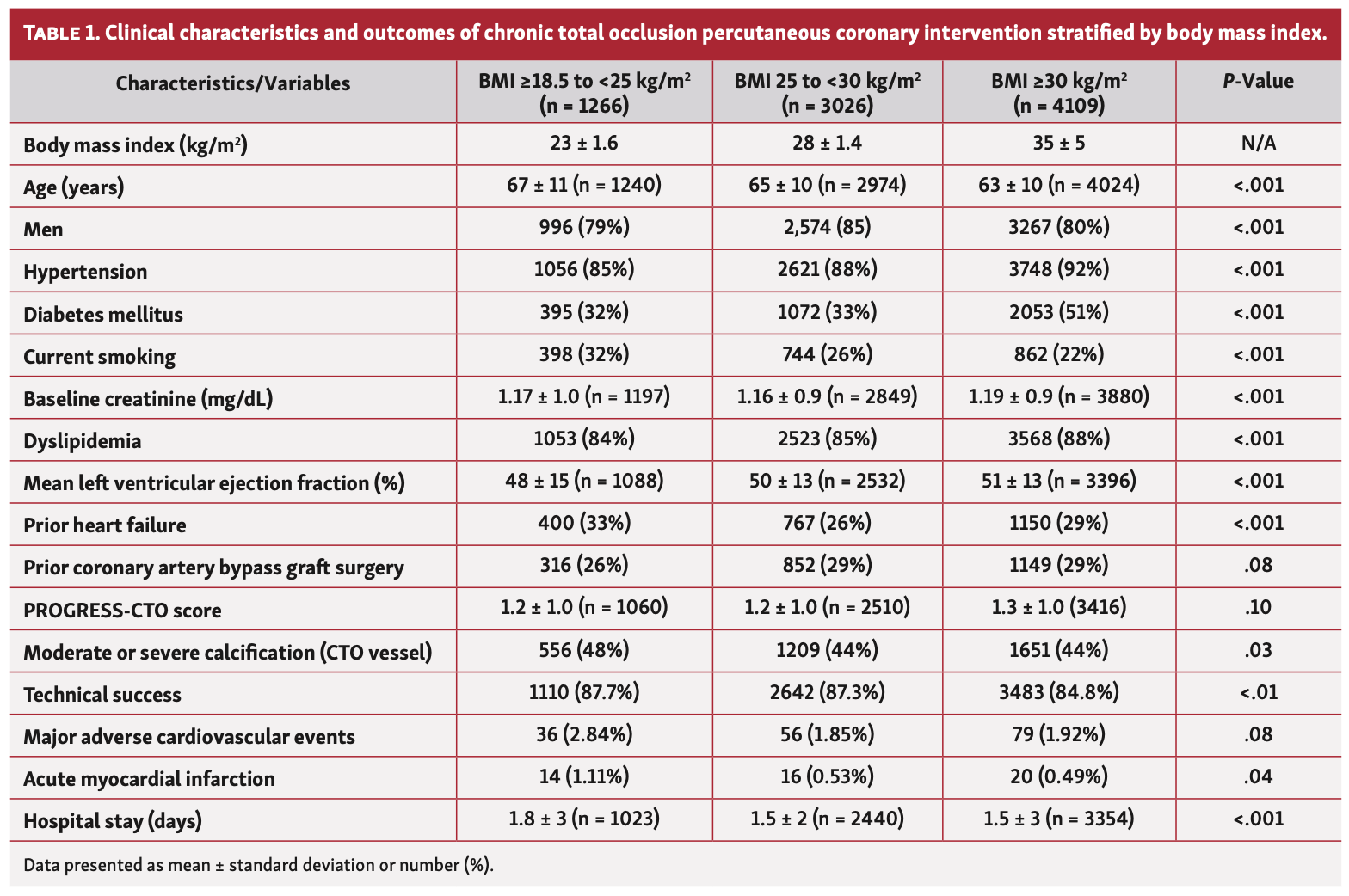
Whether this phenomenon is observed in chronic total occlusion (CTO)-PCI is unknown. Therefore, we examined the association of BMI with the outcomes of CTO-PCI in the large, multicenter PROGRESS-CTO (Prospective Global Registry for the Study of Chronic Total Occlusion Intervention) registry (NCT02061436) after stratifying patients into 3 BMI groups: normal, 18.5 to <25 kg/m2; overweight, ≤25 to <30 kg/m2; and obese, ≥30 kg/m2). In-hospital major adverse cardiovascular event (MACE) was defined as the composite of all-cause death, acute myocardial infarction, re-PCI, stroke, pericardiocentesis, and emergency surgery.
Of 8401 patients who underwent CTO-PCI at 36 centers between 2012-2022, a total of 1266 (15%) had normal BMI, 3026 (36%) were overweight, and 4109 (49%) were obese. Overweight and obese patients had higher left ventricular ejection fraction compared with patients with normal BMI, were less likely to have a history of heart failure, and had less calcification in the CTO vessel (Table 1). Technical success was lowest in obese patients compared with overweight and normal BMI patients (84.8% vs 87.7% vs 87.3%, respectively; P<.01), whereas the incidence of MACE was numerically highest in the normal BMI group (2.84% vs 1.85% vs 1.92%; P=.08). The length of hospital stay was shorter in the overweight and obese group combined compared with the normal BMI group (1.5 ± 3 days vs 1.8 ± 3 days; P<.002).
