

Intracardiac Echocardiography-Guided Leaflet Modification for Coronary Protection Prior to Transcatheter Valve-in-Valve Replacement
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Transcatheter electrosurgery offers a safe and effective way to prevent iatrogenic coronary obstruction during transcatheter aortic valve replacement (TAVR) valve-in-valve (ViV).1 Tissue traversal and leaflet laceration require the complement of fluoroscopy and echocardiography for leaflet identification (left vs right coronary cusp) and optimal puncture location (mid, base).2 Transesophageal echocardiography (TEE) requires general anesthesia and visualization, particularly of the anteriorly located right coronary cusp (RCC), and is often hindered by acoustic shadowing from the prosthesis. Intracardiac echocardiography (ICE) provides a minimally invasive alternative that addresses these limitations.3
A 79-year-old man with a failed 25-mm CE Magna Ease 3300 surgical prosthesis (Edwards Lifesciences) and of high re-operative surgical risk (STS 8%) presented with dyspnea, NYHA III. Cardiac computed tomography angiography revealed anatomy that was at high risk for coronary occlusion with a short right coronary artery height of 6 mm and a valve-to-coronary distance of 2 mm. The decision was made for balloon-assisted BASILICA (bioprosthetic or native aortic scallop intentional laceration to prevent iatrogenic coronary artery obstruction during TAVR) and TAVR ViV using a 29-mm Evolut FX (Medtronic) under fluoroscopic and ICE guidance (Figure).
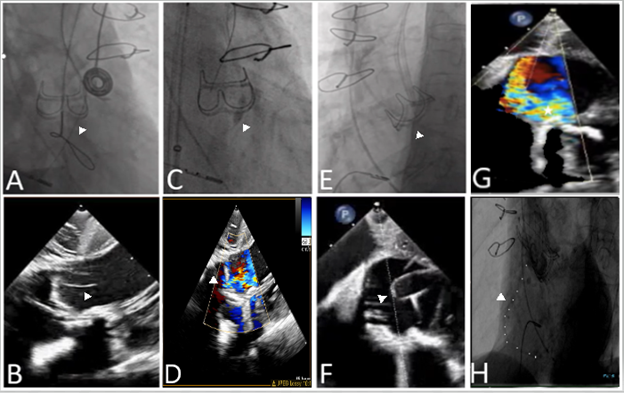
A 9-French VeriSight 3D ICE catheter (Phillips) was placed into the right atrium and a short axis view of the aortic valve was obtained. Three-dimensional ICE with x-plane and digital steering was able to identify the RCC, the ideal location for wire traversal (Figure A and B), and to visualize balloon dilatation (Figure C and D) and leaflet laceration (Figure E and F). Color Doppler revealed eccentric valvular aortic insufficiency through the right coronary leaflet (Figure G) and aortic root angiography confirmed patency of the RCA after TAVR (Figure H).
ICE is an effective alternative to TEE for TAVR ViV with BASILICA where localization for leaflet modification is essential.
Affiliations and Disclosures
From the Cardiovascular Institute, Lenox Hill Hospital, Northwell, New Hyde Park, New York, USA.
Consent statement: The authors affirm that informed consent was obtained for the described procedures.
Disclosures: Dr Kliger is a consultant and receives speaking honoraria from Edwards Lifesciences, Medtronic, and Siemens. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Chad Kliger, MD, Department of Cardiovascular and Thoracic Surgery, Lenox Hill Hospital/Northwell Health, 130 East 77th Street, 4th floor, New York, NY 10075, USA. Email: ckliger@northwell.edu
References
1. Khan JM, Rogers T, Greenbaum AB, et al. Transcatheter electrosurgery: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(12):1455-1470. doi: 10.1016/j.jacc.2020.01.035
2. Lederman RJ, Babaliaros VC, Rogers T, et al. Preventing coronary obstruction during transcatheter aortic valve replacement: from computed tomography to BASILICA. JACC Cardiovasc Interv. 2019;12(13):1197-1216. doi: 10.1016/j.jcin.2019.04.052
3. Alkhouli M, Hijazi ZM, Holmes DR Jr, Rihal CS, Wiegers SE. Intracardiac echocardiography in structural heart disease interventions. JACC Cardiovasc Interv. 2018;11(21):2133-2147. doi: 10.1016/j.jcin.2018.06.056









