Right Internal Jugular Implantation of the AVEIR Leadless Pacemaker: A Case Series Demonstrating Feasibility and Safety
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Objectives. Leadless pacemakers provide an alternative to transvenous pacing in patients at risk for lead- and pocket-related complications. While the femoral vein is the standard route of implantation, certain anatomical or clinical factors may make this approach technically challenging. The objective of this study was to evaluate the feasibility and safety of AVEIR (Abbott) implantation through the right internal jugular (RIJ) vein in patients in whom the femoral approach was not feasible.
Methods. The authors report a single-center case series of patients who underwent AVEIR implantation using the RIJ vein. Procedural techniques, periprocedural management, and early clinical outcomes were reviewed.
Results. Eight patients (8 VR and 1 DR) underwent successful implantation through the RIJ approach. Device deployment was accomplished with stable electrical parameters and without acute complications.
Conclusions. This case series demonstrates that AVEIR implantation via the RIJ is both technically feasible and safe. These findings expand access strategies for leadless pacing and may provide a foundation for future applications of conduction system pacing using superior venous routes.
Introduction
Leadless pacemakers have emerged as an important alternative to traditional transvenous pacing systems, particularly in patients at increased risk for lead- or pocket-related complications.1 Current systems, including the AVEIR, are delivered through a transfemoral approach. In many patients this route is straightforward and effective, but in others, the presence of anatomical barriers such as an inferior vena cava (IVC) filter or severe IVC tortuosity precludes safe passage of the large-bore delivery sheath.
In such cases, alternative venous routes must be considered. The right internal jugular (RIJ) vein offers a direct trajectory to the right atrium and ventricle and has been used in select circumstances for the delivery of leadless devices, particularly the Micra system (Medtronic). Prior reports describe RIJ implantation of Micra particularly in patients with IVC filters, chronic IVC occlusion, marked venous tortuosity, and congenital anomalies such as interrupted IVC with azygous continuation.1,2 Sporadic reports of AVEIR implantation via the RIJ in the adult population have also been described,3,4 but systematic experience remains limited.
We describe a case series of patients who underwent AVEIR implantation via the RIJ approach after the femoral route was deemed unfeasible. We focus on technical considerations, periprocedural outcomes, and the implications for future applications of superior venous access in leadless pacing.
Methods
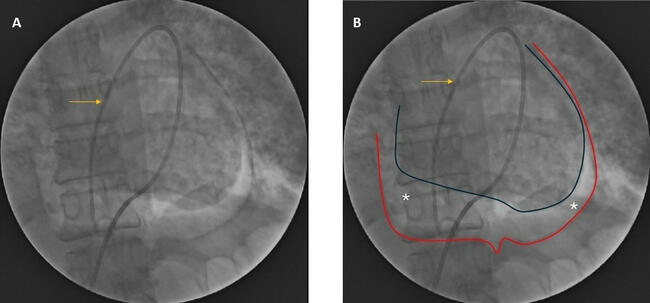
This single-center, retrospective case series included patients who underwent AVEIR implantation via the RIJ vein between 2023 and 2025. The RIJ approach was selected when the femoral route was not feasible because of venous tortuosity, the presence of IVC filter, or difficult venous anatomy that prevented safe advancement of the delivery system (Figure 1).
