

Mitral Transcatheter-Edge‐to‐Edge Repair in Failed Mitral Valve Repair
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
A 63-year-old man underwent mitral valve (MV) repair with a 28-mm Cosgrove-Edwards annuloplasty ring (Edwards Lifesciences) in 1999 due to severe primary mitral regurgitation (MR). He did well until recently, when he was recurrently admitted with pulmonary edema.
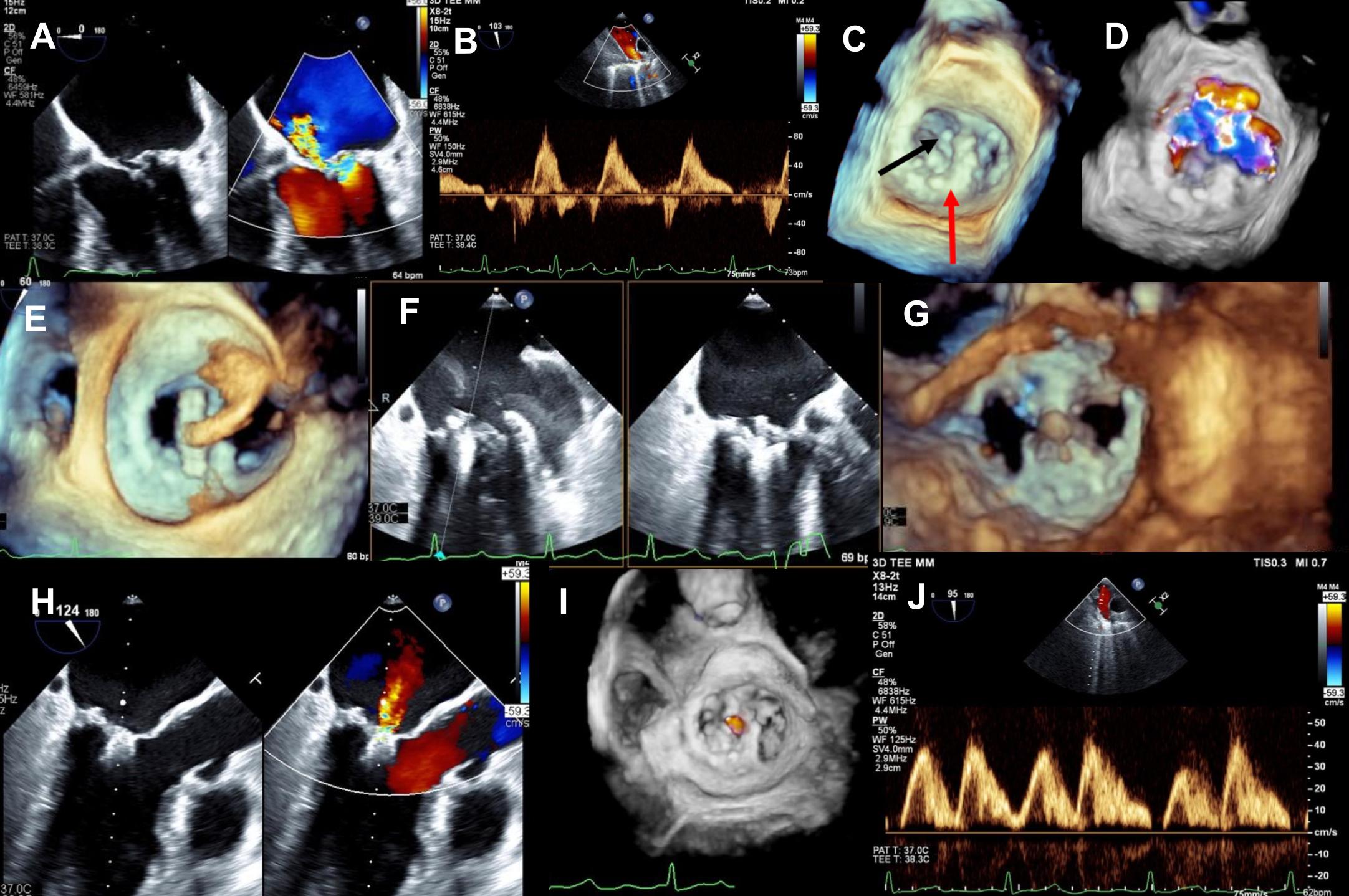
A transthoracic echocardiogram (TTE) revealed moderately reduced left ventricular systolic function and severe eccentric MR with a mean gradient of 3 mm Hg. Further evaluation using transesophageal echocardiography (TOE) demonstrated posterior leaflet flail with severe anteromedially directed MR (Figure A, Video 1) and systolic flow reversal in the pulmonary veins (Figure B). Three-dimensional views revealed the ring attached to the lateral annulus (Figure C, red arrow), the flail segment (Figure C [black arrow], Video 2), and the associated MR (Figure D, Video 3).
Treatment options were discussed at a multidisciplinary team meeting. Despite reasonable low surgical risk for reoperation, the patient declined the surgical procedure. He was subsequently offered mitral transcatheter edge-to-edge repair (TEER), which he accepted. Atrial transseptal puncture was performed superiorly and posteriorly under TOE supervision and guidance. Through the delivery sheath, a MitraClip (Abbott) was advanced into the left ventricle through the mitral ring after appropriate positioning (Figure E, Video 4). Alignment and perpendicularity were confirmed, and the leaflets were successfully grasped (Figure F, Video 5). TOE evaluation revealed adequate grasp of both mitral leaflets (Figure G, Video 6), mild residual MR (Figure H and I, Videos 7 and 8), improvement in systolic antegrade pulmonary vein Doppler velocities (Figure J), and a final gradient of 3 mm Hg.
The immediate post-procedure course was uneventful. The patient demonstrated significant clinical improvement, and a follow-up echocardiogram showed negligible residual MR.
While surgical MV repair remains the first-line option for severe symptomatic MR, this case suggests that TEER can be a safe and feasible alternative for individuals with a previous MV repair.
Affiliations and Disclosures
Aref El Nasasra, MD1,2; Artyom Star, MD1,2; Sergio L. Kobal, MD1,2; Carlos Cafri, MD1,2; Hilmi Alnsasra, MD1,2
From the 1Department of Cardiology, Soroka University Medical Center, Beersheba, Israel; 2Ben Gurion University of the Negev, Beersheba, Israel.
Dr El Nasasra and Dr Star contributed equally to this work and are designated as co-first authors.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that the patient gave informed consent for the intervention described in the manuscript and authorized the publication of the data.
Data availability statement:
All the data relevant to this case report are included in the manuscript. Additional details or imaging can be made available upon request to the corresponding author.
Address for correspondence: Hilmi Alnsasra, MD, Department of Cardiology, Soroka University Medical Center, Beersheba, Israel; Ben Gurion University of the Negev, Beersheba, Israel. Email: h.alnsasra@gmail.com