The average BMI in the United States is ~30 kg/m2; hence, individuals with normal BMI might have loss of lean mass (muscle mass or fat-free mass) without necessarily having less body fat, which could be related to worse outcomes in this group (the lean paradox).1
In conclusion, overweight patients had similar CTO-PCI technical success (87.7% vs 87.3%; P=.74) and significantly lower MACE (2.84% vs 1.85%; P=.04) compared with patients who had normal BMI, but had higher technical success (87.3% vs 84.8%; P<.01) and similar MACE (1.85% vs 1.92%; P=.82) compared with obese patients. After adjusting for potential confounders, the association between higher BMI and lower technical success remained statistically significant (P<.01), but higher BMI was no longer associated with lower MACE (P=.29).
Affiliations and Disclosures
From the 1Minneapolis Heart Institute and Minneapolis Heart Institute Foundation, Minneapolis, Minnesota; 2Division of Cardiology, Henry Ford Hospital, Detroit, Michigan; 3Department of Cardiology, WellSpan Health, York, Pennsylvania; 4Cardiovascular Research Center and Cardiology Division, Harvard Medical School and Massachusetts General Hospital, Boston, Massachusetts; 5Division of Cardiology, VCU Health Pauley Heart Center, Virginia Commonwealth University, Richmond, Virginia; and 6Cleveland Clinic Foundation, Cleveland, Ohio.
Funding: The authors are grateful for the philanthropic support of our generous anonymous donors, and the philanthropic support of Drs Mary Ann and Donald A Sens; Mrs Diane and Dr Cline Hickok; Mrs Wilma and Mr Dale Johnson; Mrs Charlotte and Mr Jerry Golinvaux Family Fund; the Roehl Family Foundation; the Joseph Durda Foundation. The generous gifts of these donors to the Minneapolis Heart Institute Foundation’s Science Center for Coronary Artery Disease (CCAD) helped support this research project.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Alaswad reports consulting and speaker honoraria from Boston Scientific, Cardiovascular Systems, Inc, Abbott Vascular, Teleflex. Dr Davies reports honoraria/consulting from Medtronic, Siemens Healthineers, Asahi intec. Dr Jaffer reports sponsored research from Canon, Siemens, Shockwave, Teleflex, Mercator, Boston Scientific; consultant for Boston Scientific, Siemens, Magenta Medical, IMDS, Asahi Intecc, Biotronik, Philips, Intravascular Imaging; equity interest in Intravascular Imaging, Inc, DurVena; licensing arrangements with his institution from Terumo, Canon, Spectrawave, for which he has the right to receive royalties. Dr Doshi reports speaker’s bureau income from Abbott Vascular, Boston Scientific, and Medtronic; research support from Biotronik. Dr Azzalini reports honoraria from Abbott Vascular, Guerbet, Terumo, and Sahajanand Medical Technologies; research support from ACIST Medical Systems, Guerbet, Terumo. Dr Khatri reports speaking fees from Medtronic, Abbott, Boston, Terumo, Asahi Intecc. Dr Brilakis reports consulting/speaker honoraria from Abbott Vascular, American Heart Association (associate editor, Circulation), Amgen, Asahi Intecc, Biotronik, Boston Scientific, Cardiovascular Innovations Foundation (Board of Directors), ControlRad, CSI, Elsevier, GE Healthcare, IMDS, InfraRedx, Medicure, Medtronic, Opsens, Siemens, Teleflex; research support from Boston Scientific, GE Healthcare; owner, Hippocrates LLC; shareholder, MHI Ventures, Cleerly Health, Stallion Medical. The remaining authors report no disclosures regarding the content herein.
Manuscript accepted June 1, 2022.
Address for correspondence: Emmanouil S. Brilakis, MD, PhD, Director of the Center for Complex Coronary Interventions, Minneapolis Heart Institute, Chairman of the Center for Coronary Artery Disease at the Minneapolis Heart Institute Foundation, 920 East 28th Street #300, Minneapolis, MN 55407. Email: esbrilakis@gmail.com
References
1. Elagizi A, Kachur S, Lavie CJ, et al. An overview and update on obesity and the obesity paradox in cardiovascular diseases. Prog Cardiovasc Dis. 2018;61(2):142-150. Epub 2018 Jul 5. doi:10.1016/j.pcad.2018.07.003
2. Holroyd EW, Sirker A, Kwok CS, et al. The relationship of body mass index to percutaneous coronary intervention outcomes: does the obesity paradox exist in contemporary percutaneous coronary intervention cohorts? Insights from the British Cardiovascular Intervention Society Registry. JACC Cardiovasc Interv. 2017;10(13):1283-1292. doi:10.1016/j.jcin.2017.03.013
3. Mattingly G, Yildiz M, Lantz R, et al. Abstract 13916: the obesity paradox in ST-elevation myocardial infarction. Circulation. 2021;144:A13916-A13916.