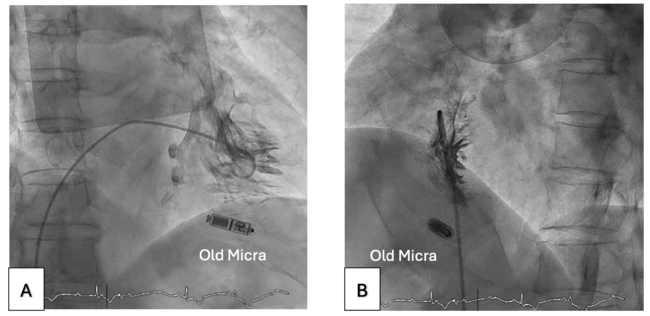
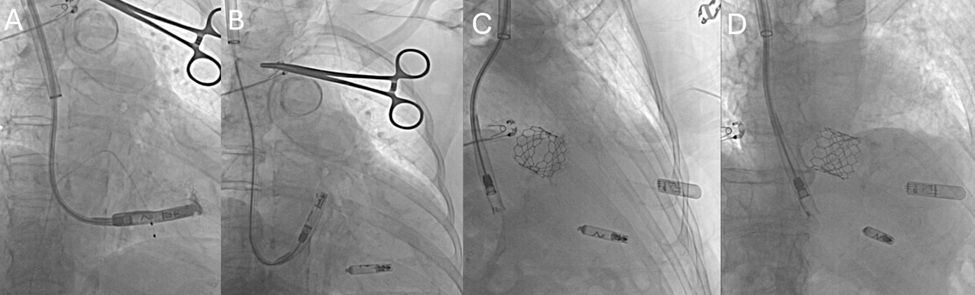
All procedures were performed under fluoroscopic guidance. Venous access was obtained in the RIJ vein under ultrasound guidance. A single Perclose ProGlide suture (Abbott) was deployed and secured with hemostats using the preclose technique. Serial dilatation allowed placement of the AVEIR delivery sheath. In cases of AVEIR VR, the sheath was advanced into the right atrium and carefully manipulated across the tricuspid valve into the right ventricle. Device deployment was performed at the right ventricular septum, and stability was confirmed with the standard tug test. Electrical performance was assessed by measuring sensing and capture thresholds, and final device release occurred only after implant criteria were satisfied (Figure 2). The delivery sheath was subsequently removed, and hemostasis was achieved with ProGlide closure in all patients.
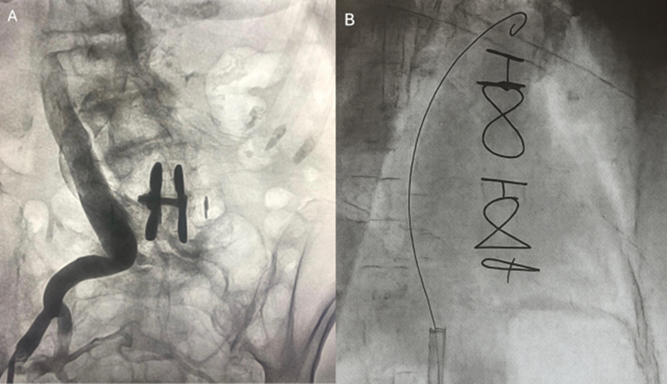
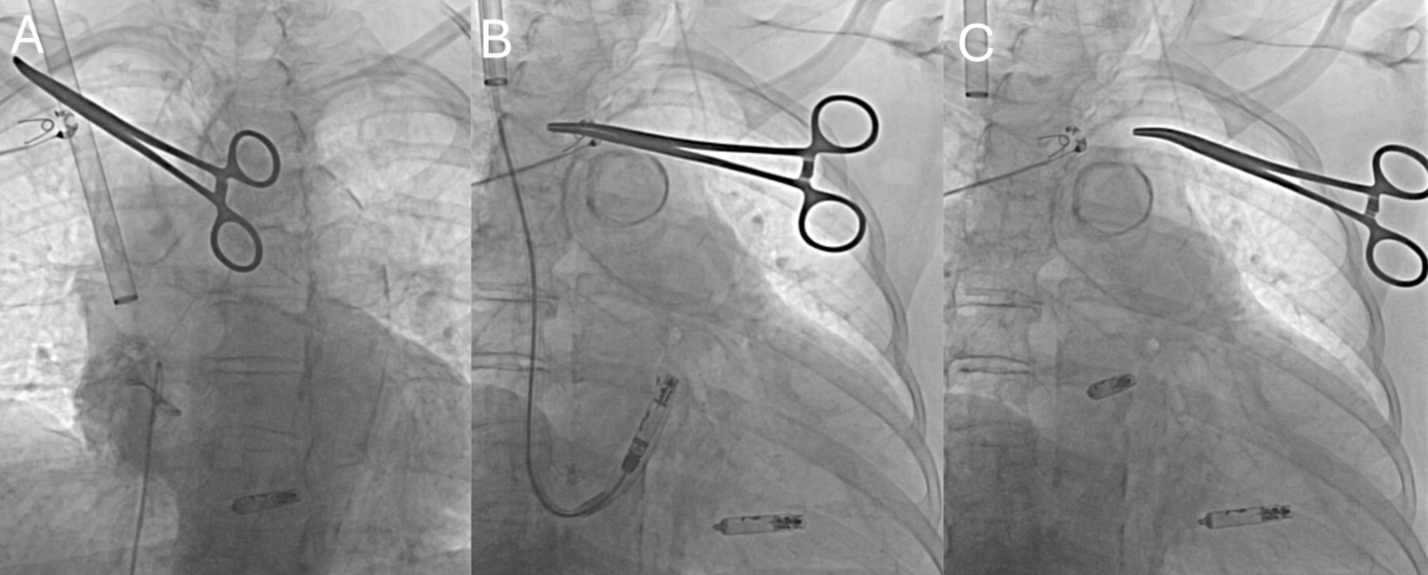
In cases of AVEIR AR, following successful placement of the VR device, an AVEIR AR was implanted via the same RIJ approach. The delivery sheath was advanced into the right atrium, and the delivery system was flexed to engage the base of the right atrial (RA) appendage. Contrast injection was used to confirm appendage depth and orientation. With fine adjustments in deflection and torque, the sheath was aligned toward the anterolateral RA wall at the appendage base, permitting secure fixation of the device. Deployment and electrical interrogation were performed using standard criteria (Figure 3).
