

Hot-Snare Assisted Percutaneous Mechanical Aspiration of a Calcified Amorphous Tumor
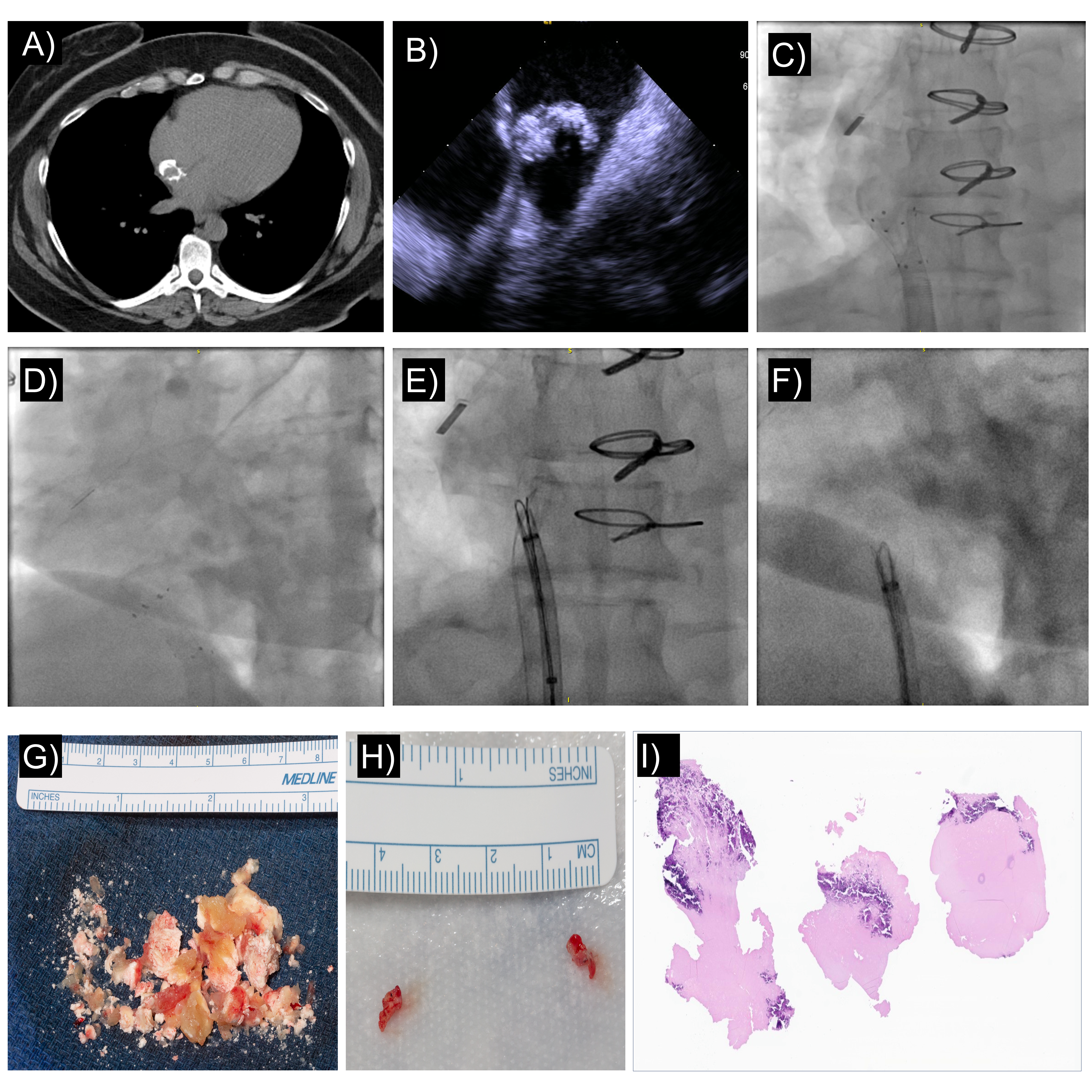
A 24-year-old female with history of an atrial septal defect post-patch closure (bovine pericardium) presented 4 years postoperative with an incidentally identified mass originating from the septal patch (Figure, A). Magnetic resonance imaging demonstrated an avascular structure with extrinsic calcification. A trial of anticoagulation was performed with no reduction in mass size, leading to a referral for endovascular removal.
Intracardiac echocardiography (ICE) from a right internal jugular approach was performed to visualize the mass (Figure, B). AngioVac (AngioDynamics) removal was performed utilizing a 22-French (F) inflow catheter and 19-F venous return. Heparin was administered to maintain an activated clotting time greater than 300 seconds. Flow was escalated to 4 L/minute with capture of the mass in the inflow funnel. Intermittent clamping of the circuit was performed to optimize suction effect and achieve aspiration of most of the mass (Figure, C & D). A residual stalk of tissue arising from the inferior-posterior septal patch was present, and the AngioVac system was unable to aspirate it. Manual retraction of the tissue using an 8-F EN Snare (18-30 mm; Merit Medical) was performed and unsuccessful, as it was firmly adhered to the patch.
A radiofrequency snare technique (polypectomy snare) was advanced over the shaft of the EN Snare around the base of the stalk of the tissue and tightened. Fifty watts were applied with slow retraction of the radiofrequency snare to detach the tissue from the atrial septum (Figure, E & F). The material was removed with the EN Snare. ICE demonstrated no residual tissue in the right atrium or iatrogenic atrial level shunt. Gross evaluation demonstrated calcified fibrotic tissue (Figure, G & H). Histopathology demonstrated organized thrombus with calcification consistent with calcified amorphous tumor (Figure I; Video).
This case outlines a novel treatment approach for endovascular intracardiac tumor removal and the utility of intracardiac echocardiography to guide the procedure in the right heart structures.
Affiliations and Disclosures
From the Department of Cardiovascular Medicine, Mayo Clinic, Rochester, Minnesota, USA.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address of correspondence: Jason H. Anderson, MD, 200 1st St SW, Rochester, MN 55905, USA. Email: anderson.jason@mayo.edu; X: @Dr_JHAnderson