Device interrogation was performed prior to discharge, and all patients returned at 2 weeks for skin incision assessment and repeat device interrogation.
Results
A total of 8 patients underwent AVEIR implantation via the RIJ approach during the study period. All procedures were completed successfully. The most common reason for selecting the RIJ was the presence of venous tortuosity, which prevented safe passage of the femoral delivery system.
Baseline clinical characteristics, pacing indication, anticoagulation status, procedural outcomes, pacing thresholds, sensing parameters, and complications were collected. A summary of these findings is presented in the Table.
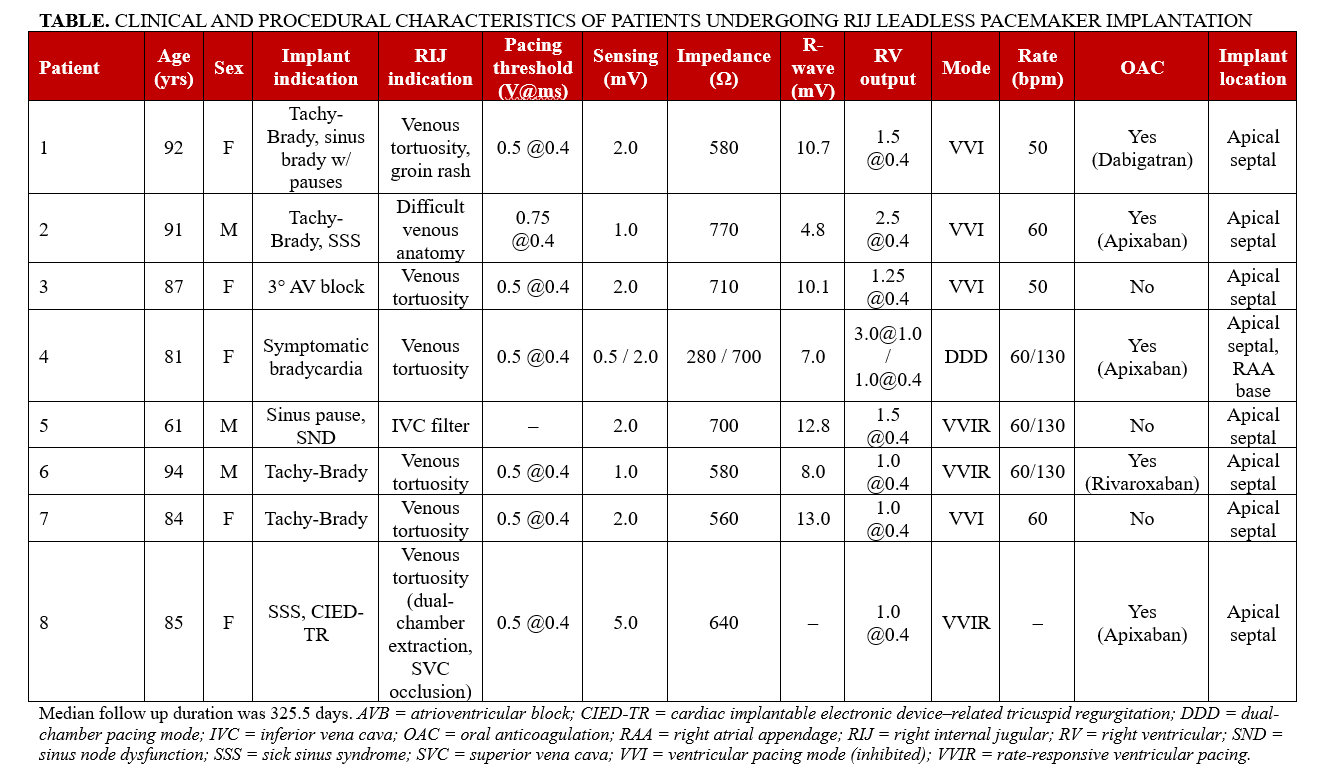
Implantation was accomplished in all patients with acceptable acute capture thresholds, sensing and impedance parameters, and the devices remained stable throughout the procedure. There were no procedural complications, including vascular injury, device dislodgement, or pericardial effusion. Patients tolerated the procedure well, and 1 ProGlide suture of the RIJ site was sufficient to achieve hemostasis in each case. At follow-up, device function remained stable, and no adverse events related to the access site were identified.
Discussion
This case series demonstrates the technical feasibility and safety of AVEIR implantation via the RIJ approach in patients where femoral venous access was not easily feasible. To our knowledge, this represents the first report of systematic experience with the AVEIR platform delivered through the RIJ vein.
The concept of using the RIJ for leadless pacemaker implantation is not new. Several groups have described successful delivery of the Micra device using the RIJ, with indications including IVC obstruction, IVC filters, venous tortuosity, congenital IVC anomalies, and altered surgical anatomy after surgery.1,2 Sporadic reports of AVEIR via RIJ have also been published.3,4 These reports established proof of principle that the superior venous route can be used effectively for leadless pacing systems. However, the AVEIR system differs significantly from Micra in terms of its delivery sheath size, flexibility, and deployment mechanics. Demonstrating the feasibility of AVEIR via the RIJ therefore provides clinically relevant evidence that this approach can be safely applied to newer leadless platforms.
The RIJ route provides a direct course into the right atrium and ventricle but requires careful manipulation of the relatively stiff delivery sheath across the tricuspid valve. Because the jugular entry offers only a short intrathoracic working distance, sheath stability is more precarious than with femoral access; in our experience, meticulous attention was required during manipulation to prevent inadvertent loss of sheath position.
The fluoroscopic angles used with the femoral approach must be adjusted by operators to ensure proper septal positioning for the RIJ route. Our experience suggests that, with attention to these technical details, implantation can be achieved reliably. Importantly, hemostasis at the jugular access site was readily achieved with a vascular closure device.
In addition, Soejima et al highlighted that the jugular trajectory may be particularly advantageous in patients with smaller cardiac dimensions, as the shorter and more direct route can facilitate sheath manipulation and device positioning compared with the femoral approach.5 This observation may be especially relevant in certain patient populations with smaller atrial and ventricular sizes.
In prior reports, the decision to pursue RIJ access for leadless pacemaker implantation was largely driven by limitations of the femoral route. Documented barriers have included IVC obstruction or occlusion, the presence of IVC filters, severe venous tortuosity, congenital IVC anomalies such as azygos continuation, and altered anatomy after prior tricuspid valve surgery. In these situations, the jugular approach provided a practical alternative that allowed safe advancement of the delivery system. However, Molitor et al recently demonstrated that the jugular route may also be chosen electively for Micra leadless pacemakers, even when femoral access is technically possible, highlighting operator preference and procedural strategy as additional considerations.1 More recently, smaller patient size and reduced cardiac chamber dimensions have also been cited as circumstances in which the superior venous route may facilitate device manipulation and positioning.5
Beyond these anatomic or surgical challenges, however, the RIJ approach may hold future significance as leadless pacing expands into dual-chamber and conduction system pacing strategies. Superior venous access may provide more favorable trajectories for engagement of atrial and His-Purkinje structures, and our early experience lays the groundwork for exploring these avenues. An additional potential advantage of the jugular approach is immediate ambulation of the patient, reducing pain and avoiding deep venous thrombosis.
Limitations
This study is limited by its small sample size and retrospective design. All procedures were performed at a single center by operators experienced with leadless device implantation, which may limit generalizability. Furthermore, only a single case involved implantation of a dual-chamber AVEIR DR system. Longer term follow-up and larger, multicenter series will be required to confirm the reproducibility and durability of this approach.
Conclusions
The RIJ approach for AVEIR leadless pacemaker implantation is technically feasible and safe in patients for whom the femoral route is technically challenging. These findings expand available access strategies for leadless pacing and support the potential use of superior venous approaches in the future development of conduction system pacing.
Affiliations and Disclosures
Leili Pourafkari, MD1,2; Jeong Hwan J. Kim, MD1; Ali Sovari, MD1,3
From the 1Department of Cardiovascular Disease, Los Robles Regional Medical Center, Thousand Oaks, California; 2Department of Anesthesiology, Jacobs School of Medicine and Biomedical Sciences, Buffalo, New York; 3Department of Cardiology, St. John’s Regional Medical Center, Oxnard, California.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for intervention described in the manuscript and to the publication of their data, including all images.
Address for correspondence: Ali Sovari, MD, Department of Cardiology, St. John’s Regional Medical Center, 1600 N Rose Ave, Oxnard, CA 93030, USA. Email: alisovari@gmail.com
References
- Molitor N, Saleem-Talib S, Ramanna H, Hofer D, Breitenstein A, Steffel J. Leadless pacemaker implantation via the internal jugular vein. Europace. 2024;26(8):euae199. doi:10.1093/europace/euae199
- Saleem-Talib S, van Driel VJ, Chaldoupi SM, et al. Leadless pacing: going for the jugular. Pacing Clin Electrophysiol. 2019;42(4):395-399. doi:10.1111/pace.13607
- Lewandowski M, Boczar K, Orzech DB, et al. First AVEIR VR leadless pacemaker implantations in Poland via internal jugular vein access. Kardiol Pol. 2025;83(6):772-774. doi:10.33963/v.phj.105223
- Suresh SP, Buchanan EB, Yoo D. First reports of dual-chamber leadless pacemaker implantation via intrajugular access. J Cardiovasc Electrophysiol. 2025;36(4):895-899. doi:10.1111/jce.16572
- Soejima K, Hilpisch K, Samec ML, Temple RL, Bonner MD. Jugular approach for the transcatheter pacemaker implant — better access for smaller hearts? Circ J. 2024;88(7):1127-1134. doi:10.1253/circj.CJ-24-0083